








HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
CPT Code 00400 covers anesthesia for procedures on the integumentary system of the extremities, anterior trunk, and perineum when no more specific anesthesia code applies.
Reimbursement is calculated using base units plus time units, multiplied by the anesthesia conversion factor; base units for 00400 are set at 3 by the ASA.
Physical status modifiers (P1–P6) and qualifying circumstance codes (99100–99140) are required additions that directly affect payment; omitting them is a common source of claim errors.
Pabau’s claims management software helps anesthesia practices submit 00400 claims with the correct modifiers, reducing denials and shortening the revenue cycle.
CPT code 00400 covers anesthesia for procedures on the integumentary system of the extremities, anterior trunk, and perineum, used when no more specific anesthesia code applies. The ASA assigns it 3 base units, and reimbursement equals (base units + time units) multiplied by the anesthesia conversion factor.
As maintained by the American Medical Association (AMA), CPT Code 00400 falls within the 00400-00474 range for anesthesia services related to procedures on the integumentary system. Within that range, 00400 specifically addresses the integumentary system—meaning the skin and its appendages—across three anatomical regions: the extremities, anterior trunk, and perineum.
The “not elsewhere classified” logic matters here. If a more specific anesthesia code covers the exact procedure and site, that code takes precedence. CPT Code 00400 is the appropriate catch-all when specificity is not available in the CPT code set.
Anesthesia billing uses a different payment formula from standard procedure codes. Understanding this formula is essential before submitting any 00400 claim.
The formula is: (Base Units + Time Units + Modifying Units) x Anesthesia Conversion Factor = Reimbursement
The American Society of Anesthesiologists (ASA) assigns base units to every anesthesia CPT code to reflect the relative complexity of the service. CPT Code 00400 carries a base unit value of 3. These base units remain constant regardless of how long the procedure takes.
Time units are added based on the duration of anesthesia care. Medicare and most commercial payers use a 15-minute increment, meaning every 15 minutes of anesthesia time equals 1 time unit. Some payers use different increments, so checking payer-specific policy before submitting is advisable.
The conversion factor is a dollar amount that translates unit totals into a payment figure. Medicare publishes its anesthesia conversion factor annually. For 2026 rates, use the CMS Physician Fee Schedule lookup to verify current values by locality. Commercial payer rates vary significantly from Medicare and are governed by individual contracts.
Submitting CPT Code 00400 without the correct modifiers almost guarantees a denial or underpayment. Two modifier categories apply to every 00400 claim: physical status modifiers and provider-type modifiers. Qualifying circumstance codes are an additional consideration for specific patient populations.
Physical status modifiers reflect the patient’s health condition at the time of anesthesia. The clinical determination belongs to the anesthesia provider, not the billing team.
For a straightforward laceration repair on a healthy adult, the correct modifier is P1. Medicare does not reimburse additional modifying units for P1 or P2, but the modifier must still appear on the claim. Omitting it triggers an edit that delays payment.
The provider delivering anesthesia services determines which modifier set applies. Misreporting the supervision arrangement is a compliance risk, not just a billing inconvenience.
These modifiers reflect actual supervision arrangements in place during the procedure. Billing QX when the CRNA operated without direction, or AA when the anesthesiologist supervised rather than personally performed, creates a false claim risk. Document the care arrangement in the anesthetic record before the claim goes out.
The G8 modifier applies to CPT Code 00400 when the service is delivered as Monitored Anesthesia Care (MAC) for a deep, complex, or markedly invasive procedure. Per CMS Article A57361, 00400 is explicitly listed among the codes eligible for the G8 modifier. MAC claims for 00400 without G8 where the procedure qualifies will not reflect the correct complexity of care provided.
These add-on codes report unusual conditions that affect the risk of anesthesia. They are billed in addition to 00400, not as replacements.
Before submitting any 00400 claim, run a modifier checklist: (1) physical status modifier assigned by the anesthesia provider, (2) provider-type modifier reflecting the actual supervision arrangement, (3) G8 appended if MAC is documented for a qualifying procedure, (4) qualifying circumstance code added if patient age or clinical conditions apply.
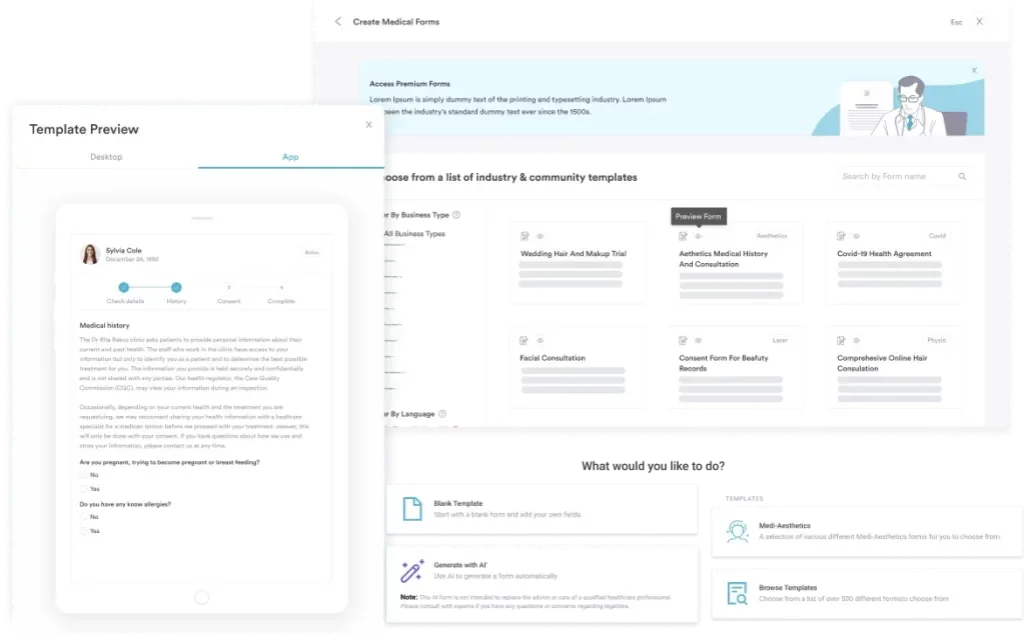
Anesthesia claims are among the most scrutinized in any payer audit. The anesthetic record is the foundation of every 00400 claim; incomplete documentation is the primary reason clean claims become contested.
Using digital anesthesia record forms reduces transcription errors and ensures all required fields are captured before the claim is submitted. Consistent documentation structure also makes it faster to respond to payer requests for records. Review your practice’s CPT billing documentation standards across all anesthesia codes, not just 00400, to keep the entire billing workflow consistent.
Payers cross-reference the operative report against the anesthesia code. If the operative report documents a procedure in the abdominal cavity rather than on the integumentary surface of the anterior trunk, 00400 will not survive a review. Maintaining HIPAA-compliant billing workflows means every record produced during the case supports the code on the claim.
Practices performing procedures such as skin substitute graft add-on procedures should verify that the anesthesia code selected aligns with the documented surgical depth.
Pabau's claims management software helps anesthesia and surgical practices submit 00400 claims with the correct modifiers attached, monitor claim status in real time, and respond to payer requests with documentation already in the system. Fewer denials, shorter payment cycles.

Knowing the code and its modifiers is necessary but not sufficient. The billing guidelines that govern how 00400 is submitted, bundled, and audited determine whether claims actually pay.
UnitedHealthcare’s commercial anesthesia reimbursement policy bundles HCPCS code G0516 into CPT Code 00400. When G0516 is present on a claim alongside 00400, UHC treats the anesthesia as already included in the G0516 payment. Billing both results in a denial of the 00400 line. Coders handling UHC claims should verify the current bundling table in the UHC provider reimbursement policy before submitting.
For plastic surgery practices and dermatology settings where 00400 appears frequently alongside skin excision and reconstruction procedures, establishing a claim edit protocol that checks each of these error categories before submission significantly reduces rework.
Coders should also be familiar with paring or cutting of benign hyperkeratotic lesions and similar integumentary codes that may appear on the same claim. Medical practice compliance considerations extend to anesthesia billing accuracy, not just clinical documentation.
Code selection depends on reading the operative report carefully and matching the procedure and site to the most specific code available. CPT Code 00400 is the default when no other code fits, but several adjacent codes exist for related procedures.
The distinction between 00400 and 00402 is one of the most frequently contested in anesthesia audits. A breast excision biopsy (skin and subcutaneous tissue only) may appropriately use 00400. A breast reconstruction or implant procedure uses 00402. The operative report’s documented intent and anatomical depth determine the correct code.
Review the AAPC Codify CPT code range for the full 00400-00474 range descriptions to verify adjacent code selection. Compare reimbursement levels across related codes when evaluating claim accuracy. For practices that also bill skin graft procedures across multiple service lines, a code crosswalk review reduces the risk of selecting 00400 when a more specific code applies.
Audit a sample of your 00400 claims quarterly. Pull the corresponding operative reports and confirm the documented procedure and site match the integumentary system of the extremities, anterior trunk, or perineum. If claims are clustering on breast or chest wall procedures, verify whether 00402, 00404, or 00406 should have been billed instead. Catching this internally is far less costly than finding it during a payer audit.
Manual anesthesia billing produces two recurring problems: modifier omissions and incomplete documentation. Both are avoidable with the right system.
Pabau’s claims management software gives anesthesia and surgical practices a structured workflow for submitting 00400 claims with modifiers attached at the point of claim creation.
Physical status modifiers, provider-type modifiers, and G8 can be configured as required fields, preventing a claim from advancing without them. The anesthetic record links directly to the claim, so documentation is available inside the same system when payers request supporting records.
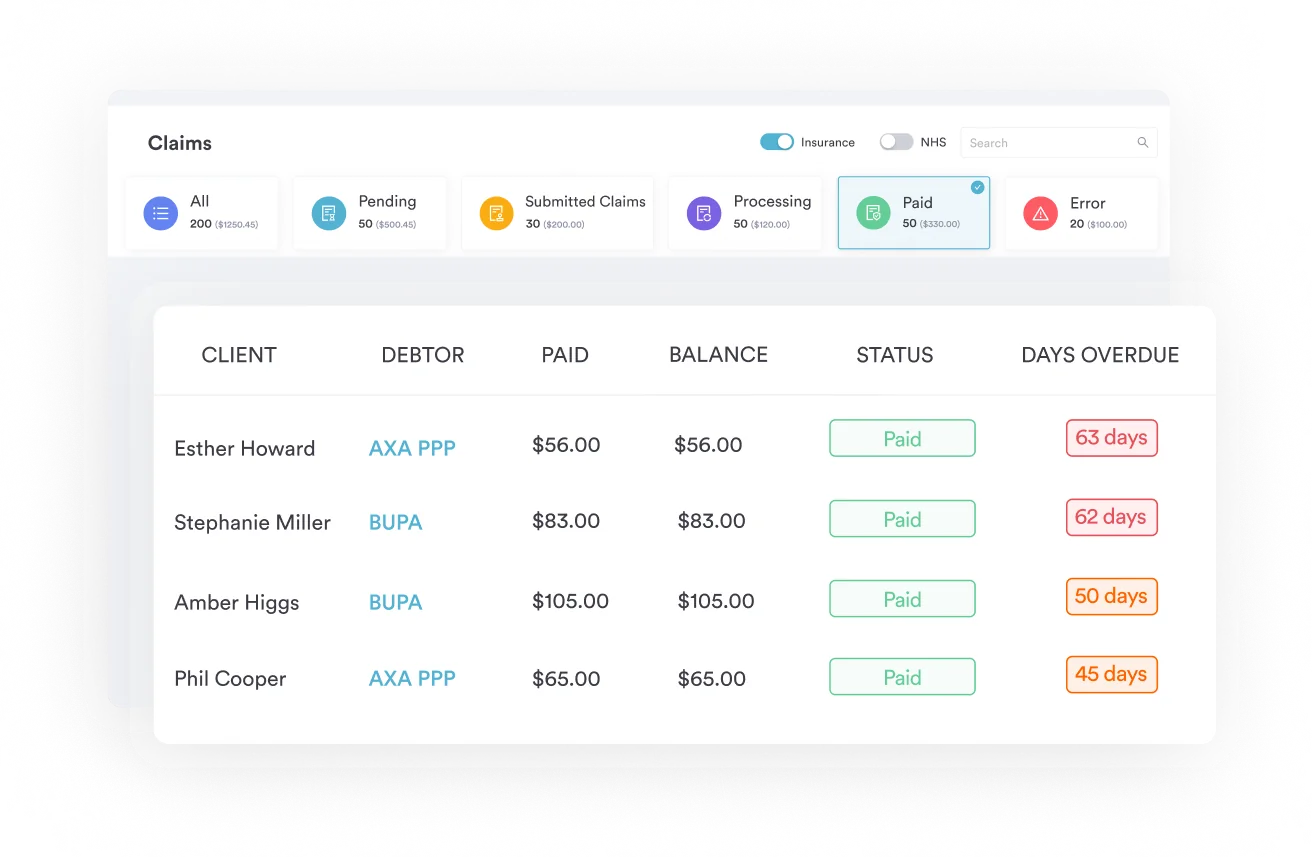
Automated billing workflows flag claims missing required modifiers or carrying diagnosis codes inconsistent with the procedure, catching errors before submission rather than after denial.
Review your HIPAA compliance for medical offices framework alongside your billing system selection to ensure documentation stored within the platform meets federal standards. Practices that bill Mohs surgery or other skin-based procedures alongside anesthesia should also ensure their modifier workflows cover those codes.
CPT Code 00400 is a technically straightforward code with significant compliance complexity underneath it. Related integumentary procedures such as CT thorax imaging may appear in the same patient encounter and require separate, accurate coding alongside the anesthesia claim.
Base unit values, time calculations, physical status modifiers, provider-type modifiers, G8 applicability, and documentation requirements all interact on every claim. Getting any element wrong costs time in denial management and risks underpayment or overpayment exposure.
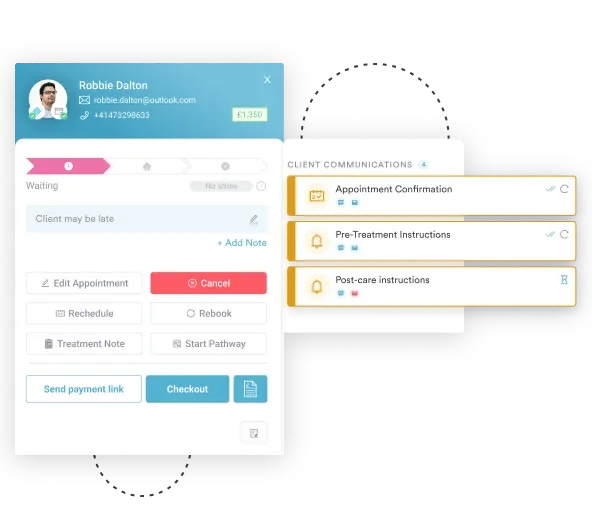
Pabau’s claims management software reduces that complexity by enforcing modifier rules and linking documentation to claims in one workflow. Practices managing pre-operative antibiotic prophylaxis reporting alongside anesthesia claims will find that a unified billing workflow reduces errors across both code sets. To see how it handles anesthesia billing in practice, book a demo with the Pabau team.
Need a structured approach to claims billing compliance? HIPAA compliance checklist for primary care covers the documentation and billing standards that apply to any medical practice handling protected health information.
Looking for software built for specialty practices? Dermatology practice management software shows how specialty practices manage procedure billing, patient records, and compliance in one system.
Want to reduce administrative overhead across your billing workflow? Features that save private practices time covers the automation tools that reduce manual billing steps and documentation rework.
CPT code 00400 covers anesthesia services for procedures on the integumentary system of the extremities, anterior trunk, and perineum when no more specific anesthesia code applies. Common examples include laceration repair on a finger, skin excision on the anterior trunk, and integumentary procedures in the perineal region.
CPT code 00400 requires a physical status modifier (P1–P6) and a provider-type modifier on every claim. Provider-type modifiers include AA for a personally performing anesthesiologist, QK for medical direction of multiple CRNAs, QX for a CRNA under physician direction, QY for medical direction of one CRNA, and QZ for a CRNA without physician direction. The G8 modifier applies when MAC is provided for a qualifying complex procedure. Qualifying circumstance codes (99100–99140) are added when patient age or clinical conditions elevate anesthesia risk.
Reimbursement equals (Base Units + Time Units + Modifying Units) multiplied by the anesthesia conversion factor. CPT code 00400 carries 3 ASA base units. Time units are typically calculated at 1 unit per 15 minutes under Medicare. The conversion factor varies by geographic locality and payer. Commercial payer rates differ from Medicare and are contract-specific.
CPT code 00400 applies to anesthesia for integumentary system procedures on the extremities, anterior trunk, and perineum when no more specific code applies. CPT code 00402 applies specifically to reconstructive procedures on the breast, such as augmentation, reduction, or reconstruction. A breast excision biopsy limited to skin and subcutaneous tissue may use 00400; a breast reconstruction uses 00402. The operative report’s documented procedure type and anatomical depth determine the correct code.
Required documentation includes a pre-anesthesia evaluation with physical status classification, informed consent, a complete intraoperative anesthetic record showing continuous monitoring data and drug administration, a post-anesthesia note, and an operative report that corresponds to an integumentary procedure at the anatomical site covered by 00400. An ICD-10-CM diagnosis code reflecting the condition requiring the procedure must also accompany the claim.



