








CPT code 17312: Mohs surgery add-on stage billing guide
CPT 17312 bills each Mohs stage after the first on the head, neck, hands, feet, ...
Last Updated: August 4, 2026
CPT code 00534 describes anesthesia for transvenous insertion or replacement of a pacing cardioverter-defibrillator (ICD device)
00534 carries 7 anesthesia base units, confirmed across VA, Pennsylvania, Massachusetts, and Arizona fee schedules
Applicable modifiers include AA, QK, QX, QY, QZ, AD, and qualifying circumstance codes 99100-99140. Failing to append the correct modifier is a leading cause of claim denial
Practice management software like Pabau helps anesthesia billing teams track time units, attach modifiers, and reduce documentation errors before submission
CPT code 00534 is anesthesia for transvenous insertion or replacement of a pacing cardioverter-defibrillator (ICD), carrying 7 base units under the ASA Relative Value Guide. It sits within the Anesthesia for Intrathoracic Procedures range and applies only to transvenous, vein-based lead placement rather than open-chest device implantation.
CPT code 00534 is one of the more frequently misapplied anesthesia codes in cardiac electrophysiology billing. Coders confuse it with adjacent codes covering pacemaker insertion (00530) and cardiac electrophysiology studies (00537), and that confusion costs practices revenue through denials and downcoded claims.
The official descriptor for CPT code 00534 is: Anesthesia for transvenous insertion or replacement of pacing cardioverter-defibrillator. As of January 1, 2026, the short descriptor was updated per FindACode. Confirm the exact wording against the AMA CPT code set for your billing year.
The code falls within the Anesthesia for Intrathoracic Procedures range and is classified as HCPCS Level I under Current Procedural Terminology maintained by the American Medical Association (AMA).
This code applies specifically to transvenous approaches, where leads are threaded through a vein to reach the heart. It covers both initial device insertion and replacement procedures. Open-chest device implantation uses a different code set.
Anesthesia reimbursement is calculated differently from most CPT codes. Rather than a flat fee, payment is based on a formula: (Base Units + Time Units + Qualifying Circumstance Units) multiplied by the payer’s conversion factor.
CPT code 00534 carries 7 base units, as established by the American Society of Anesthesiologists (ASA) Relative Value Guide and confirmed independently across four government sources: the VA Community Care outpatient data tables, Pennsylvania DHS, Massachusetts MassHealth, and Arizona Industrial Commission fee schedules.
Time units are calculated at one unit per 15 minutes of anesthesia time, beginning when the anesthesia provider starts preparing the patient and ending when the provider is no longer in attendance.
Accurate time documentation is critical: payers audit anesthesia records, and underdocumented time is a top denial driver. See the CMS Physician Fee Schedule for current Medicare conversion factor values by locality.
Track anesthesia start and stop times in your clinical notes at the exact minute, not rounded to the nearest quarter-hour. Even a two-minute discrepancy between the anesthesia record and the operative note can trigger a medical necessity review or reduce reimbursement by a full time unit.
Modifier selection for CPT code 00534 depends on who is delivering the anesthesia and under what supervisory arrangement. Getting this wrong is among the most expensive coding errors in anesthesia billing.
For Medicare claims, the medical direction rules are strict. Under the AD modifier, the physician is limited to three base units per case. Under QK, the physician must document seven specific requirements in the medical record, including pre-anesthesia evaluation and presence at induction.
Missing any of these requirements converts a medically directed case to a supervision case, reducing reimbursement significantly. For guidance on clinical documentation compliance across your practice, ensure your records meet payer audit standards.
Physical status modifiers are not payable by Medicare but are required by many commercial payers and the ASA. They describe the patient’s pre-anesthesia health status and affect reimbursement under some payer contracts.
For patients undergoing ICD insertion or replacement, P3 and P4 are most common given the underlying cardiac conditions requiring device therapy. Check your commercial payer contracts for how physical status modifiers affect the reimbursement calculation.
Qualifying circumstance codes are add-on codes that report anesthesia conditions that significantly affect the character and complexity of the service. They can be appended to CPT code 00534 when applicable, adding base units to the claim. The same add-on logic applies to qualifying circumstance codes used with IVF CPT codes and other anesthesia-adjacent procedures.
Not all payers accept qualifying circumstance codes. Medicare, for example, does not recognize 99100-99140 as separately reimbursable add-ons in the same way commercial payers do. Always verify with the specific payer before appending these codes.
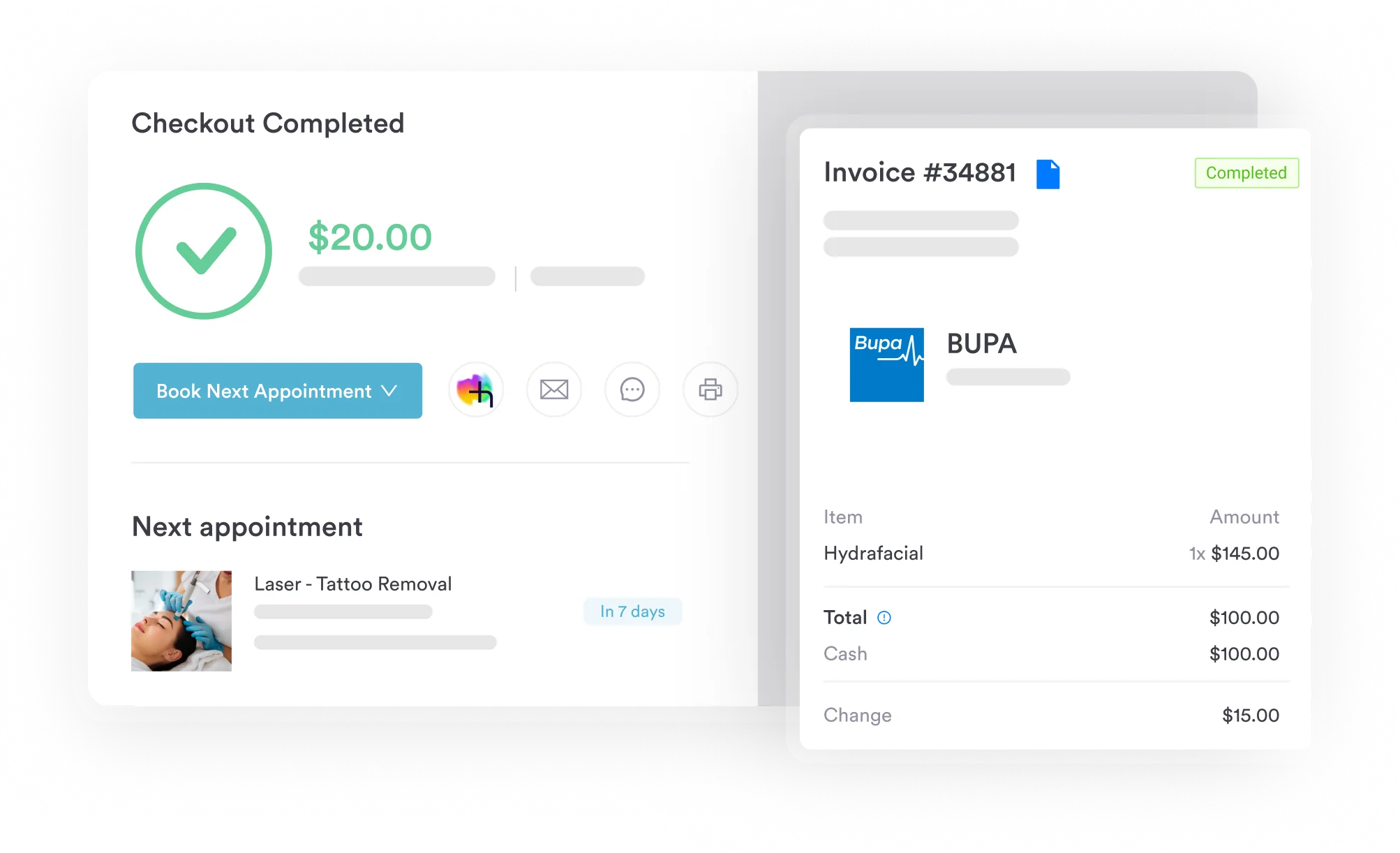
Pabau's claims management tools help anesthesia and cardiac surgery practices track time units, attach modifiers correctly, and submit cleaner claims the first time. See how it works for your team.

Every CPT code 00534 claim needs supporting documentation that demonstrates medical necessity, provider qualification, and accurate time reporting. Inadequate records are the second most common reason for anesthesia claim denials after incorrect modifier use.
Your anesthesia record should capture all of the following before the claim is submitted. Use digital anesthesia documentation forms to standardize data capture and reduce omissions across your practice.
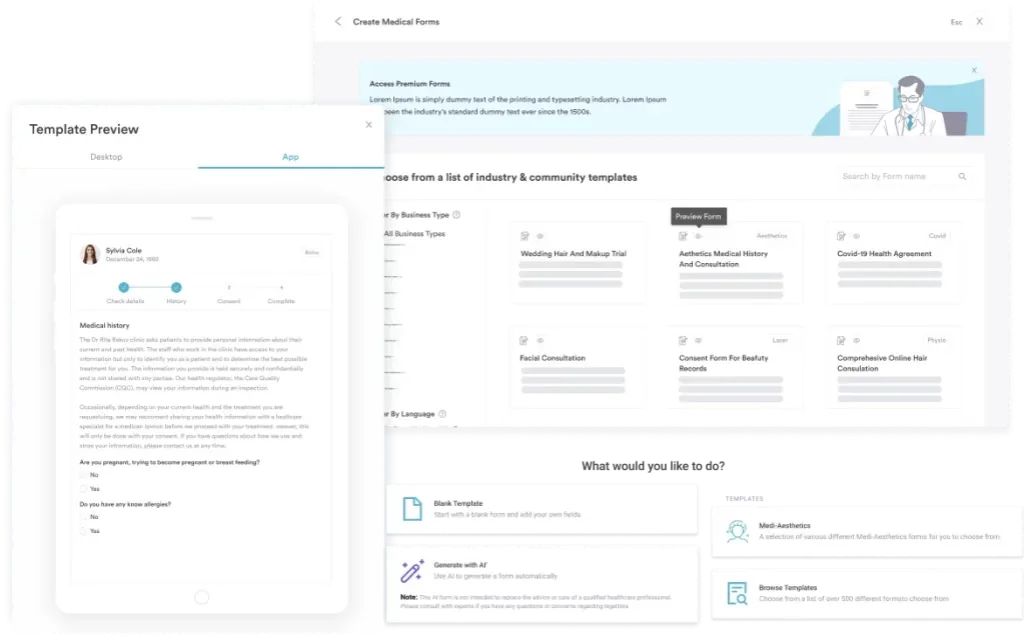
The clinical records system must preserve all of these elements in a retrievable, timestamped format. Payers conducting post-payment audits will request the full anesthesia record. Incomplete documentation results in recoupment demands. Practices can also benefit from standardized medical forms across the practice to ensure consistent capture of required data fields.
Anesthesia reimbursement for CPT code 00534 varies by payer, geographic locality, and year. No single national rate applies universally. The formula is consistent, but the conversion factor differs by payer and is updated annually.
Reimbursement formula: (Base Units + Time Units + QC Units) x Conversion Factor = Payment
With 7 base units and a typical 60-minute procedure generating 4 time units (at 15 min/unit), a base calculation before qualifying circumstances would yield 11 units multiplied by the payer’s conversion factor. For Medicare, conversion factors vary by locality and are updated each calendar year through the Physician Fee Schedule.
As a historical reference, Arizona’s Industrial Commission 2020-2021 fee schedule listed $427.00 for 00534 (7 base units at the state conversion factor at that time). Current rates will differ. For commercial payers, negotiated rates in your payer contracts govern reimbursement. Always verify current rates through your payer portals rather than relying on historical state documents.
Run a quarterly review of your top anesthesia CPT codes against your ERA (Explanation of Remittance Advice) data. Compare expected units times your payer’s conversion factor against actual payments. A consistent shortfall on 00534 claims often points to modifier mismatches or time-unit rounding errors that your billing team can correct prospectively.
Selecting the wrong code from the intrathoracic anesthesia range is a common upcoding or downcoding risk. CPT code 00534 has specific neighbors that coders must distinguish carefully, and the same discipline applies to other anesthesia codes like 01962 and 00938.
The distinction between 00530 and 00534 is clinically significant. A pacemaker implant (00530, 4 base units) is a different device and procedure than a cardioverter-defibrillator implant (00534, 7 base units). Billing 00530 for an ICD implant understates the complexity and reduces reimbursement. Billing 00534 for a standard pacemaker overstates complexity and creates an audit risk.
Every anesthesia claim requires a supporting ICD-10-CM diagnosis code that establishes medical necessity for the procedure. The diagnosis must match the clinical reason for the ICD device implant or replacement, cross-referenced against the device’s own billing code, C1721, and distinguished from adjacent procedures like anesthesia for arrhythmia conversion under 00410.
For replacement procedures, Z45.02 is the appropriate primary diagnosis. For initial insertions driven by arrhythmia or cardiomyopathy, the primary cardiac diagnosis drives medical necessity. Check the AAPC Codify CPT lookup for current crosswalk guidance linking CPT 00534 to its most common diagnosis pairings.
Understanding the denial patterns specific to CPT code 00534, and to codes like 11046, lets billing teams intercept problems before submission rather than working rejections after the fact. Sound medical billing workflow planning builds denial prevention into the claim-preparation process.
Per the Pennsylvania DHS Physician Procedure Codes document (a state source — CMS guidelines govern at the federal level), 00534 is billed in the following settings:
Practices using anesthesia claims management software can automate modifier checks and flag missing documentation before the claim reaches the payer. This is especially useful for high-volume anesthesia groups where manual review of every case is not feasible.
Anesthesia billing for codes like CPT code 00534 involves multiple moving parts: capturing accurate time, selecting the right modifier based on the care arrangement, pairing the correct ICD-10 diagnosis, and verifying payer-specific rules before submission. Manual processes introduce errors at every step.
Pabau brings these billing steps together in one connected workflow, reducing the manual reconciliation burden on billing teams. Structured practice management software that connects clinical documentation to billing reduces the lag between service delivery and claim submission, which affects both cash flow and audit readiness.
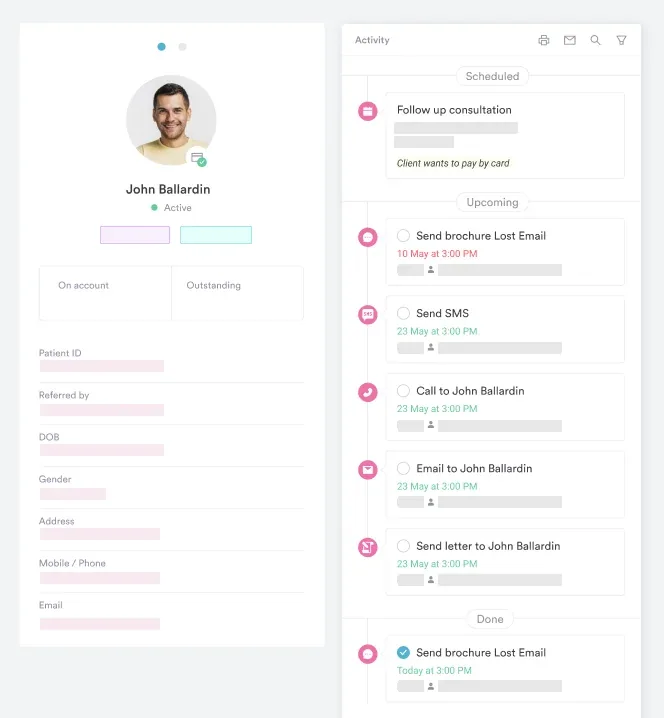
Anesthesia providers can also use Pabau’s structured note templates to ensure required documentation elements (start/stop times, physical status, medical direction criteria) are captured at the point of care rather than reconstructed after the fact.
The same connected workflow extends to other specialty practices with similarly detailed, time-based billing. IV therapy practices and physical therapy clinics track comparable documentation and modifier requirements, and benefit from the same connected record-to-claim workflow.
CPT code 00534 is a seven-base-unit anesthesia code for transvenous ICD insertion and replacement procedures. The most common billing failures involve modifier mismatches between the physician and CRNA arrangement, underdocumented anesthesia time, and misidentifying the procedure as a simple pacemaker insertion (00530).
Clean claims for 00534 start with documentation precision at the point of care. Pabau’s claims management and digital forms tools help anesthesia practices capture the required fields, attach the correct modifiers, and submit cleaner first-pass claims. Book a demo to see how Pabau handles anesthesia billing workflows end to end.
Need base-unit and modifier rules for another orthopedic anesthesia case? 01712 covers anesthesia for upper arm tendon surgery and how its billing differs from cardiac device cases.
Coding anesthesia for a hip or femur procedure? 01220 breaks down anesthesia for closed procedures on the upper femur and its base-unit calculation.
Not sure what to do with a deleted anesthesia code on an old claim? 01180 explains what happened to the deleted code for obturator neurectomy and how to rebill affected claims.
CPT code 00534 is an anesthesia procedure code describing services for transvenous insertion or replacement of a pacing cardioverter-defibrillator (ICD). It carries 7 base units and falls within the Anesthesia for Intrathoracic Procedures code range maintained by the AMA.
CPT code 00534 has 7 base units, as confirmed by the VA Community Care outpatient data tables, Pennsylvania DHS, Massachusetts MassHealth, and Arizona Industrial Commission fee schedules. Base units are added to time units (one per 15 minutes) and any qualifying circumstance units before multiplying by the payer’s conversion factor.
The primary modifiers for 00534 are AA (physician anesthesiologist personally performing), QK (physician directing 2-4 CRNAs), QX (CRNA under physician direction), QY (physician directing one CRNA), QZ (independent CRNA without direction), and AD (physician supervising more than 4 concurrent cases). Physical status modifiers P1-P6 are also reportable and required by many commercial payers.
CPT 00530 covers anesthesia for pacemaker insertion and carries only 4 base units, while 00534 covers anesthesia for transvenous insertion or replacement of a pacing cardioverter-defibrillator and carries 7 base units. Using 00530 for an ICD procedure understates complexity and reduces reimbursement. Billing 00534 for a standard pacemaker insertion creates an upcoding risk.
Common ICD-10 pairings include I49.01 (ventricular fibrillation), I47.2 (ventricular tachycardia), I42.0 (dilated cardiomyopathy), I50.20 (systolic heart failure), and Z45.02 (encounter for adjustment of automatic implantable cardiac defibrillator) for replacement procedures. The diagnosis code must establish the medical necessity for ICD therapy.
Medicare generally does not separately reimburse qualifying circumstance codes (99100-99140) as add-ons in the same way commercial payers do. For commercial payer contracts, verify whether your specific contract allows qualifying circumstance add-ons before appending them to 00534 claims.



