ICD-10 code M17.2: Bilateral post-traumatic osteoarthritis of knee
ICD-10 Code M17.2 is a billable diagnosis code for bilateral post-traumatic oste...
Last Updated: July 29, 2026
ICD-10 code H49.12 is a billable diagnosis code for fourth [trochlear] nerve palsy of the left eye, valid for FY2026 HIPAA-covered transactions.
H49.12 sits under the H49.1 parent code; laterality subcodes run H49.10 (unspecified), H49.11 (right), H49.12 (left), and H49.13 (bilateral).
Parent code H49 carries a Type 2 Excludes note, meaning both H49.12 and the excluded code may be reported simultaneously when clinically appropriate.
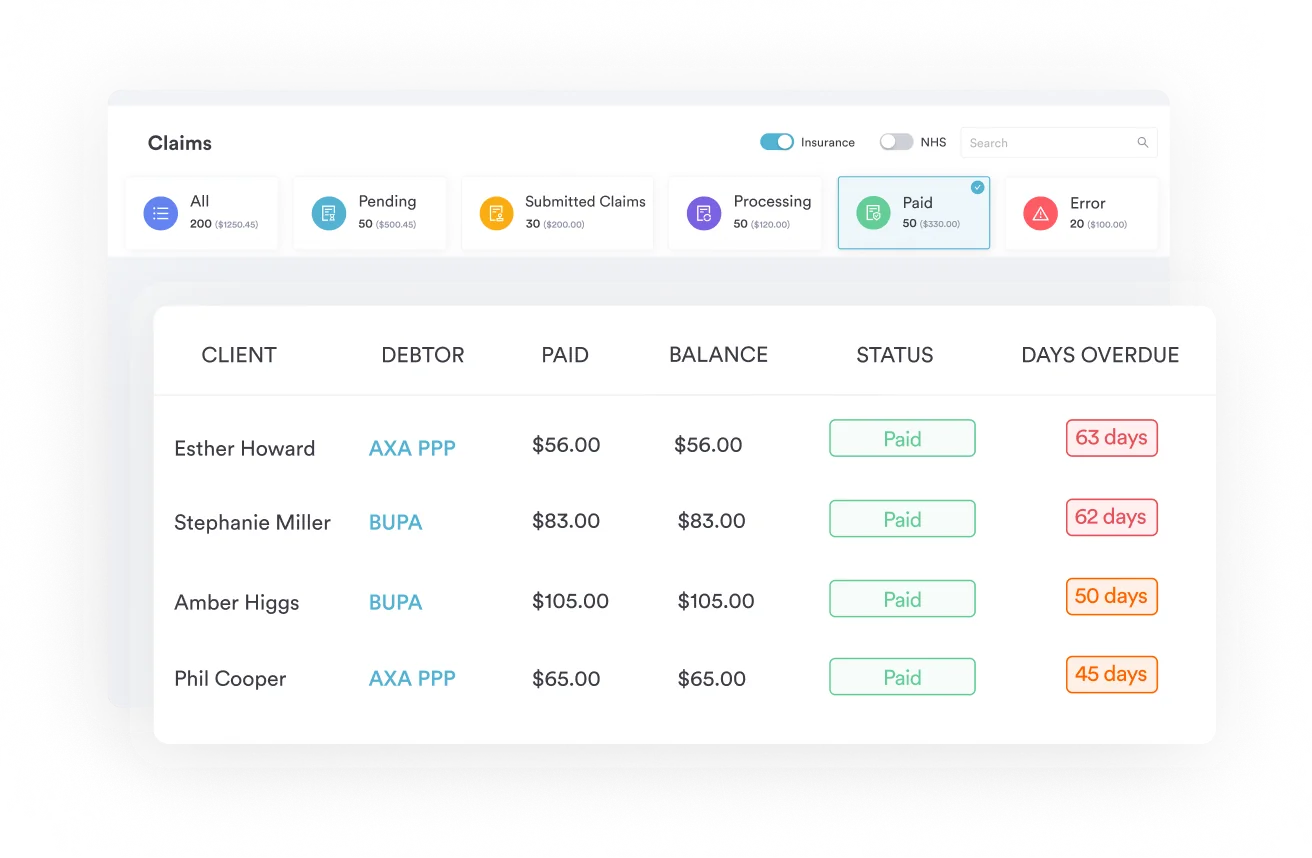
Pabau’s claims management software lets ophthalmology practices attach H49.12 directly to clinical notes and insurance claims, reducing manual coding errors.
ICD-10 code H49.12 is the billable diagnosis code for fourth [trochlear] nerve palsy of the left eye, valid for FY2026 claims. Because H49.1 splits by laterality, payers scrutinize eye selection closely — coding the wrong eye or defaulting to unspecified H49.10 is a common reason these claims are denied.
This guide covers where H49.12 sits in the ICD-10-CM hierarchy, how it differs from the other laterality subcodes under H49.1, and what the clinical documentation needs to say to support it on a claim.
ICD-10 code H49.12 is the billable diagnosis code for fourth [trochlear] nerve palsy of the left eye. Coders and clinicians use it to document paralysis or paresis of cranial nerve IV affecting the left eye specifically, making laterality documentation a hard requirement for accurate claim submission.
The trochlear nerve controls the superior oblique muscle, which depresses and intorts the eye. When it is damaged, patients typically present with vertical diplopia, a compensatory head tilt away from the affected side, and cyclodeviation.
Most ophthalmologists and neuro-ophthalmologists recognize the classic presentation: a patient tilts their head to the right when the left trochlear nerve is compromised. Capturing this laterality with AI-assisted treatment notes at the point of care prevents downstream denials.
H49.12 falls within ICD-10-CM Chapter 7: Diseases of the eye and adnexa (H00-H59), specifically the block H49-H52 covering disorders of ocular muscles, binocular movement, accommodation, and refraction. The parent code is H49.1 (fourth [trochlear] nerve palsy), which is itself a child of H49 (paralytic strabismus).
The same laterality logic shows up in H49.9, the unspecified paralytic strabismus code, where specificity at the sixth or seventh character level is what determines billable status.
H49.12 is a fully billable ICD-10-CM diagnosis code. It is valid for HIPAA-covered electronic transactions from October 1, 2025, covering the FY2026 coding cycle. Per the Centers for Medicare and Medicaid Services (CMS) ICD-10 codes page, the code requires no additional specificity; the sixth-character laterality suffix already satisfies the highest level of coding granularity available under this subcategory.
When submitting claims with H49.12, confirm the code against the CDC/NCHS ICD-10-CM web tool to verify the FY2026 tabular description matches your documentation before submitting to payers.
Selecting the wrong laterality subcode is one of the most common reasons fourth nerve palsy claims are returned. The four subcodes under H49.1 each represent a distinct clinical scenario, and payers expect the code to match the documented examination findings precisely.
The same granularity principle applies to G53, which classifies cranial nerve disorders arising from diseases documented elsewhere in the record.
Key rule: H49.10 should be the code of last resort. CMS guidance and the American Academy of Ophthalmology (AAO) agree that unspecified codes apply only when the record cannot support laterality assignment, never as a default for incomplete documentation.
Coders should query the treating physician before defaulting to H49.10. The same pattern shows up in H50.9, where coders reach for the unspecified code more often than the documentation actually requires.
Before submitting with H49.12, confirm the operative note or consultation letter explicitly states ‘left eye’ or ‘left trochlear nerve palsy.’ A note that says only ‘fourth nerve palsy’ without laterality forces the coder to use H49.10, which many payers treat as a lower-specificity code. Flag the chart for provider clarification before submission rather than defaulting to unspecified.
Accurate coding of H49.12 depends on clinical documentation that clearly establishes three things: the nerve affected, the eye affected, and the functional impact on the patient. Incomplete records are the most common trigger for claim denials and audit findings in ophthalmology practices.
For broader guidance on clinical documentation compliance across allied health settings, the same specificity principles apply to eye care billing.
A cranial nerve examination checklist can help standardize how these findings get captured during the encounter, rather than reconstructed later at billing time.
When documentation references only “strabismus” or “diplopia” without identifying the responsible nerve or laterality, H49.12 cannot be supported. Coders should use the more specific clinical record documentation tools available in their EHR to surface laterality requirements at the point of note creation, not retrospectively at billing time.
Fourth nerve palsy rarely presents in isolation from a documented cause. Coders should review the clinical record for underlying etiologies that require their own diagnosis codes alongside H49.12.
For the diabetic etiology specifically, a diabetes eye exam template helps standardize how the ophthalmic exam findings that support the etiology code get recorded.
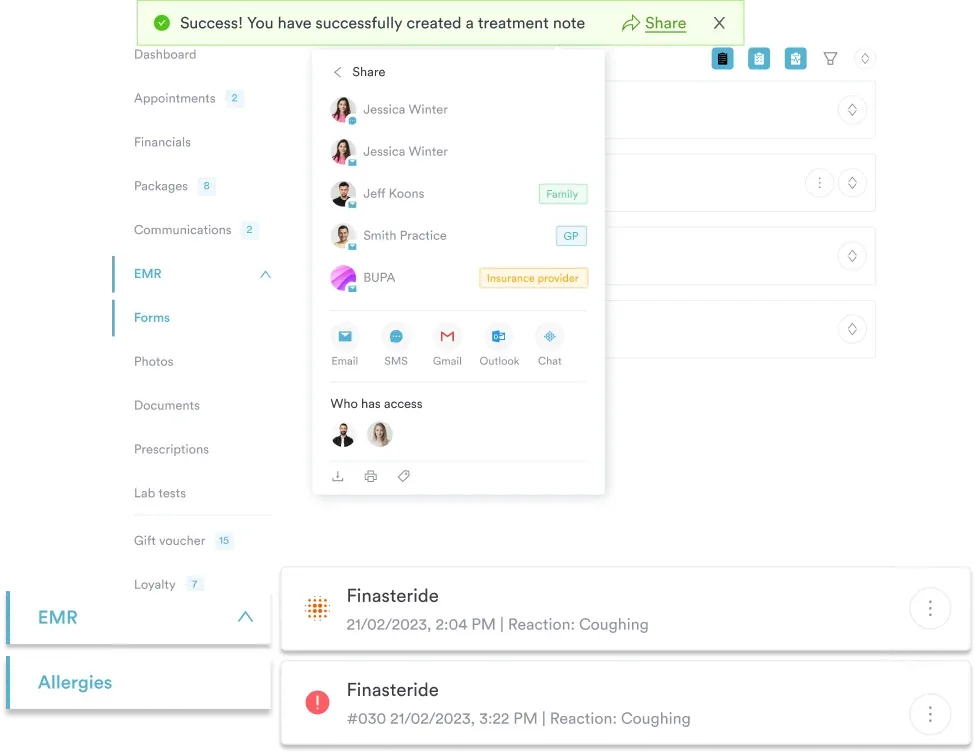
Pabau helps ophthalmology and specialist practices attach diagnosis codes like H49.12 directly within clinical notes, so missing documentation is caught before claims are submitted, not after they are denied.

The parent code H49 (Paralytic strabismus) carries a Type 2 Excludes note. Understanding what this means in practice prevents under-coding and avoids the error of treating the excludes note as a prohibition.
A Type 2 Excludes note indicates that the excluded condition is not part of the coded condition, but a patient may have both at the same time. Under H49, that means H49.12 and the excluded code can be reported together on the same claim when both conditions are documented and relevant to the encounter.
This differs from a Type 1 Excludes note, which sets a hard rule: if a Type 1 Excludes note applies, the two codes cannot be reported together.
For patient care documentation purposes, the treating clinician should explicitly document both conditions in the encounter note when dual coding is intended. Undocumented dual coding is an audit risk regardless of the type of excludes note.
When H49.12 is coded alongside an underlying etiology (such as diabetic cranial mononeuropathy), official ICD-10-CM sequencing guidelines generally require the etiology code to be listed first, with H49.12 as a manifestation code. Always verify sequencing against the most current AAPC Codify ICD-10-CM guidelines and the payer’s specific LCD policy, as sequencing requirements can vary by payer and encounter type.
When billing H49.12 for a patient with a confirmed underlying cause such as diabetes or a head trauma, review the payer’s Local Coverage Determination (LCD) on the CMS Medicare Coverage Database before submission. Some LCDs for strabismus evaluation and management services require the primary diagnosis to be from the condition causing the palsy, with H49.12 listed as a secondary code.
Ophthalmology coders regularly encounter codes adjacent to H49.12 in the H49 category. Knowing where each fits helps avoid substituting the wrong code when laterality or nerve identification differs. The WHO’s ICD classification framework groups these systematically under paralytic strabismus for this reason.
Coders sometimes also confuse H49.12 with H51.0, which covers conjugate gaze palsy rather than an isolated cranial nerve deficit. The exam findings distinguish the two: an isolated trochlear palsy affects only the superior oblique, while a gaze palsy limits movement of both eyes in the same direction.
The ICD List free lookup tool is useful for confirming adjacent codes within the H49 category, including DRG groupings that may apply when the palsy is managed in an inpatient setting. For HIPAA-compliant billing workflows, every code submitted must be supported by documentation in the clinical record, not inferred from a previous encounter.
H49.12 is a diagnosis code, not a procedure code, so it always pairs with a CPT or HCPCS procedure code on the claim. The CPT codes most commonly reported alongside a fourth nerve palsy diagnosis reflect the clinical services an ophthalmologist or neuro-ophthalmologist typically performs.
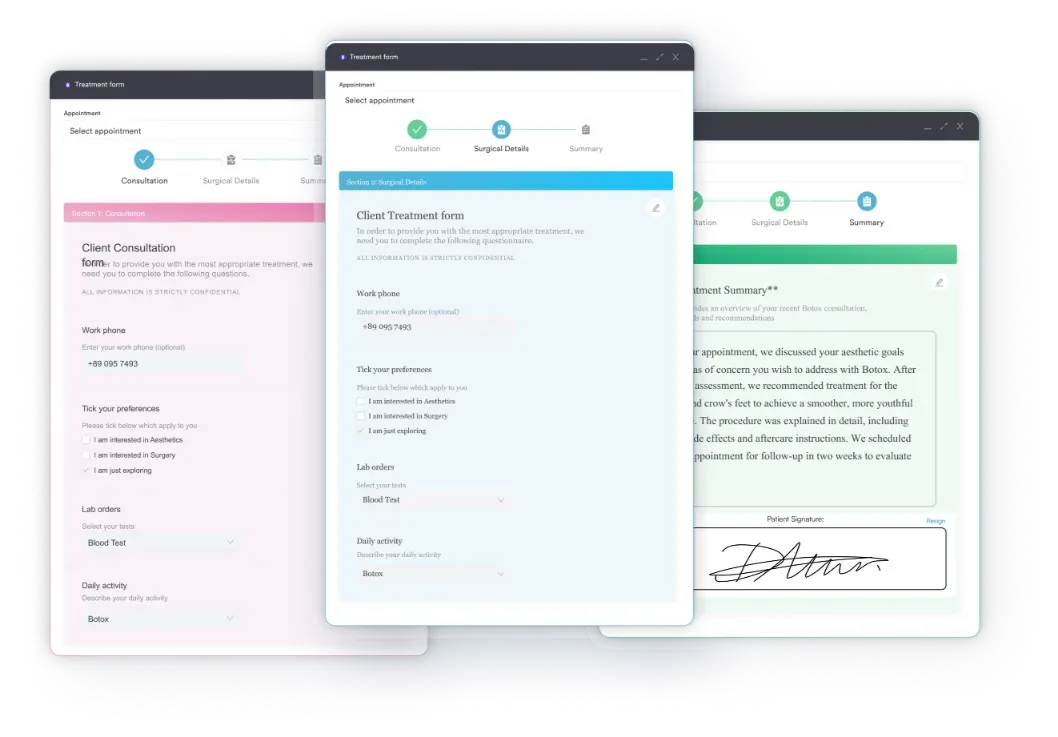
Using digital intake forms that capture presenting symptoms before the encounter helps ensure the procedure codes selected reflect the actual clinical complexity documented.
Practices should verify CPT-to-diagnosis medical necessity alignment against their payer’s LCD before submission. Mismatch between the procedure code’s implied clinical need and the diagnosis code’s specificity is one of the leading causes of ophthalmology claim rejection, particularly when an E&M code like 99214 is billed without documentation supporting that level of complexity.
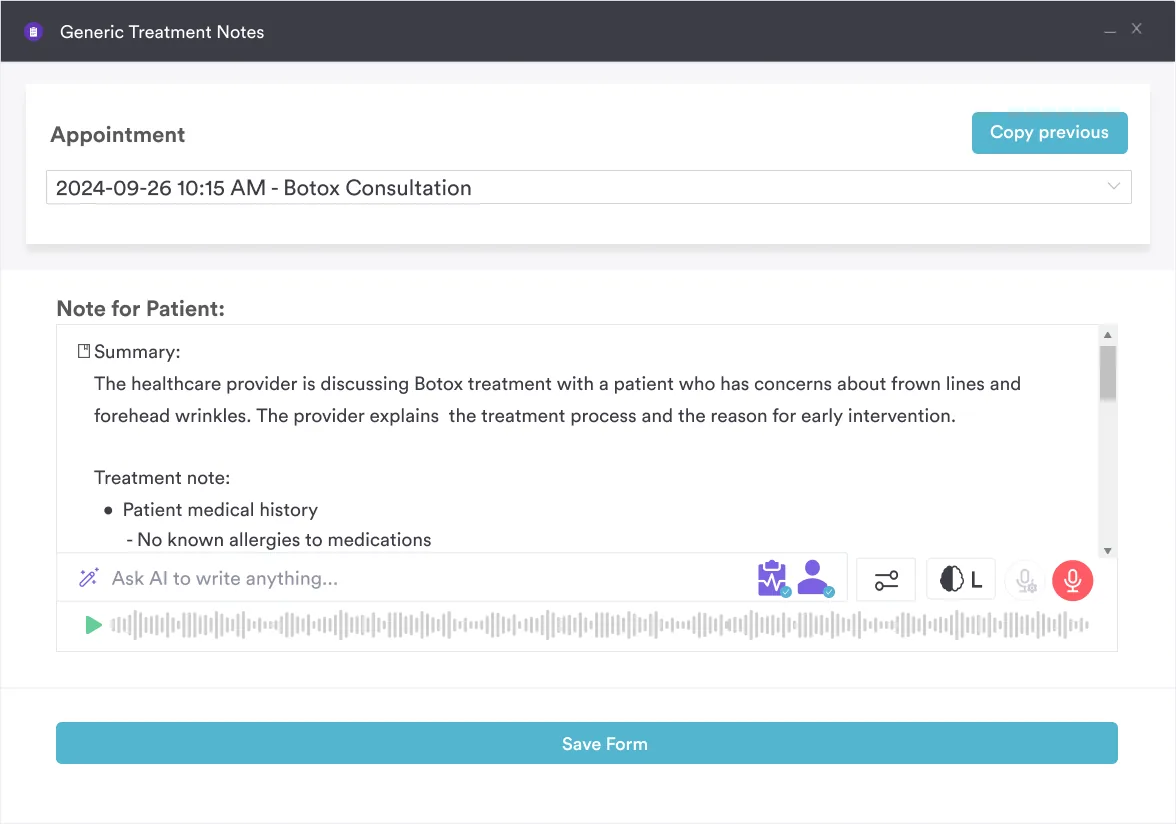
Claim denials for fourth nerve palsy coding are almost always preventable. The most effective practices build laterality verification into the clinical workflow itself, not the billing workflow after the fact. Using AI-assisted clinical documentation that prompts for laterality at the point of note creation removes the main source of coding ambiguity before it reaches the claims queue.
Most fourth nerve palsy claims that get denied share a single root problem: laterality is either missing from the clinical note or coded at the unspecified level when the record supports something more specific. H49.12 solves that problem for left-eye presentations, but only when the underlying documentation matches what the code asserts.
Pabau’s claims management software helps ophthalmology practices catch these issues before submission, linking diagnosis codes directly to clinical notes so laterality, sequencing, and CPT-to-ICD alignment are verified at the source. To see how it works for your billing team, book a demo.
Need to streamline your ophthalmology practice billing? End-to-end claims tracking covers claim submission and denial tracking for specialist practices.
Looking for guidance on clinical documentation standards? Safer clinical notes covers best practices for structuring encounter documentation to support accurate coding.
Want to reduce manual coding errors across your team? Pabau Scribe, our AI scribe, assists clinicians with note creation, shortening the distance between clinical encounter and coded claim.
ICD-10 code H49.12 is used to document a diagnosis of fourth [trochlear] nerve palsy affecting the left eye, a condition where cranial nerve IV is damaged and the superior oblique muscle cannot function normally. Clinicians and coders use it when the clinical record explicitly confirms left-sided involvement, distinguishing it from right-eye (H49.11), bilateral (H49.13), and unspecified (H49.10) presentations. It is valid for FY2026 HIPAA-covered transactions.
All four codes describe fourth [trochlear] nerve palsy but differ by laterality. H49.10 is unspecified eye and should be used only when laterality cannot be established from the clinical record. H49.11 is right eye, H49.12 is left eye, and H49.13 is bilateral, often seen after head trauma affecting both trochlear nerves. Payers increasingly require the laterality-specific code; defaulting to H49.10 when documentation supports a specific eye is a common audit finding.
Yes. H49.12 is fully billable and valid for HIPAA-covered electronic transactions from October 1, 2025 through the FY2026 cycle. No additional specificity beyond the sixth character is required. The code can be submitted directly on a CMS-1500 or electronic 837P claim when supported by adequate clinical documentation establishing left-eye trochlear nerve involvement.
The most frequently paired CPT codes are 92004 or 92014 (comprehensive ophthalmological examination for new or established patients), 92060 (sensorimotor examination with prism measurements), and E&M codes 99213-99215 when the encounter is billed under the E&M framework. Strabismus surgery CPT codes (67311-67316) apply when surgical correction is performed. Always verify medical necessity alignment with the relevant payer LCD before submission.
The clinical note must explicitly name the fourth (trochlear) nerve or cranial nerve IV, state left eye involvement, and record objective findings such as vertical diplopia, head tilt direction, or hypertropia measured in prism diopters on cover testing. Notes referencing only “strabismus” or “diplopia” without nerve and laterality identification do not support H49.12. If an underlying cause (trauma, diabetes, neoplasm) is documented, it should also be coded and sequenced appropriately.
Yes. When a confirmed etiology exists, such as diabetic cranial mononeuropathy or traumatic nerve injury, both H49.12 and the underlying condition code should be reported. Per ICD-10-CM official sequencing guidelines, the etiology code is generally listed first and H49.12 as an additional code. The Type 2 Excludes note under the parent H49 category confirms that dual reporting is permitted when both conditions are clinically present.