HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
CPT code 00126 covers anesthesia for procedures on the external, middle, and inner ear, including biopsy and tympanotomy – maintained by the AMA under “Anesthesia for Procedures on the Head.”
Reimbursement is calculated using base units (4 base units for 00126) plus time units, multiplied by the anesthesia conversion factor – not standard work RVUs.
Modifier 99100 applies when the patient is under 1 year or over 70 years of age; ASA physical status modifiers (P1-P6) are required on every anesthesia claim.
Pabau’s claims management software helps anesthesia billing teams track modifier requirements, attach correct ICD-10 diagnosis codes, and reduce claim denials.
CPT code 00126 is the anesthesia billing code for procedures on the external, middle, and inner ear, including biopsy and tympanotomy. The American Medical Association maintains it within the CPT anesthesia code set, under the category “Anesthesia for Procedures on the Head.” Anesthesia billers, CRNAs, and practice managers in ENT and surgical settings bill it most often for pediatric ear tube placement.
Modifier errors, missing ASA physical status codes, and misdocumented provider roles drive most tympanotomy denials, not medical necessity disputes. All three are preventable with the right billing workflow.
The American Medical Association (AMA) maintains CPT code 00126 within the Current Procedural Terminology (CPT) code set, under the category “Anesthesia for Procedures on the Head.” This guide covers base unit calculation, applicable modifiers, documentation standards, related codes, and the most common billing errors to avoid.
For context on how CPT coding for specialty procedures works across practice settings, the coding logic here follows the same anesthesia billing framework used system-wide. For background on how anesthesia claims fit into the broader revenue cycle, see what is medical billing.
CPT code 00126 carries 4 anesthesia base units, as defined by the American Society of Anesthesiologists (ASA) Relative Value Guide (RVG). Unlike standard procedure codes reimbursed via work RVUs, anesthesia codes follow a different formula entirely.
Other anesthesia codes use the identical base-plus-time formula with different base unit values: CPT code 00148 for ophthalmoscopy, CPT code 00142 for lens surgery, and CPT code 01502 for lower leg embolectomy are three examples.
The reimbursement formula is:
Time units accrue at one unit per 15 minutes of anesthesia time. The conversion factor – expressed in dollars per unit – varies significantly by payer and geographic region. Medicare publishes its anesthesia conversion factor annually through the CMS Physician Fee Schedule.
Commercial payer rates are negotiated separately and often differ from the Medicare benchmark. Use the FastRVU 2026 RVU lookup to verify current base unit values and conversion factors by locality.
Because tympanotomy is a short procedure – typically 10 to 30 minutes – total anesthesia time units are low. At 15 minutes, a provider accrues 1 time unit, meaning the entire claim may total only 5 units (4 base + 1 time) before the conversion factor is applied.
Accurate time documentation is therefore critical: a few minutes’ discrepancy can affect reimbursement. The PCC free 2026 RVU/RBRVS calculator can help practices model expected reimbursement across different payer conversion factors.
Modifier selection is the most common source of claim denials for CPT code 00126. Every anesthesia claim requires an ASA physical status modifier. Additional modifiers apply based on patient age, provider type, and whether the procedure is repeated.
For most pediatric tympanotomy cases, P1 or P2 applies. The ASA physical status must be documented in the anesthesia record before the claim is submitted. Missing this modifier is a guaranteed denial for Medicare and most commercial payers. Pairing strong compliance management for anesthesia billing with your practice workflow reduces the rate of omitted modifiers significantly.
Modifier 99100 adds 1 qualifying circumstance unit to the claim when anesthesia is provided for a patient under 1 year of age or over 70 years of age. Because tympanotomy is performed predominantly on young children, modifier 99100 applies frequently in ENT practice settings.
The age threshold matters precisely. A 12-month-old does not qualify; an 11-month-old does. Document the patient’s date of birth and the procedure date in the anesthesia record. This documentation supports the modifier and protects against audit. For HIPAA-compliant documentation practices that support accurate age-based claims, review your HIPAA compliance for medical offices protocols alongside anesthesia record standards.
The billing split between medically directed and non-directed cases is one of the highest-risk areas in anesthesia billing. Submitting QZ when medical direction was actually provided – or vice versa – constitutes a billing error and can trigger audits. Confirm supervision arrangements before claim submission on every case.
Modifier 76 applies when anesthesia for the same ear procedure is repeated within the same episode of care by the same provider. This can occur when additional infection sites require treatment during the operative session. Append modifier 76 to CPT code 00126 on the second line of the claim to distinguish the repeat service from a duplicate billing error.
Incomplete anesthesia records are the second-leading cause of CPT code 00126 claim denials, behind modifier errors. CMS and the ASA both require specific documentation elements in every anesthesia record.
ICD-10 codes that commonly support medical necessity for CPT code 00126 include H65.x (non-suppurative otitis media), H66.x (suppurative otitis media), and H74.x (middle ear disorders).
Using digital anesthesia documentation forms that prompt for all required fields helps ensure completeness before records reach the billing team. ICD-10 code linkage between the diagnosis and the anesthesia claim clarifies how secondary diagnoses interact with primary procedure codes in anesthesia records.
Document anesthesia start time as the moment monitoring is established, not when the first agent is administered. CMS defines anesthesia time from the moment the anesthesiologist or CRNA begins preparing the patient for induction – earlier than many providers record. Earlier start times mean more time units, and more time units mean higher reimbursement.
Selecting the wrong anesthesia code is a separate but equally costly error. CPT codes 00120, 00124, and 00126 all cover ear anesthesia but apply in different scenarios, and the distinctions matter for correct billing. Durable medical equipment used in ear care, such as an ear mold or insert device, is billed separately under HCPCS and is not part of the anesthesia claim.
Pabau helps surgical and ENT practices manage anesthesia documentation, track modifier requirements, and submit cleaner claims. See how the workflow fits your team.

CPT code 00120 is the not-otherwise-specified (NOS) code for anesthesia on the external, middle, and inner ear, including biopsy – the same anatomical scope as CPT code 00126. The difference is specificity: 00120 is the generic catch-all used when no more precise code applies, while 00126 is the specific code for tympanotomy.
When the surgical procedure is tympanostomy tube placement, 00126 is the correct anesthesia code, not 00120. Using the NOS code when a more specific code exists is a mismatch that payers catch on edit review.
Focus code for this guide highlighted in teal.
A common point of confusion involves CPT 69433 and CPT 69436. These are the surgical procedure codes for tympanostomy tube placement, not anesthesia codes.
The surgical team bills 69433 or 69436; the anesthesia provider bills 00126. These are separate claims submitted by different providers. Bundling both on a single claim, or submitting the surgical code as the anesthesia code, creates a denial.
Reviewing IVF CPT codes as a parallel example shows how surgical and anesthesia billing responsibilities remain distinct across specialties. Similarly, ADHD screening CPT codes illustrate how documentation and code pairing standards apply consistently across the CPT framework.
Even experienced anesthesia billing teams encounter recurring errors with this code. Most fall into predictable categories.
Medicare and most commercial payers reject anesthesia claims submitted without a P1-P6 modifier. The physical status modifier is a required claim element, not an optional one. Build a claim scrubber rule that flags any 00126 line without a P-modifier before submission.
Submitting QZ (non-directed) when a physician was medically directing the case – or QX when no direction occurred – creates a compliance exposure. Each billing scenario has a specific modifier pair (QX/QK for directed cases, QZ for non-directed).
Confirm supervision documentation before selecting the modifier. Practices using anesthesia claims management software can build modifier validation rules directly into the claim submission workflow.
Time units are calculated from the anesthesia record. If the start and stop times are rounded to the nearest quarter-hour rather than recorded precisely, time units may be understated. For a short procedure like tympanotomy, even a 5-minute discrepancy can reduce reimbursement by one full time unit.
The 00120 error is one of the most common substitution mistakes in ENT anesthesia billing. Verify the surgical code before selecting the anesthesia code. If the surgical team bills 69436 or any tympanotomy-related code, CPT code 00126 is the correct anesthesia counterpart.
Similar NOS-versus-specific mismatches occur with other anesthesia codes, such as CPT code 00176 for intraoral procedures. Consulting the AAPC Codify CPT lookup can confirm the correct code family before submission.
Tympanotomy skews heavily pediatric. When the patient is under 1 year old, modifier 99100 must be appended and the additional qualifying circumstance unit must be billed. Failing to append 99100 for eligible patients leaves reimbursement on the table.
A pre-claim review step that checks patient age against the procedure date catches this error before submission. Structured pre-claim checklists that verify ICD-10 diagnosis code documentation alongside anesthesia records help prevent both modifier and diagnosis omissions.
Run a monthly audit of all CPT 00126 claims submitted in the prior 60 days. Filter for claims without a P-modifier, claims missing 99100 where the patient was under 1 year old, and claims where the anesthesia time is recorded as a round number. Round numbers often signal estimated rather than actual documentation, which creates audit risk.
Coverage policies for CPT code 00126 are consistent across major payers for tympanotomy, but several payer-specific rules affect reimbursement rates and submission requirements.
Medicare: Covers CPT code 00126 for medically necessary ear procedures. Reimbursement uses the Medicare anesthesia conversion factor published annually in the Physician Fee Schedule. Prior authorization is typically not required for tympanotomy under Medicare, but documentation of medical necessity (ICD-10 codes linking to otitis media diagnoses) must be present in the record.
Medicaid: Coverage and reimbursement rates vary by state. Some state Medicaid programs reimburse anesthesia for tympanotomy at a lower conversion factor than Medicare. Verify with your state’s provider manual before billing. New York Medicaid (eMedNY) explicitly lists CPT code 00126 as a covered tympanotomy anesthesia code in its April 2026 physician procedure code schedule.
Commercial payers: Most commercial carriers follow Medicare’s modifier and documentation requirements but negotiate their own conversion factors. Prior authorization requirements differ by plan. Check the payer’s provider portal or authorization system before scheduling anesthesia for elective tympanostomy tube placements.
Practices managing multi-payer anesthesia billing may benefit from prescription and medication tracking systems that integrate with their billing platform to keep anesthetic agent documentation aligned with claim submissions. For a broader comparison of billing platforms, see our review of the best medical billing software in the US.
CPT code 00126 claims fail for predictable reasons: missing P-modifiers, wrong CRNA billing modifiers, imprecise time documentation, and incorrect code substitution. These errors are systematic: they repeat across cases until the workflow is corrected.
Pabau’s claims management software helps anesthesia and ENT practices build modifier validation rules, attach correct ICD-10 diagnosis codes, and catch errors before submission. For teams ready to tighten their anesthesia billing workflow, book a demo to see how Pabau supports cleaner claims from documentation through submission.
Managing billing for multiple procedure types? Pabau claims management software helps practices reduce denials across CPT code families with built-in modifier validation.
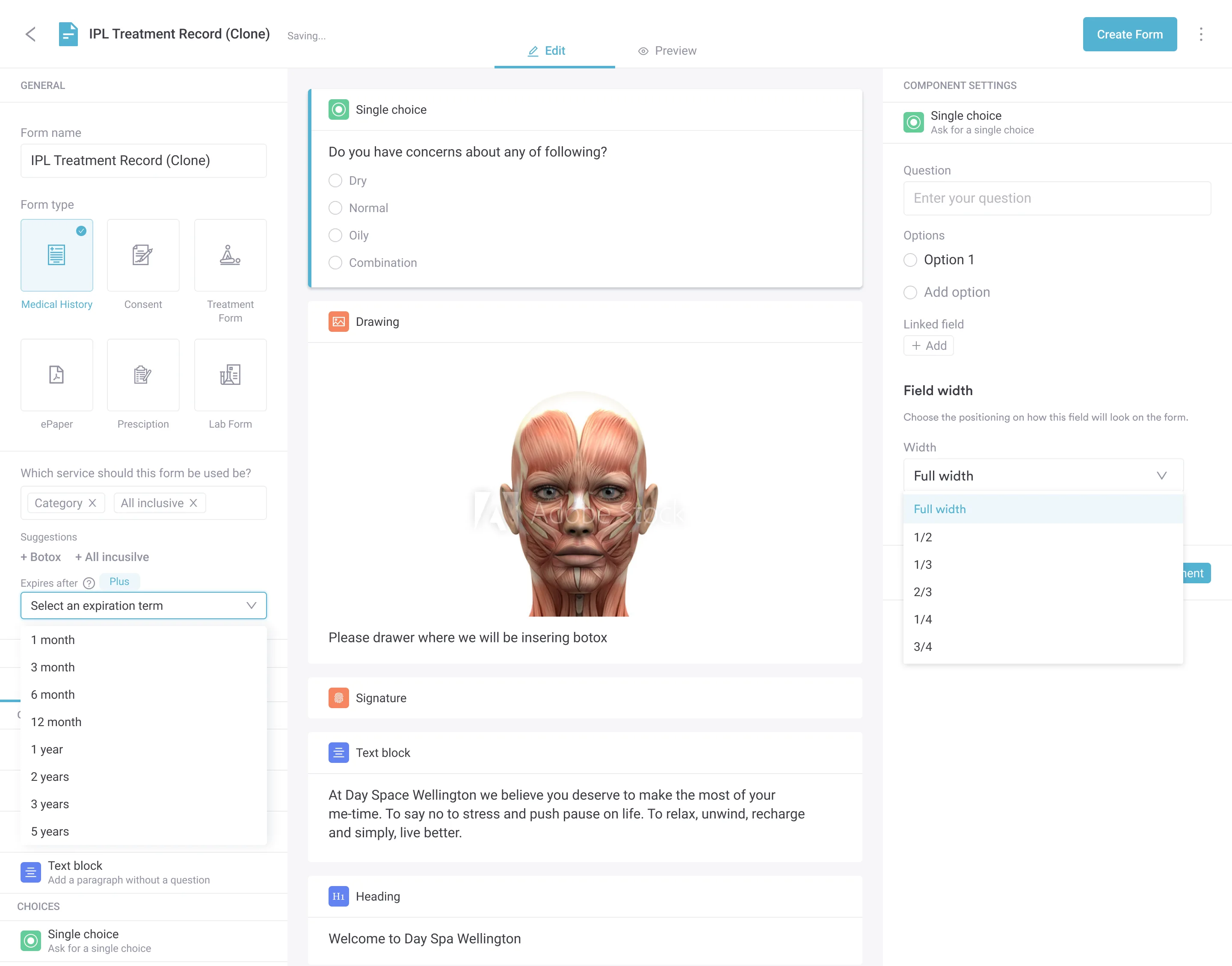
Need compliant anesthesia documentation templates? Pabau digital forms lets teams build structured anesthesia records that prompt for every required field, from ASA physical status to procedure stop time.
Looking for compatible EMR software for your surgical practice? Best EMR software for surgical practices reviews the features that matter most for anesthesia-compatible documentation and billing workflows.
CPT code 00126 describes anesthesia services for procedures on the external, middle, and inner ear, including biopsy and tympanotomy. It is maintained by the American Medical Association under the CPT category “Anesthesia for Procedures on the Head” and applies when a qualified anesthesia provider administers care during ear surgery.
CPT 00120 and CPT code 00126 cover the same anatomical scope – the external, middle, and inner ear, including biopsy – but 00120 is the not-otherwise-specified catch-all code, while 00126 is the specific code for tympanotomy. Tympanostomy tube placement requires 00126, not the generic 00120.
Modifier 99100 applies when the patient is under 1 year of age or over 70 years of age. It adds 1 qualifying circumstance unit to the claim. Because tympanotomy is common in young children, check patient age against the date of service on every 00126 claim before submission.
Reimbursement equals (base units + time units) multiplied by the anesthesia conversion factor. CPT code 00126 carries 4 base units. Time units accrue at 1 unit per 15 minutes of anesthesia time. The conversion factor is set by CMS annually for Medicare, and negotiated separately by commercial payers. Other anesthesia codes, such as CPT code 00700 and CPT code 00840, follow the same formula with different base unit values.
CPT code 00126 is the correct anesthesia code for tympanostomy tube replacement under general anesthesia. It pairs with the surgical code CPT 69436. The ASA physical status modifier (P1-P6) and, when applicable, modifier 99100 for pediatric patients must be appended to the anesthesia claim.
Common ICD-10 diagnosis codes supporting medical necessity for CPT code 00126 include H65.x (non-suppurative otitis media), H66.x (suppurative otitis media and related conditions), and H74.x (middle ear disorders). The diagnosis code must reflect the clinical indication documented in the patient’s medical record.
Yes. When bilateral myringotomy and tubes (BMT), the standard pediatric ear tube surgery, is done under general anesthesia, CPT code 00126 is the anesthesia claim that pairs with surgical code 69436. The surgeon bills the tube procedure and the anesthesia provider bills 00126 separately, each with its own modifiers.
Match the anesthesia code to what was actually done: 00124 covers diagnostic otoscopy under anesthesia, 00126 covers tympanotomy, and 00120 is the not-otherwise-specified option when neither fits. An ear exam under anesthesia does not default to one code, so bill from the documented procedure rather than the word exam alone.