ICD-10 code M17.2: Bilateral post-traumatic osteoarthritis of knee
ICD-10 Code M17.2 is a billable diagnosis code for bilateral post-traumatic oste...
Last Updated: July 29, 2026
ICD-10 Code H52.6 is a billable diagnosis code for other disorders of refraction. It’s valid for reimbursement claims with a date of service on or after October 1, 2015.
H52.6 covers five synonymous conditions: accommodative excess, accommodative fatigue, anisophoria, drug-induced refractive change, and transient refractive change.
Documentation must specify the type of refractive disorder and its clinical cause. Vague notes are a common cause of claim denials.
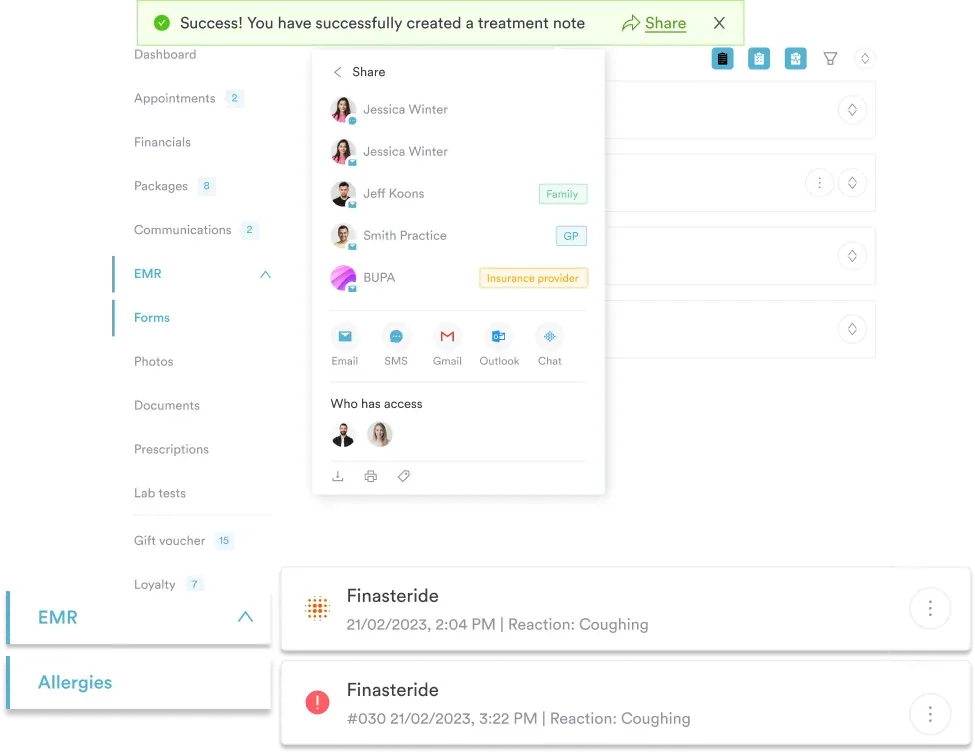
Pabau’s claims management software and digital forms help optometry and ophthalmology practices code H52.6 accurately and reduce billing errors.
ICD-10 code H52.6, “Other disorders of refraction,” covers refractive conditions that don’t fit the more specific entries in the H52 category. Optometrists and ophthalmologists use this code when a patient’s refractive disorder isn’t a straightforward case of myopia, hypermetropia, astigmatism, presbyopia, or another named condition in the block. The disorder still needs accurate documentation and coding.
According to CMS ICD-10-CM coding guidelines, ICD-10 Code H52.6 sits in Chapter 7 (H00-H59), Diseases of the Eye and Adnexa. It falls under the H52 subcategory for disorders of refraction and accommodation. The WHO International Classification of Diseases classifies it under the range covering disorders of ocular muscles, binocular movement, accommodation, and refraction.
ICD-10 Code H52.6 is a billable, specific ICD-10-CM code. Practices can use it on reimbursement claims with a date of service on or after October 1, 2015. That’s when the Centers for Medicare and Medicaid Services (CMS) required ICD-10-CM for all HIPAA-covered transactions.
The code is valid for the 2026 fiscal year. It doesn’t need a more specific fourth or fifth character to be billable, which sets it apart from several neighboring codes in the H52 category.
H52.5 (Disorders of accommodation), for example, is a non-billable header that needs a more specific child code. H52.6, by contrast, stands alone as the final, billable level of classification.
| Field | Value |
|---|---|
| Code | H52.6 |
| Description | Other disorders of refraction |
| Chapter | Chapter 7: Diseases of the eye and adnexa (H00-H59) |
| Category | H52: Disorders of refraction and accommodation |
| Billable | Yes (specific, valid for reimbursement) |
| Valid from | October 1, 2015 |
| Valid for FY | 2026 |
| MS-DRG grouping | MS-DRG v43.0: 124 (Other disorders of the eye with MCC or thrombolytic agent) |
Five conditions fall under ICD-10 Code H52.6. Each is a distinct clinical presentation, but none meets the criteria for the more specific codes in the H52 range.
This is a temporary shift in the eye’s refractive status. Blood sugar swings (common in patients with diabetes), medication effects, or post-surgical changes often trigger it. The documentation should note the transient nature and the suspected cause. A diabetes eye exam template can help standardize how that history gets captured at the point of care.
Practices using clinical records management software can attach relevant systemic history directly to the encounter note. That extra context strengthens the clinical rationale for this code.
Certain medications can produce rapid refractive shifts. These include sulfonamides, topiramate, and some antidepressants, which can swell the ciliary body or push the lens forward. When coding drug-induced refractive change under ICD-10 Code H52.6, name the causative drug in the clinical note. Where relevant, add a secondary adverse-effect code from the T36-T50 range to support medical necessity.
Accommodative excess occurs when the ciliary muscle over-converges, producing a pseudomyopic presentation. It shows up most often in children and young adults who do a lot of near-work, like reading or screen time. Clinicians should document the binocular vision findings, cycloplegic refraction results, and any related asthenopia symptoms.
Accommodative fatigue is a drop in sustained focusing ability that typically worsens through the day. It overlaps with convergence insufficiency in symptoms, but amplitude-of-accommodation testing tells the two apart. The clinical note should record the accommodative amplitude, the conditions under which symptoms occur, and any related vergence findings.
Anisophoria is a condition where the phoria (the eyes’ tendency to deviate) differs depending on the direction of gaze or the distance being tested. It’s distinct from anisometropia (coded as H52.3). Documentation should include the phoria measurement at different fixation distances, to justify this diagnosis over H52.7 (Unspecified disorder of refraction).
Understanding where ICD-10 Code H52.6 sits within the H52 category helps coders pick the most specific code available. The H52 block covers disorders of both refraction and accommodation. Several codes in the range are non-billable headers that need a more specific child code.
Coders across specialties will recognize this pattern: always use the most specific billable code the clinical record supports. For eye care, that means preferring H52.6 over H52.7 whenever the documentation identifies one of the five included conditions. The CDC/NCHS ICD-10-CM web tool provides the official tabular list for checking code hierarchy and inclusion notes.
The Chapter 7 eye block includes other billable codes worth recognizing alongside H52.6, such as H53.8 (Other visual disturbances), H32 (Chorioretinal disorders in diseases classified elsewhere), and H51.0 (Palsy of conjugate gaze). Keeping these neighboring codes in mind helps coders route each encounter to the right entry in the eye chapter.
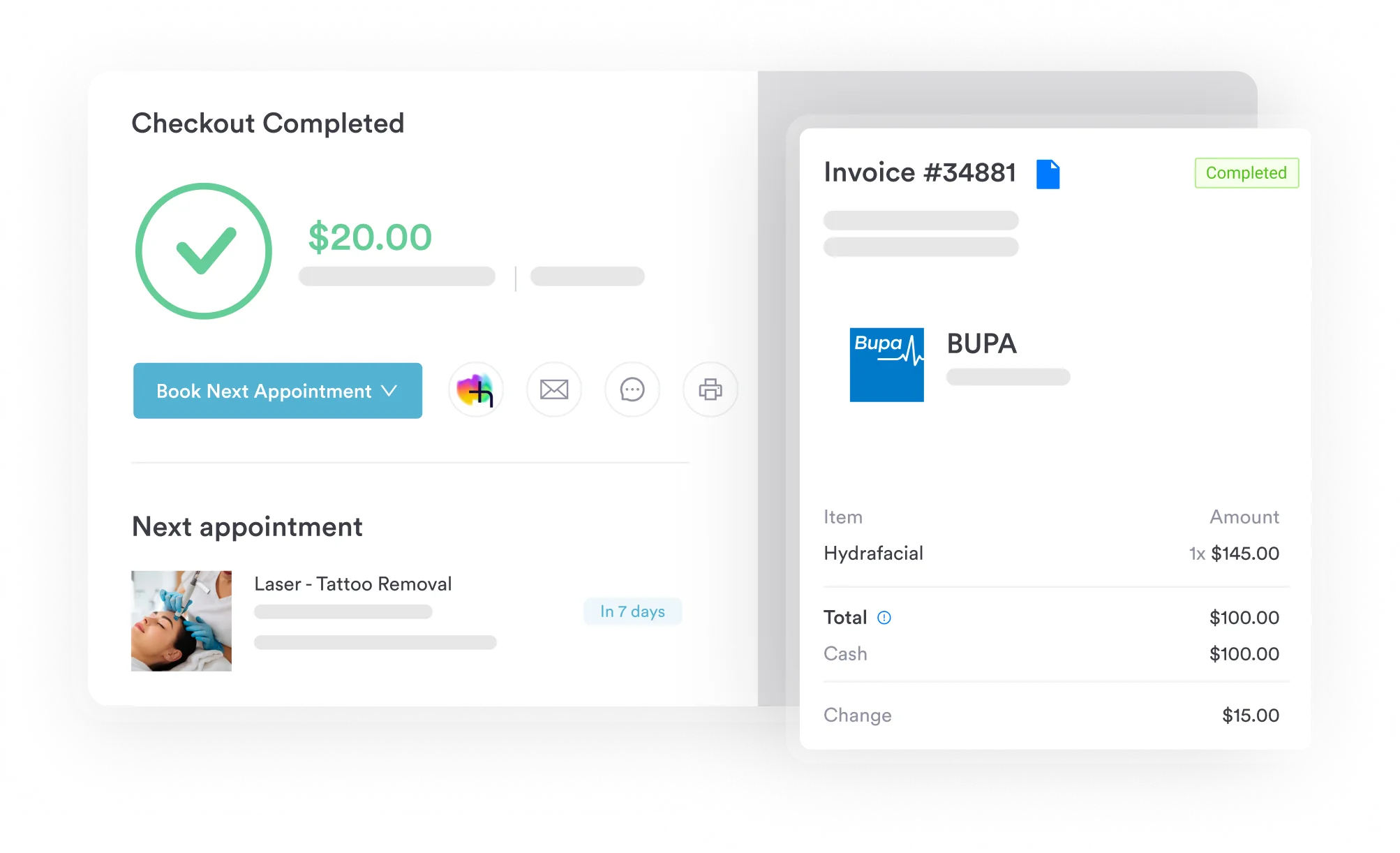
ICD-10 Code H52.6 falls within MS-DRG v43.0: DRG 124, Other disorders of the eye with MCC or thrombolytic agent. MS-DRG groupings matter mainly for inpatient hospital billing. Most H52.6 encounters happen in outpatient optometry or ophthalmology settings. There, the code supports the medical necessity of specific CPT procedures rather than a DRG assignment.
Two CPT codes commonly pair with ICD-10 Code H52.6 in outpatient eye care billing. CPT 92015 (Determination of refractive state) is the standard refraction procedure code. Medicare doesn’t cover it as a medical benefit, but vision plans often do.
CPT 92014 (Ophthalmological services: medical examination and evaluation, established patient, comprehensive) supports the evaluation component. It applies when the refractive disorder is part of a broader eye exam.
Payers cover these two codes differently, so practices should check plan-level benefits before submitting combined claims. Other commonly billed optometry procedures, like CPT 92310 (Contact lens fitting), follow similarly payer-specific coverage rules.
Flag H52.6 claims that pair CPT 92015 with Medicare as primary payer: Medicare does not cover routine refractive services. Bill the examination component (CPT 92014) separately and collect CPT 92015 directly from the patient or their vision plan. Document the medical necessity of the exam independently of the refraction to protect the 92014 claim.
Payers audit H52.6 claims more often than straightforward refractive codes, because the “other” designation invites scrutiny. If a claim lacks documentation for one of the five included conditions, reviewers will likely reclassify it as H52.7. That reclassification can delay reimbursement, even when payers accept the code itself.
Strong documentation for ICD-10 Code H52.6 should include all of the following elements:
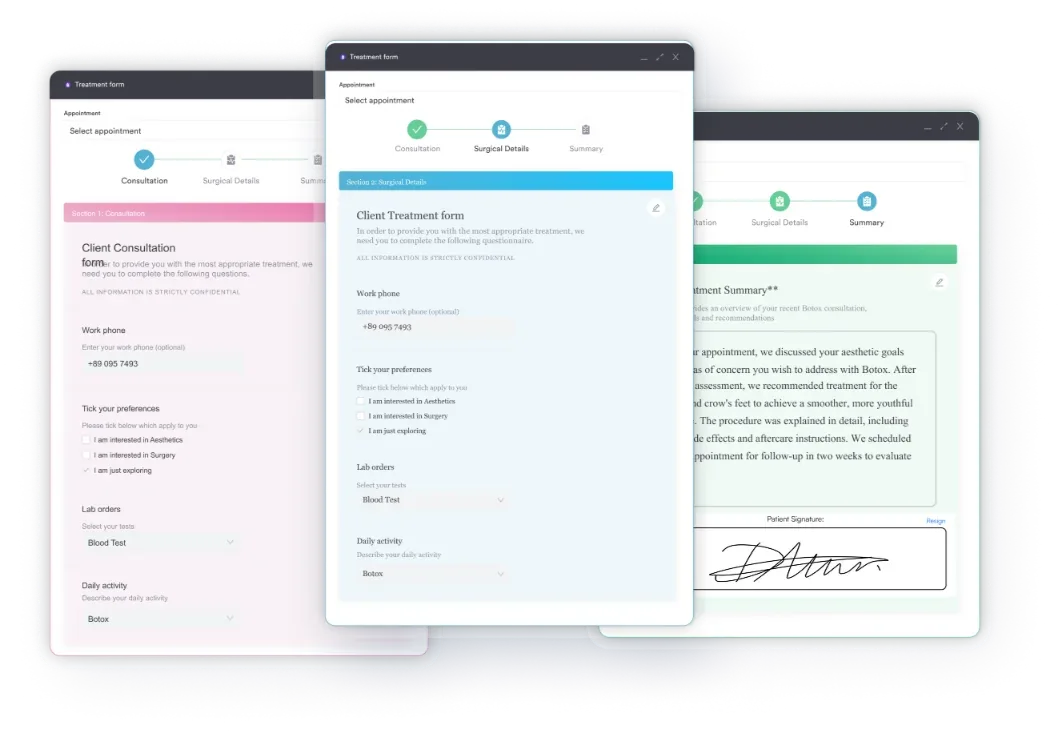
Practices that use digital forms to capture structured intake data can pre-fill relevant fields (current medications, visual symptoms, prior refractive history) before the clinician opens the encounter note. This reduces the missing documentation that leads to denials.
The same principle applies to standardized clinical intake forms for medical practices: build the right data fields into the point of capture, instead of relying on notes added after the fact. A PERRLA-based eye exam form is a practical example for eye care, since it standardizes the objective findings coders need to see.
H52.7 (Unspecified disorder of refraction) should be a last resort. AAPC coding guidelines, available through the AAPC Codify ICD-10-CM lookup, say unspecified codes are acceptable only when the clinical documentation truly doesn’t support a more specific diagnosis. For many encounters currently coded H52.7, a closer read of the clinical note would reveal one of the H52.6 synonyms.
Here is the practical decision rule:
Practices managing HIPAA-compliant documentation workflows benefit from structured templates that prompt clinicians to specify the type of refractive disorder before finalizing the encounter note. This single step greatly reduces unspecified H52.7 assignments and supports more defensible coding decisions.
The same approach applies to other ICD-10 reference areas. ICD-10 diagnostic code references in mental health settings, for example, follow the same rule: specific documentation determines reimbursement outcomes.
Pabau, an all-in-one practice management system, helps optometry and ophthalmology practices capture the documentation needed to support ICD-10 Code H52.6 claims. It offers structured digital intake forms and automated billing workflows that flag incomplete encounter notes before submission.

Claim denials for H52.6 rarely reflect a coding error at the code-selection stage. Instead, they reflect documentation written before the coder saw the chart, with no structured prompt to identify the type of refractive disorder. Workflow integration closes that shortfall.
A practical approach has three stages. First, intake forms capture the patient’s medication list, relevant systemic diagnoses (diabetes, autoimmune conditions), and visual symptom history. Second, the clinical encounter template includes pre-mapped diagnostic options for each H52.6 synonym.
This way, the clinician records the specific condition instead of writing free text like “refractive disorder.” Third, the billing team reviews the encounter note against the submitted code before the claim leaves the practice.
Pabau’s claims management software supports this workflow by linking encounter documentation to claim submission. It surfaces coding discrepancies before submission, rather than after a denial.
The AI-assisted clinical documentation feature further reduces missing documentation. It generates structured clinical notes from dictated or typed encounter summaries, capturing the clinical detail that supports specific ICD-10 code selection. For a closer look at how structured notes cut coding errors across specialties, see our guide to clinical documentation software.
For eye care practices managing multiple patients per session, this kind of automation matters. It’s often the difference between an H52.6 claim that pays on first submission and one that needs a rework cycle.
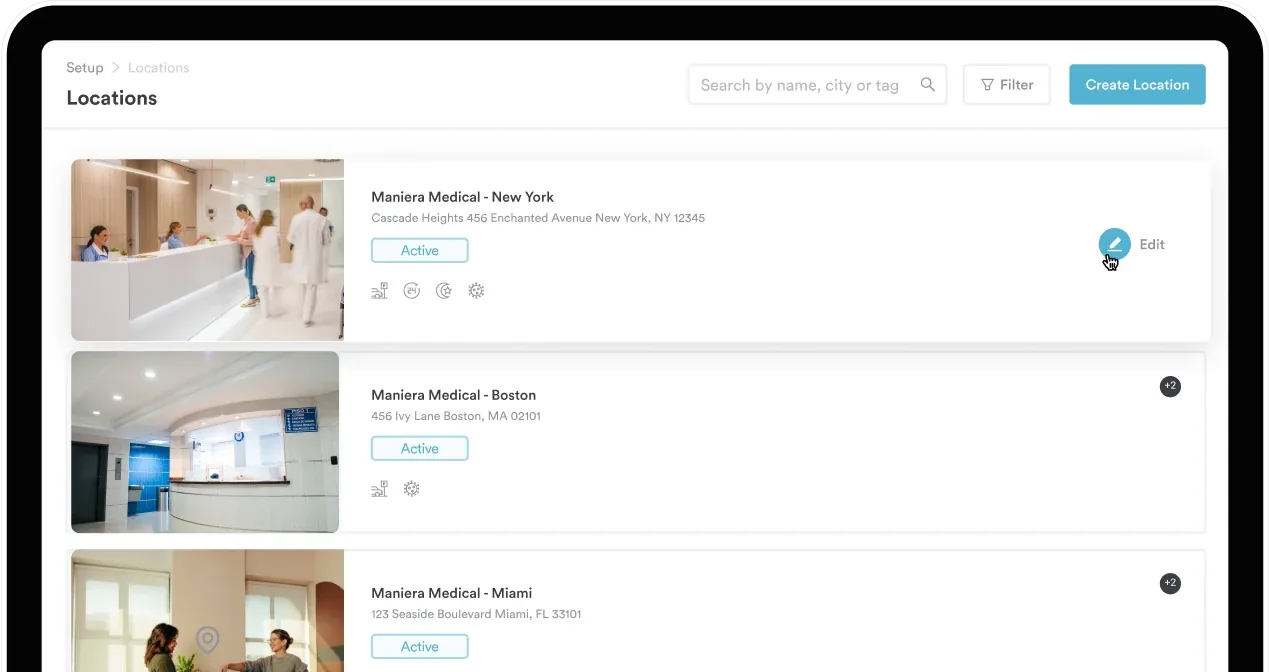
Practices that operate across multiple practice locations face extra consistency challenges. Coding standards need to apply the same way across every site, not vary by individual clinician habit. Centralizing ICD-10 code templates and documentation prompts in a single practice management system solves this directly.
Build a quick-reference card for your front-desk and billing team. List the five H52.6 synonyms alongside the documentation element each requires. Transient refractive change needs a named trigger. Drug-induced change needs the causative agent. Accommodative excess and fatigue need amplitude data. Anisophoria needs phoria measurements at distance and near. Post this beside the coding workstation to reduce H52.7 defaults.
Claim denials tied to ICD-10 Code H52.6 are almost always a documentation problem, not a coding problem. The code is billable, specific, and valid for 2026.
Its five included conditions — transient refractive change, drug-induced refractive change, accommodative excess, accommodative fatigue, and anisophoria — are distinct clinical entities, each with its own documentation needs. When the encounter note captures the right clinical detail, H52.6 supports a defensible, payable claim.
Pabau’s practice management workflows for eye care and specialist practices embed coding support directly into the clinical encounter. This narrows the difference between what clinicians document and what coders need. To see how Pabau handles ICD-10 documentation and claim submission for optometry and ophthalmology practices, book a demo.
Handling HIPAA-covered transactions for your practice? HIPAA compliance for medical offices explains the documentation and data security requirements that govern ICD-10 claim submissions.
Need the neighboring code for optic chiasm disorders? ICD-10 Code H47.49 covers disorders of the optic chiasm in other conditions classified elsewhere.
Seeing a nerve palsy case instead? ICD-10 Code H49.12 covers fourth trochlear nerve palsy of the left eye.
Not sure the disorder fits any named category? ICD-10 Code H44.9 is the unspecified code for disorders of the globe.
Billing an established-patient office visit alongside an eye exam? CPT Code 99214 covers documentation requirements for that visit level.
ICD-10 Code H52.6 is a billable ICD-10-CM diagnosis code for other disorders of refraction. It covers five specific conditions: transient refractive change, drug-induced refractive change, accommodative excess, accommodative fatigue, and anisophoria. It’s valid for dates of service on or after October 1, 2015, and remains current for fiscal year 2026.
Yes. H52.6 is a specific, billable ICD-10-CM code that doesn’t need an extra character to support reimbursement claims. It contrasts with H52.5 (Disorders of accommodation), a non-billable header that needs a fully specified child code for billing.
H52.6 applies when clinical documentation identifies one of five included conditions: transient refractive change, drug-induced refractive change, accommodative excess, accommodative fatigue, or anisophoria. H52.7 (Unspecified disorder of refraction) applies only when the documentation describes a refractive disorder without enough detail for a more specific H52 code. Use H52.7 as a last resort, not a default.
CPT 92015 (Determination of refractive state) and CPT 92014 (Comprehensive ophthalmological examination, established patient) are the most common pairings. Medicare doesn’t cover CPT 92015 as a medical benefit. For most Medicare encounters, vision plan coverage and direct patient billing apply to the refraction instead.
Under MS-DRG v43.0, ICD-10 Code H52.6 falls within DRG 124 (Other disorders of the eye with MCC or thrombolytic agent). MS-DRG assignment matters mainly for inpatient facility billing. Most H52.6 encounters happen in outpatient optometry or ophthalmology settings, where DRG doesn’t apply.
It depends on how specific the documentation is. H52.7 (Unspecified disorder of refraction) applies when the note simply mentions a refractive error without further detail. When the record documents transient refractive change, drug-induced refractive change, accommodative excess, accommodative fatigue, or anisophoria, ICD-10 Code H52.6 is the more specific and defensible choice.
No. Convergence insufficiency has its own code, H51.11, under the H51 category for disorders of binocular movement. Accommodative fatigue falls under H52.6 instead. Amplitude-of-accommodation testing is what separates the two conditions on the chart, since they share overlapping symptoms.