HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
CPT code 00148 describes anesthesia for procedures on the eye; ophthalmoscopy, covering eye examinations requiring sedation or general anesthesia.
00148 carries 4 base units, confirmed across CMS, VA, Massachusetts Medicaid, and NY eMedNY fee schedules.
Modifier AA is required when an anesthesiologist personally performs the service; modifiers QK, QX, QY, and QZ apply to medically directed or supervised CRNA arrangements.
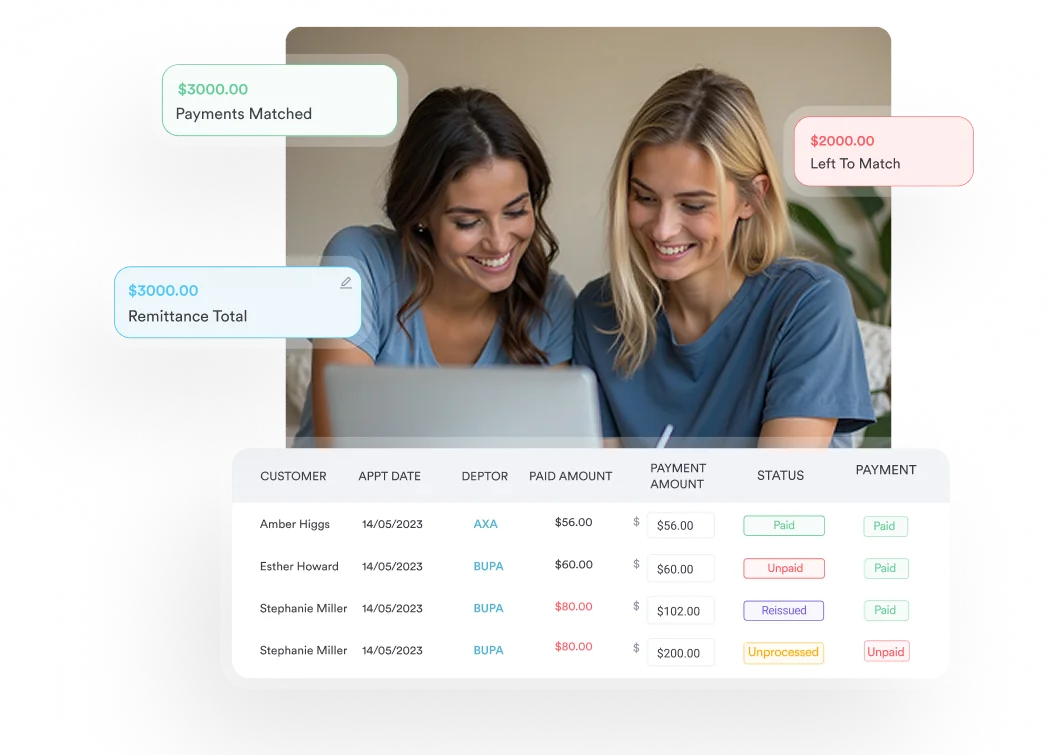
Pabau’s claims management software helps anesthesia billing teams attach the correct modifiers, link supporting ICD-10 codes, and track claims through to payment.
CPT code 00148 is the anesthesia procedure code for ophthalmoscopy. It is the code for an eye exam under anesthesia, billed when a patient needs sedation or general anesthesia to complete the examination. Pediatric patients, adults with cognitive impairment, and patients with extreme exam anxiety are the most common candidates, since they frequently cannot hold still for a standard exam.
A routine, unsedated eye exam is instead billed under CPT code 92002.
The full official description, as maintained by the American Medical Association (AMA), is: Anesthesia for procedures on eye; ophthalmoscopy. It falls within the CPT range 00100 through 00222, which covers anesthesia for procedures on the head.
Unlike adjacent codes in the eye-procedure cluster, CPT code 00148 is specific to ophthalmoscopy rather than surgical intervention on the globe or its structures. Lens surgery uses CPT code 00142. Corneal transplant uses CPT 00144. Vitreoretinal surgery uses CPT 00145. CPT code 00148 stays in its own lane: the diagnostic eye examination performed under anesthesia, often documented in the chart as an examination under anesthesia (EUA).
Anesthesia providers billing this code should also confirm that the underlying ophthalmoscopy procedure has been documented as medically necessary. Payers require a clear link between the anesthesia service and a covered eye examination, not merely an assertion that the patient was anxious. The ICD-10-CM diagnosis code on the claim does that linking work.
CPT code 00148 carries 4 base units, confirmed across multiple payer and government sources including the VA Table H, Massachusetts Medicaid, and NY eMedNY. Base units are a fixed value the AMA assigns to each anesthesia code based on procedural complexity. They represent the starting point for calculating total anesthesia reimbursement, before time is added.
Anesthesia reimbursement uses a formula that differs from standard RVU-based physician fee schedules. The calculation is:
Total reimbursement = (B + T + M) x CF. For a 30-minute ophthalmoscopy under Medicare, that would be (4 + 2 + 0) x CF, where CF is the published Medicare anesthesia conversion factor for the provider’s locality.
Use the CMS Physician Fee Schedule lookup to find the current conversion factor for your location. Time should be recorded in the anesthesia record and carried directly to the claim.
Ophthalmoscopy cases frequently involve patients who qualify for add-on circumstance codes. Code 99100 (anesthesia for patients under 1 year of age or over 70) adds 1 unit. Code 99140 (emergency conditions) adds 2 units. These are appended to the claim alongside CPT code 00148, not substituted for it. Document the qualifying factor in the anesthesia record to support the add-on.
Modifier selection for CPT code 00148 follows the same rules as any anesthesia CPT code. The modifier communicates who provided the anesthesia service and whether physician direction of a CRNA was involved. Payers use these to determine whether the full fee or a reduced rate applies.
For ophthalmoscopy cases billed under CPT code 00148, MAC arrangements are common. Under MAC, the anesthesiologist is present and monitoring the patient throughout but may not be administering a general anesthetic.
The CMS Monitored Anesthesia Care article A57361 explicitly lists CPT code 00148 among the anesthesia codes supported for MAC billing. Verify that your claim pairs the correct MAC modifier with a diagnosis code that reflects the patient’s actual clinical picture, since the article’s own diagnosis list is a general medical-necessity list rather than an eye-specific one.
Run a modifier audit on your last 90 days of CPT code 00148 claims. Flag any claim where QK and QX are both present without documentation of all seven TEFRA conditions. This is one of the most common audit targets for anesthesia practices and a straightforward fix with the right workflow in place.
Every CPT code 00148 claim needs a paired ICD-10-CM diagnosis code that establishes why anesthesia was medically necessary for an eye examination. Without it, payers treat the claim as lacking medical necessity documentation and deny.
The table below covers the most commonly paired codes, grouped by clinical scenario. Corneal conditions such as H18.10 (bullous keratopathy) can also justify anesthesia-assisted examination when slit-lamp evaluation alone is not tolerated.
CMS MAC article A57361 is a general medical-necessity diagnosis list covering roughly 47 anesthesia codes; it lists systemic patient conditions rather than an eye-diagnosis-specific set. Of the codes in the table above, only F84.0 (autistic disorder) is confirmed on that list. Confirm coverage for the other diagnoses through the payer’s own eye-specific policy before submission.
For pediatric glaucoma and retinal cases, also consider pairing qualifying circumstance code 99100 when the patient is under 1 year of age. Reviewing ICD-10 code H35.9 alongside the retinopathy codes above helps billers select the most specific retinal diagnosis supported by documentation, rather than defaulting to an unspecified code.
Claims denied for medical necessity on CPT code 00148 almost always share a common problem: the ICD-10 code on the claim is too vague to justify anesthesia for a diagnostic procedure. An unspecified eye disorder code is harder to defend than a specific diagnosis tied to a documented clinical finding.
For example, H26.8 (other specified cataract) supports medical necessity more clearly than the unspecified H26.9 code when documentation supports the more specific diagnosis.
Ophthalmologists and referring physicians should document the specific reason anesthesia was required, not just the eye condition being evaluated. That documentation becomes the basis for the ICD-10 code selection.
Pabau gives anesthesia billing teams a single workflow for attaching modifiers, linking ICD-10 codes, and tracking CPT code 00148 claims through to payment. No chasing EOBs across separate systems.

Reimbursement for CPT code 00148 varies by payer, locality, and arrangement type; no single dollar figure applies universally. Understanding the variables that move the number helps practices forecast revenue and catch underpayments early.
For practices with anesthesia claims management workflows, tracking CPT code 00148 reimbursement at the payer level, not just the aggregate, is the fastest way to identify a contract that is systematically underpaying.
A single payer paying below the contracted rate across dozens of small ophthalmoscopy claims adds up to meaningful lost revenue. Pabau’s reporting tools let billing teams pull this data without a manual export.
Practices that also bill procedure codes across other specialties will find the same tracking logic applies. Reviewing your reimbursement pattern for CPT codes for IVF procedures or CPT codes for coaching procedures uses the same payer-by-payer analysis that catches underpayments on anesthesia codes.
Request an EOB breakdown from your top three payers on CPT code 00148 claims over the last 12 months. Compare the paid conversion factor against your contracted rate. If the paid rate is consistently lower, that is a contract dispute, not a coding error, and it should be escalated through your payer relations contact rather than a rebill.
Getting CPT code 00148 paid on the first submission requires documentation that covers three areas: clinical justification for anesthesia, service delivery confirmation, and accurate modifier assignment. Missing any one of these triggers a denial or a request for additional documentation that delays payment by weeks.
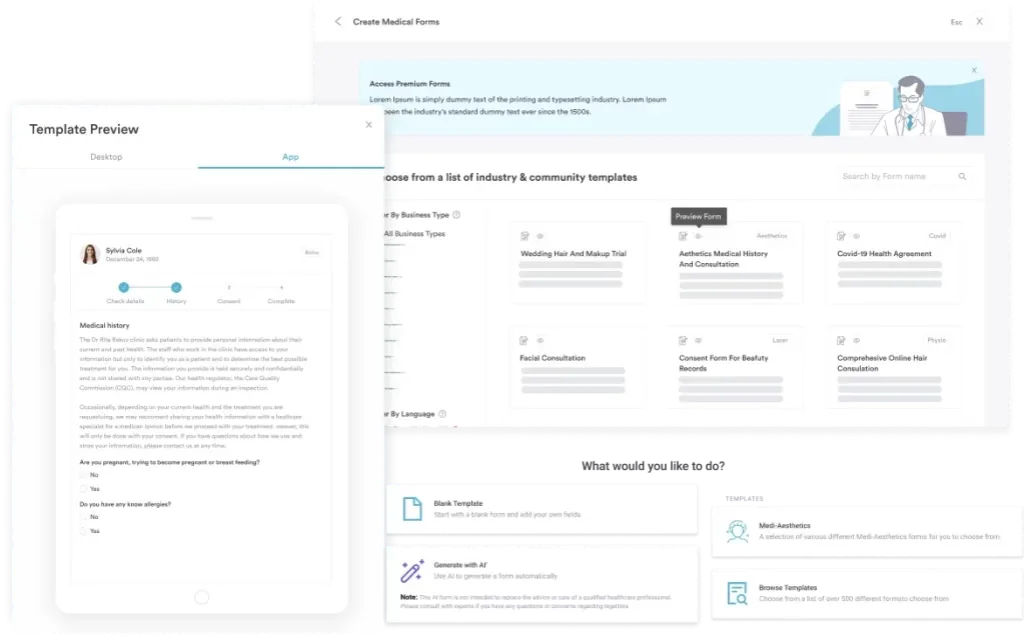
Practices using digital documentation forms reduce the risk of incomplete anesthesia records. A pre-built anesthesia template prompts providers to capture every required field before the patient leaves the recovery area, so the billing team receives a complete record rather than chasing down missing time entries the next morning.
Maintaining HIPAA compliance for medical offices in how those records are stored and transmitted is an additional requirement that applies to every claim workflow.
Anesthesia billing teams working across multiple specialties also benefit from reviewing how CPT coding workflows apply in adjacent areas. The same documentation discipline required for CPT code 00148 applies to ADHD screening CPT codes and other anesthesia procedure types, such as CPT code 00126 for tympanotomy, where medical necessity documentation drives payer decisions.
Understanding how situational anxiety ICD-10 coding works also helps billers who encounter patients with anxiety-related reasons for requiring anesthesia during an eye exam.
CPT code 00148 sits within a cluster of eye-procedure anesthesia codes. Using the correct code for the specific procedure performed is not optional. Upcoding to a higher-complexity code (and its associated higher base units) is an audit risk. Downcoding misrepresents the service delivered. The table below clarifies which code applies to which procedure.
CPT code 00148 shares the lowest base-unit count in this cluster, tied with 00142 and 00147, because ophthalmoscopy is a diagnostic examination rather than a surgical intervention. When a patient undergoes both an examination under anesthesia and a surgical procedure on the same date of service, the surgical anesthesia code typically takes precedence.
Bill the higher-complexity code for the primary procedure; do not stack CPT code 00148 on top of a surgical anesthesia code for the same encounter. The AAPC Codify CPT lookup provides current modifier and crosswalk data for each code in this range. Also refer to the AMA’s CPT coding resources for the most current code descriptions and annual updates.
Billers managing multi-specialty practices also benefit from resources covering adjacent diagnosis code families. Understanding how disorders of the iris and ciliary body are coded is relevant when a patient scheduled for iridectomy (CPT code 00147) also needs an anesthesia-assisted eye exam captured under CPT code 00148 during the same visit.
CPT code 00148 is a low-complexity anesthesia code with a straightforward description, but the billing errors that generate denials on these claims are preventable. Most come down to the same three problems: wrong modifier for the provider arrangement, ICD-10 code that does not satisfy medical necessity criteria, and time documentation that does not match the minutes billed.
Each of these is a documentation discipline issue, not a matter of coding knowledge.
Pabau’s claims management software gives anesthesia practices the workflow structure to catch these issues before submission, not after a denial. If your team is ready to reduce rework on anesthesia claims and see cleaner first-pass rates across CPT code 00148 and related eye-procedure codes, book a demo to see how Pabau handles this end to end.
Need a structured billing workflow for other CPT code families? IVF CPT codes covers the full coding and documentation framework for fertility procedure billing.
Working across specialties with different ICD-10 needs? Situational anxiety ICD-10 coding explains how anxiety diagnoses pair with procedure codes when patients require additional clinical support during examinations.
Exploring how practice management software supports claims workflows? Practice management software walks through how integrated billing, scheduling, and documentation tools reduce claim errors across specialties.
CPT code 00148 is the anesthesia procedure code for ophthalmoscopy, described officially as “Anesthesia for procedures on eye; ophthalmoscopy.” It is used when a patient requires sedation or general anesthesia to undergo a diagnostic eye examination, and it carries 4 base units as assigned by the American Medical Association.
CPT code 00148 has 4 base units. This value is confirmed across the VA Table H, Massachusetts Medicaid, NY eMedNY, and other federal and state fee schedules. Base units are fixed by the AMA and do not vary by geography or payer.
Modifier AA applies when an anesthesiologist personally performs the service. QK and QX are used together for medically directed CRNA arrangements. QY applies to medical direction of a single CRNA. QZ is used when a CRNA bills without physician direction, and under Medicare Part B it is reimbursed at 100% of the anesthesia fee schedule, the same as AA. The MAC-specific modifier G9 (monitored anesthesia care for a patient with a history of severe cardio-pulmonary disease) also applies to CPT code 00148; G8 does not, since CMS MAC article A57361 restricts it to CPT codes 00100, 00300, 00400, 00160, 00532, and 00920.
Commonly paired ICD-10-CM codes include H35.00 (unspecified background retinopathy), H40.10X0 (unspecified open-angle glaucoma), H50.00 (unspecified esotropia), F84.0 (autistic disorder), and Z13.5 (encounter for screening for eye disorders). CMS MAC article A57361 is a general medical-necessity diagnosis list covering roughly 47 anesthesia codes, not an eye-diagnosis-specific list; of the codes above, only F84.0 is confirmed on that list. Confirm coverage for the others through the payer’s own policy before submission.
Reimbursement uses the formula (Base Units + Time Units + Qualifying Circumstance Units) x Conversion Factor. For CPT code 00148, base units are 4. Time units are calculated at 1 unit per 15 minutes under Medicare, though some commercial payers use 10-minute increments. The conversion factor varies by payer and location; use the CMS Physician Fee Schedule lookup to find the current Medicare rate for your locality.
The CPT code for an eye exam under anesthesia is 00148 when the procedure is an ophthalmoscopy. It applies to a diagnostic examination under anesthesia (EUA) rather than surgery on the eye, and it carries 4 base units. If the eye examination accompanies a surgical procedure on the same date, the anesthesia code for that surgery is billed instead.