HIPAA medical release form
Nine elements make a HIPAA authorization valid, not eight. Read more on what eac...
Last Updated: July 31, 2026
An authorization for release of confidential information is a legally required form that allows patients to permit healthcare providers to share protected health information (PHI) with named recipients.
HIPAA regulations require authorizations to include: description of information, recipient name, purpose, expiration date/event, patient signature and date, and the right to revoke without penalty (45 CFR § 164.508).
Substance use disorder (SUD) records fall under stricter 42 CFR Part 2 confidentiality rules and require a separate, specific authorization with enhanced language and protections.
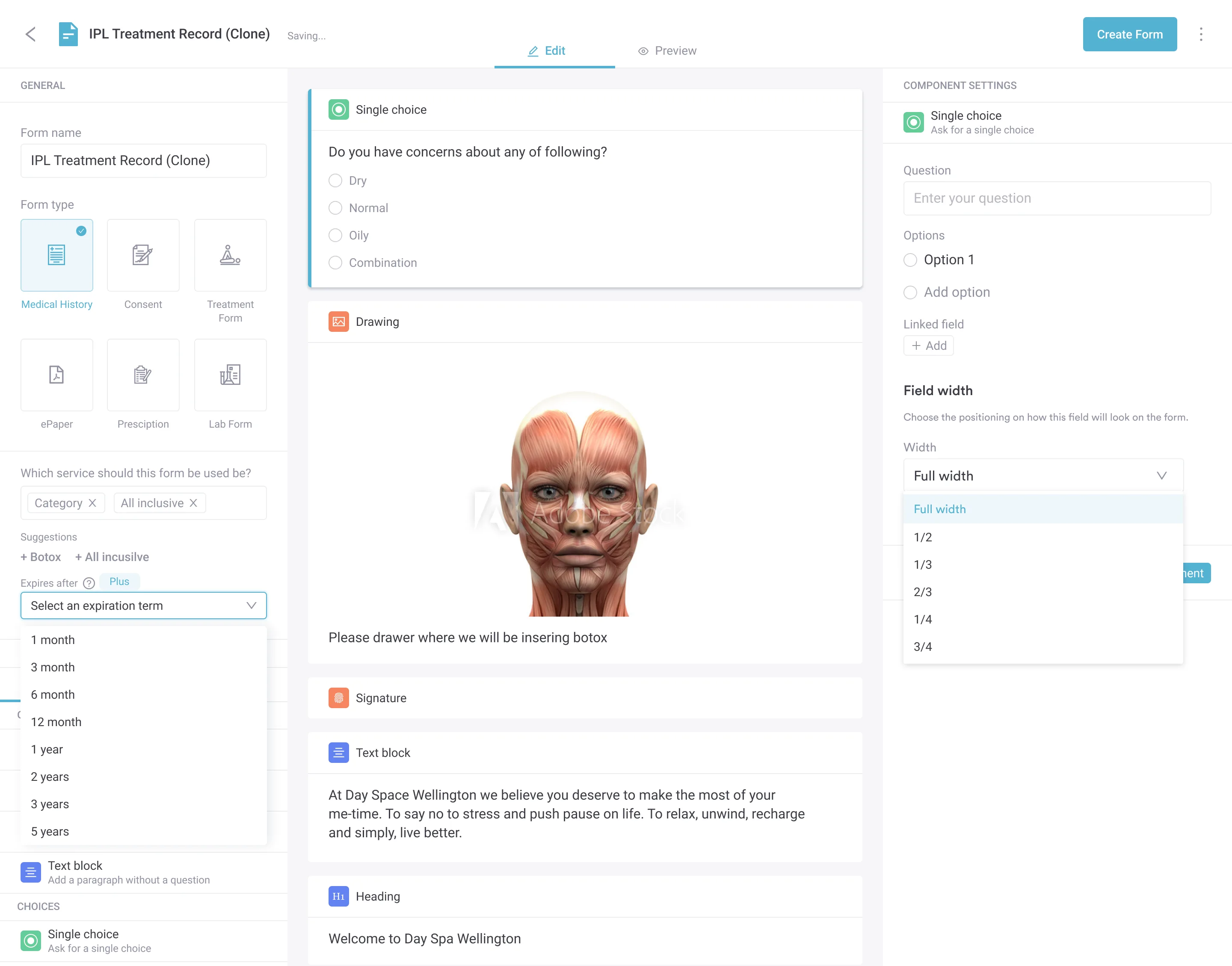
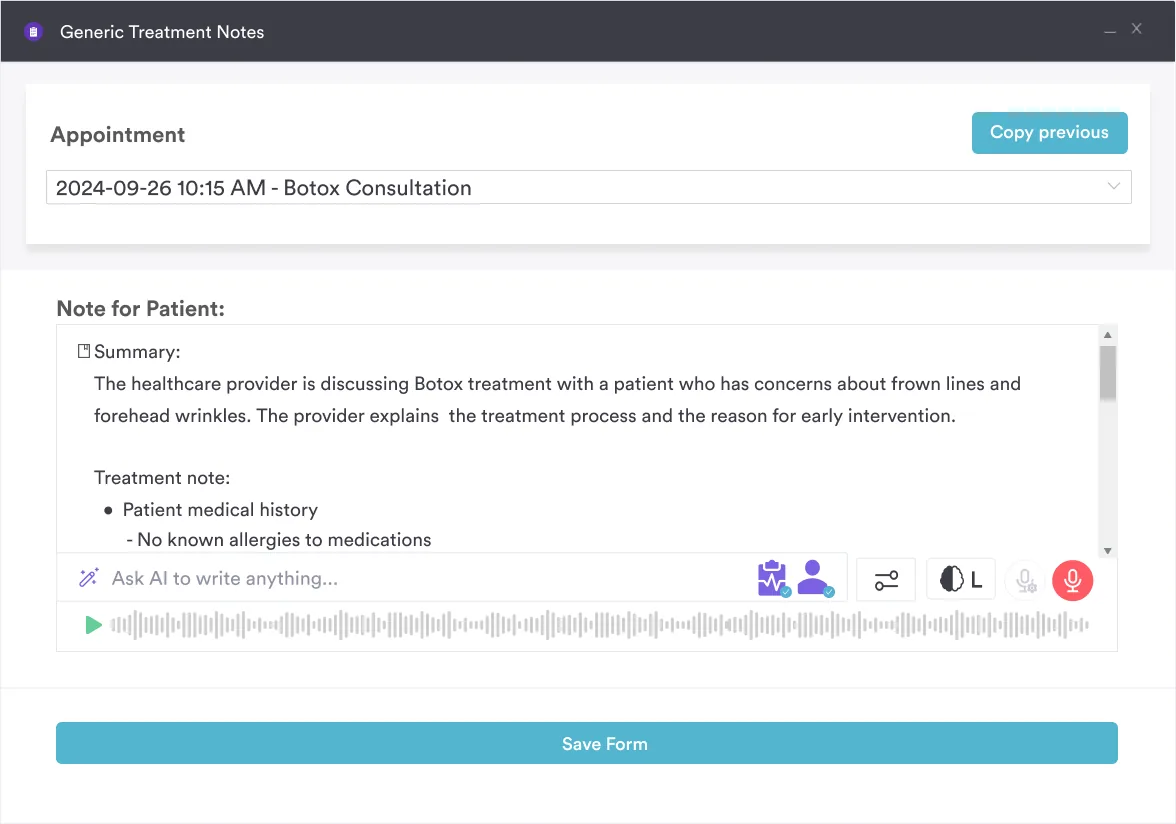
Practice management software like Pabau automates authorization collection through digital forms and stores signed documents securely, cutting out manual paper workflows.
A HIPAA-compliant consent form covering patient details, information to be released, purpose of disclosure, recipient information, expiration date, patient rights, signature, and regulatory compliance language for mental health, therapy, and general healthcare practice workflows.
Download templateSharing a patient’s records with anyone outside treatment, payment, or healthcare operations requires their written permission first. Whether you’re a therapist releasing mental health records, a primary care physician sending files to a specialist, or an addiction treatment provider handling substance use disorder confidentiality, the authorization for release of confidential information form is what makes that disclosure legal.
HIPAA civil penalties range from roughly $145 to $73,011 per violation. The annual cap reaches $2,190,294 per violation category, and HHS adjusts these figures periodically for inflation. On top of that, state-level privacy laws add even stricter penalties.
This guide explains what an authorization for release of confidential information is, when it’s legally required, and how to complete it correctly. It also shows how practice management software like Pabau collects, signs, and stores these forms with a complete audit trail, so you can keep every disclosure defensible without the paper.
An authorization for release of confidential information is a signed legal document that lets a healthcare provider disclose a patient’s protected health information (PHI) to a named third party. It records the patient’s explicit consent, which HIPAA requires for most disclosures outside treatment, payment, and healthcare operations.
A Notice of Privacy Practices only informs patients of their rights, and a general consent-to-treatment form does the same. An authorization is more specific. It names exactly what information you can share, with whom, for what purpose, and for how long. Without it, sharing patient records, even with another healthcare provider, counts as a breach.
Completing and collecting these forms correctly is the difference between a compliant practice and a HIPAA liability. Follow these five operational steps to keep every authorization legally defensible and clinically appropriate.
Any practice that holds patient information and receives requests to share it needs a compliant authorization process. For example, common users include:
Legal protection: A signed, properly completed authorization shields your practice from HIPAA violations and state privacy law breaches. It documents informed patient consent and creates an audit trail. Regulators, including HHS Office for Civil Rights, CMS, and state health departments, expect to see this trail during compliance reviews and breach investigations.
In addition, some practices pair this with a broader HIPAA authorization form template for general-purpose disclosures.
Workflow efficiency: Because standardized authorization forms reduce administrative burden, staff save time on every disclosure. Staff don’t have to custom-write disclosure letters or negotiate scope with patients. Instead, the form clarifies exactly what the practice is sharing, with whom, and why.
Digital patient intake forms also eliminate manual printing, scanning, and filing, so staff reclaim hours they would otherwise spend chasing paperwork.
Patient transparency: An authorization ensures patients understand what records the practice is releasing and to whom. This builds trust and reduces disputes over “I didn’t know you were sharing my information with my employer.” Clear, HIPAA-aligned language, stored in a secure EHR, helps patients feel in control of their own data.
Regulatory readiness: Regulators frequently cite missing or incomplete authorizations during inspections. Practices that keep a signed, complete authorization for every disclosure clear HHS OCR audits and state health department reviews faster and with fewer findings. Many track this with dedicated HIPAA compliance software that flags a missing authorization before an audit does.
Audit your current authorization process: pull 10 random patient records from the last 3 months, and verify that every disclosure has a signed authorization on file (records sent to specialists, insurance companies, family members, or other practices). If any disclosures lack signed authorizations, document the finding and put a corrective action plan in place. This self-audit is your best defense against future compliance findings.
While HIPAA sets the federal floor, individual states additionally impose stricter requirements for release of confidential information. A form that meets federal HIPAA standards may not comply with your state’s privacy laws.
Best practice: obtain your state’s model authorization (if available) and cross-reference it with your HIPAA form. If your state has stricter language requirements, integrate them into your standard template. When in doubt, consult your state’s health department or a healthcare attorney.
The U.S. Federal ESIGN Act (15 U.S.C. § 7001) permits electronic signatures on healthcare documents, so an electronically signed authorization is legally equivalent to a wet signature and binding under federal law.
Electronic collection is faster, reduces manual filing errors, and creates an automatically timestamped audit trail. Read more about running a paperless, HIPAA-compliant practice if you’re still relying on printed forms.
To streamline authorization collection, book a demo and see how Pabau’s digital forms handle the full workflow: electronic signature capture, automatic document storage, and compliance audit trails in one place.
Substance use disorder (SUD) treatment records are among the most heavily protected health information in the US healthcare system. They fall under 42 CFR Part 2 (federal substance use confidentiality regulations), which imposes stricter rules than standard HIPAA.
SUD practices and addiction treatment programs must use a separate authorization form built for substance use disorder records. The Pabau template above includes standard HIPAA language, so SUD practices should customize it to add the 42 CFR Part 2 disclosures and prohibitions.
Consult the full text of 42 CFR Part 2 for the exact required consent language for your program type.
An authorization for release of confidential information is the legal cornerstone of patient privacy in healthcare. Whether you’re releasing mental health records, SUD treatment information, or general medical records, a signed, complete form protects your practice. It also respects patient autonomy and ensures compliance with HIPAA, state privacy laws, and regulations like 42 CFR Part 2.
Download the free template above, customize it for your state and specialty, and integrate it into your patient intake workflow. For streamlined digital collection, schedule a demo with Pabau. You’ll see how practice management software automates authorization workflows and keeps your practice audit-ready.
Need guidance on HIPAA compliance beyond authorizations? Compliance management features help practices audit documentation, audit trails, and regulatory readiness across all patient touchpoints.
Looking for a template for a specific treatment type? Group therapy informed consent and psychiatric evaluation templates are available alongside authorization forms.
Documenting mental health assessments? Our newly published anxiety nursing diagnosis template gives you a structured starting point.
Managing broader patient documentation? Our diabetes medication list and EMT patient assessment templates are also available for practices handling chronic care and emergency intake.
An authorization for release of confidential information is a signed, written legal document that permits a healthcare provider to disclose a patient’s protected health information (PHI) to a named third party. It is required by HIPAA (45 CFR § 164.508) for most non-treatment, non-payment, and non-operations disclosures.
An authorization is required whenever you disclose PHI for purposes other than treatment, payment, or healthcare operations. Common triggers include requests from family members, employers, insurance companies, attorneys, educational institutions, or researchers. Disclosures for treatment coordination with another provider, billing inquiries, or credentialing do not require a separate authorization.
Yes. Patients have the right to revoke an authorization in writing at any time, except where action has already been taken in reliance on the authorization (45 CFR § 164.508(b)(5)). Keep a dated record of revocations and immediately halt further disclosures under that authorization.
Yes. Electronic signatures are legally binding under the U.S. Federal ESIGN Act (15 U.S.C. § 7001) and are HIPAA-compliant. Esignature platforms like Docusign and patient portal signing systems create timestamped audit logs and are admissible as evidence in regulatory reviews.
42 CFR Part 2 is a federal regulation that governs substance use disorder (SUD) treatment records. It imposes stricter confidentiality rules than HIPAA and requires a separate, specific authorization with mandated language. SUD practices must use a dedicated form that includes SAMHSA-required disclosures and prohibitions on re-disclosure.
HIPAA civil penalties range from roughly $145 to $73,011 per violation, with an annual cap of up to $2,190,294 per violation category (figures adjusted periodically by HHS), plus potential civil lawsuits from the patient. State privacy laws (California CMIA, Texas Occupations Code, etc.) impose additional penalties. A single unauthorized disclosure can trigger regulatory investigations and reputational damage.
The patient signs their own authorization. For a minor, a patient who lacks capacity, or a deceased patient, a parent, legal guardian, or personal representative signs on their behalf and must show documentation of that authority. Record the signer’s name, relationship, and authority on the form.