ICD-10 code S53.442D: UCL sprain of left elbow, subsequent encounter
ICD-10 code S53.442D is a valid, billable ICD-10-CM diagnosis code effective Oct...
Last Updated: August 10, 2026
CPT code 00529 covers anesthesia for mediastinoscopy and diagnostic thoracoscopy utilizing one-lung ventilation, a closed chest procedure performed with a double-lumen endotracheal tube
The code carries 11 base units, the highest in the closed chest series; anesthesia payment is calculated as (base units + time units + modifying units) x conversion factor
Modifier selection depends on provider type: AA for a physician anesthesiologist working alone, QX or QY for a medically directed CRNA, QZ for an independent CRNA
Pabau’s claims management software helps practices submit, validate, and track claims, and reconcile payments against invoices from one platform
For an intrathoracic anesthesia case, one detail in the operative note decides which code you bill: whether the anesthesia team used one-lung ventilation. When a mediastinoscopy or diagnostic thoracoscopy is performed with one-lung ventilation, the case belongs to CPT code 00529.
That distinction is easy to miss. The neighboring code, 00528, describes the same two procedures performed without one-lung ventilation, and it carries fewer base units. Pick the wrong one, and the claim either loses base units or comes back denied for a code the documentation does not support.
Getting it right starts with what 00529 actually describes, then follows through to how its 11 base units, modifiers, and supporting diagnoses turn into a claim that gets paid.
CPT code 00529 is assigned to anesthesia services provided during a mediastinoscopy or diagnostic thoracoscopy that requires one-lung ventilation. The surgeon inserts a mediastinoscope through a small incision at the base of the neck to view and biopsy the mediastinum, or introduces a thoracoscope into the chest cavity, while the anesthesia team ventilates only one lung through a double-lumen endotracheal tube so the other lung can be deflated for surgical access.
The code sits within the anesthesia section maintained by the American Medical Association (AMA), specifically the intrathoracic procedure range spanning CPT codes 00500 through 00580. Coders reach for 00529 specifically when the operative report documents one-lung ventilation during a mediastinoscopy or diagnostic thoracoscopy; when the same procedures are performed without one-lung ventilation, 00528 is the correct code instead. Confirming whether one-lung ventilation was actually used, not just which scope was inserted, is what separates 00528 from 00529 on the claim.
This reference covers the code’s base units, the full anesthesia billing formula, applicable modifiers, CRNA versus physician billing rules, reimbursement context, ICD-10 crosswalk, and documentation requirements. For related CPT billing workflows in other specialties, Pabau maintains a growing library of procedure-code references.
CPT 00529 carries 11 base units, consistent with AMA CPT codebook values and confirmed across VA, state Medicaid, and commercial coding references (verify against the current edition for each billing year, as base units are subject to annual review). It is the highest base-unit value in the closed chest series, reflecting the added complexity of managing one-lung ventilation through a double-lumen endotracheal tube during the procedure.
The table below compares 00529 with the adjacent intrathoracic anesthesia codes in the 00500-00580 range. Understanding where 00529 sits in this sequence helps coders choose the most accurate code for the operative scenario.
The 11-unit assignment for 00529 is the highest in this group because one-lung ventilation adds real anesthetic complexity: the anesthesia team must place and confirm a double-lumen tube, manage oxygenation with one lung deflated, and be ready to re-inflate quickly if the patient desaturates. Anesthesia billing for other procedure-code families follows the same base-unit logic, though specific unit values differ by code section.
Anesthesia reimbursement does not work like a flat surgical fee. The Centers for Medicare and Medicaid Services (CMS) uses a formula that combines procedural complexity with actual anesthesia time and a regional conversion factor.
The standard formula, confirmed across CMS guidelines and billing references, is:
For a 3-hour mediastinoscopy or diagnostic thoracoscopy case billed under 00529 with no modifying units, the total anesthesia units equal 23. Multiply that by the applicable conversion factor to get the expected Medicare payment. Commercial payers set their own conversion factors, which may differ significantly from Medicare rates. Always verify the conversion factor with each payer before estimating reimbursement. For current Medicare conversion factor data, use the FastRVU 2026 RVU lookup tool.
Modifier selection for CPT 00529 directly affects reimbursement and compliance. The wrong modifier causes claim denial; omitting a required modifier triggers audit scrutiny. The applicable modifiers depend on who provides the anesthesia and what level of supervision is involved.
Commercial payers may apply their own modifier rules that differ from Medicare. Verify modifier requirements with each payer’s provider manual before submitting claims. For a broader look at claims management workflows built for specialty billing, Pabau’s platform keeps claim submission, validation, and status tracking in one system, from initial submission through payment reconciliation.
Audit your 00529 claims quarterly: filter by modifier and check that AA claims have no concurrent CRNA claims for the same time window, and that QX/QY pairs match on the same case. Mismatched modifier pairs are the most common reason anesthesia claims trigger payer audits.
Provider type changes both who submits the claim and which modifiers appear on it. Three distinct billing scenarios arise with CPT 00529.
Physician anesthesiologist (solo, modifier AA): The physician is personally present for the entire procedure. They submit the claim with modifier AA and receive 100% of the allowed anesthesia fee. This is the highest-reimbursement scenario under Medicare.
Medical direction (modifiers QK/QX or QY/QX): The physician medically directs one to four CRNAs performing concurrent cases. The physician submits with QK or QY (depending on the number of concurrent rooms); each CRNA submits a separate claim with QX. Under Medicare, the medically directed rate for both parties is 50% of the allowed fee, making the combined payment for physician plus CRNA equal to the solo physician rate.
Independent CRNA (modifier QZ): Where a state has exercised the CMS opt-out from physician supervision requirements, a CRNA may bill independently using modifier QZ and receive 100% of the anesthesia fee. CMS permits states to waive the supervision requirement, and more than two dozen states have done so as of mid-2026, though the list changes periodically. Always confirm current opt-out status with your state’s CMS regional office or the facility’s compliance team before billing QZ. Independent CRNA eligibility also depends on facility credentialing rules and state board of nursing scope-of-practice regulations.
Medicare does not publish a fixed dollar amount per anesthesia unit. Reimbursement for CPT 00529 depends on the total anesthesia units (base + time + modifying) multiplied by a locality-specific conversion factor that CMS updates annually through the Medicare Physician Fee Schedule (MPFS).
To look up the current conversion factor and any locality adjustments for your practice’s geographic area, use the CMS Physician Fee Schedule search tool. For a worked reimbursement estimate using current RVU data, the FastRVU lookup tool imports CMS data and applies geographic adjustments. Commercial payers, Medicaid, and VA programs each set their own conversion factors and may use different base-unit tables than Medicare.
The VA, for instance, publishes its own anesthesia base-unit table that lists CPT 00529 at 11 base units, consistent with the AMA CPT value. If your practice bills VA Community Care, verify base-unit values against the VA-specific table rather than assuming CMS values apply. For understanding how EHR integration for billing connects clinical documentation to claim submission, Pabau’s workflows keep the anesthesia record and the billing record in the same system, cutting out the manual re-entry step between the two.
Pabau's integrated billing workflows keep procedure documentation and claim submission in one place, so your team spends less time cross-checking reference tools and more time on clean claims.

Every anesthesia claim requires at least one supporting ICD-10-CM diagnosis code to establish medical necessity. For CPT 00529, the diagnosis codes reflect the condition that made mediastinoscopy or diagnostic thoracoscopy with one-lung ventilation necessary, most often lung cancer staging or an unexplained mediastinal finding. The table below lists ICD-10 codes frequently paired with 00529 on anesthesia claims.
This list is illustrative, not exhaustive. The correct ICD-10-CM code must reflect the actual diagnosis documented in the patient record. For a practical introduction to ICD-10 crosswalk principles, the Pabau resource on ICD-10 diagnosis coding walks through how crosswalks connect procedure codes to supporting diagnoses. The AAPC Codify CPT lookup also provides a CPT-to-ICD-10 crosswalk useful for validating code pairings before submission.
An underdocumented anesthesia record is the fastest path to a denied claim or failed audit. For CPT 00529, the anesthesia record must capture every element CMS and payers use to calculate and validate the claim.
Maintaining HIPAA-compliant billing records is a baseline requirement for every anesthesia claim. Pabau’s digital documentation tools capture procedure notes with timestamped entries, supporting a complete anesthesia record and audit readiness. Practices using structured medical forms at the point of care reduce the risk of missing documentation elements that trigger post-payment reviews. For a comprehensive approach to billing efficiency in private practices, integrated documentation and billing tools remove the manual transfer step between the anesthesia record and the claim.
Most anesthesia billing errors originate at the handoff between clinical documentation and claim submission. When time units come from a paper record and get manually entered into a separate billing system, discrepancies are easy to introduce and hard to catch before submission.
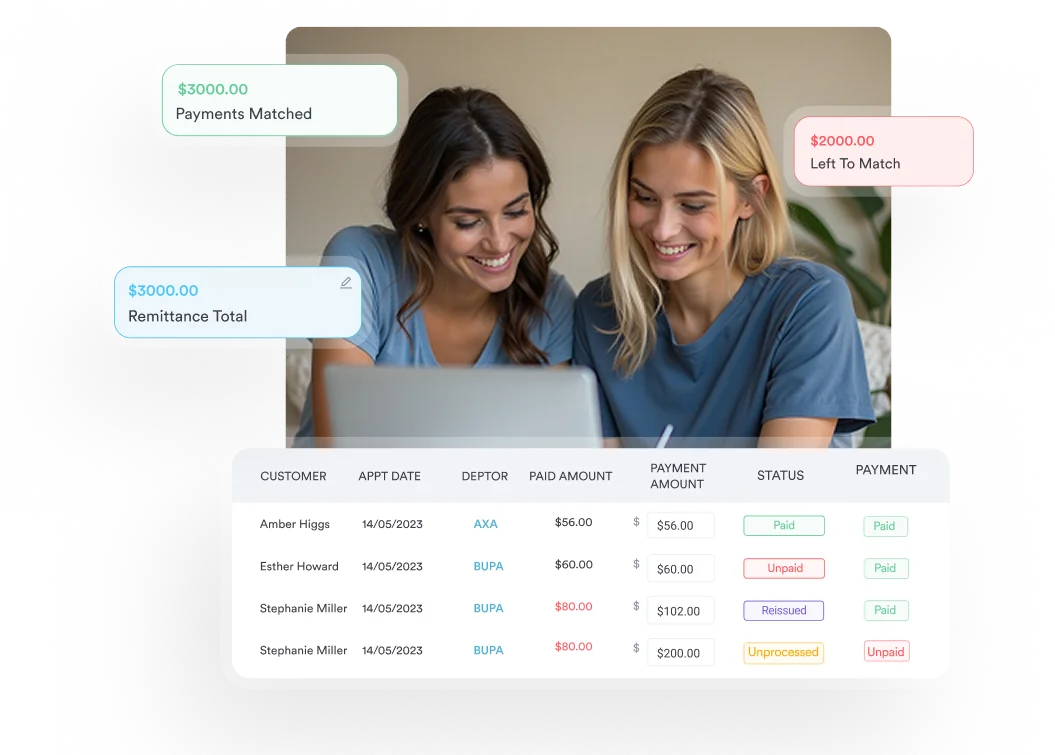
Pabau’s claims management software connects procedure documentation directly to the billing workflow, so the anesthesia record and the claim live in the same system rather than two separate ones. Built-in field validation checks a claim before it goes out, and a live claim-status dashboard lets administrators follow up on outstanding claims and reconcile payments against invoices, supporting the kind of quarterly audit the pro tip above recommends. For practices looking to understand how practice management software integrates billing and documentation, Pabau’s platform is built around that workflow connection.
Getting CPT 00529 right comes down to three decisions made before the claim is submitted: correct code selection (confirming the operative report documents one-lung ventilation rather than billing 00528 or a different adjacent code), accurate modifier selection based on provider type and supervision arrangement, and complete time documentation that supports the unit count. Errors in any one of these areas lead to denial, audit risk, or underpayment.
Pabau’s integrated approach connects the anesthesia record to the claim in a single workflow, reducing the manual-transfer errors that cause most anesthesia billing rejections. To see how Pabau handles claim submission, validation, and tracking for anesthesia and other specialty practices, explore Pabau’s claims management features.
Need a reference for other anesthesia-adjacent CPT codes? CPT billing workflows for specialty codes covers how to apply the same base-unit and modifier logic across different procedure-code families.
Looking to strengthen HIPAA compliance in your billing process? HIPAA compliance for medical offices outlines the documentation and data-handling requirements that apply to every anesthesia claim record.
Want to see how digital documentation reduces billing errors? Pabau’s digital forms capture structured clinical data at the point of care, supporting clean-claim submission without manual transcription.
CPT code 00529 is used to report anesthesia services for a mediastinoscopy or diagnostic thoracoscopy that requires one-lung ventilation. The surgeon views or biopsies the mediastinum through a small incision at the base of the neck, or explores the chest cavity with a thoracoscope, while the anesthesia team ventilates one lung through a double-lumen endotracheal tube so the other lung can be deflated for surgical access. When the same procedures are performed without one-lung ventilation, 00528 is the correct code instead.
CPT 00529 carries 11 base units, the highest value in the closed chest anesthesia series, reflecting the added complexity of managing one-lung ventilation during the procedure. Base unit values are assigned by the AMA and are subject to annual review; always verify against the current CPT codebook edition before billing.
The applicable modifiers are AA (physician personally performing), QK (physician directing two to four CRNAs), QX (CRNA under medical direction), QY (physician directing one CRNA), QZ (independent CRNA), AD (physician supervising five or more cases), and GC (teaching physician with resident). Modifier choice depends on who provides the anesthesia and the supervision arrangement in place for the case.
Anesthesia payment equals (base units + time units + modifying units) multiplied by the applicable conversion factor. For CPT 00529 with 11 base units, a 3-hour case produces 12 time units (1 unit per 15 minutes), giving 23 total units before modifying units. Multiply by the payer’s current conversion factor to estimate payment. Medicare conversion factors vary by locality and are updated annually.
Yes, a CRNA can bill CPT 00529 independently using modifier QZ, but only in states that have exercised the CMS opt-out from physician supervision requirements and where the facility’s credentialing rules permit independent CRNA practice. CRNA independent billing eligibility depends on both state law and facility policy; verify current opt-out status with your state’s CMS regional office before billing QZ.
CPT 00529 covers mediastinoscopy and diagnostic thoracoscopy performed with one-lung ventilation and carries 11 base units, the highest in the closed chest series. Adjacent codes describe related but distinct scenarios: 00520 is the general not-otherwise-specified code, including bronchoscopy, at 6 base units; 00522 covers needle biopsy of pleura at 4 base units; 00524 covers pneumocentesis at 4 base units; and 00528 covers the same mediastinoscopy or diagnostic thoracoscopy procedures as 00529 but without one-lung ventilation, at 8 base units. Confirm from the operative report whether one-lung ventilation was actually used before choosing between 00528 and 00529.