Tight hip flexors test: How to do the Thomas Test
Front-of-hip tightness is easy to feel and hard to pin down. You stretch, it eas...
Last Updated: August 11, 2026
A diabetes eye exam is a comprehensive dilated and retinal assessment performed by an optometrist or ophthalmologist to screen for diabetic retinopathy, macular edema, glaucoma, and cataracts.
The American Diabetes Association recommends an initial dilated exam at diagnosis for type 2 diabetes, or within 5 years of onset for type 1 diabetes; the interval may extend to every 2 years after one or more annual exams show no retinopathy and glycemia is well controlled. Medicare Part B covers one exam per year.
NCQA HEDIS EED documentation requires recording specific findings: visual acuity, intraocular pressure, retinal photography or dilated exam evidence, and absence/presence of diabetic retinal disease.
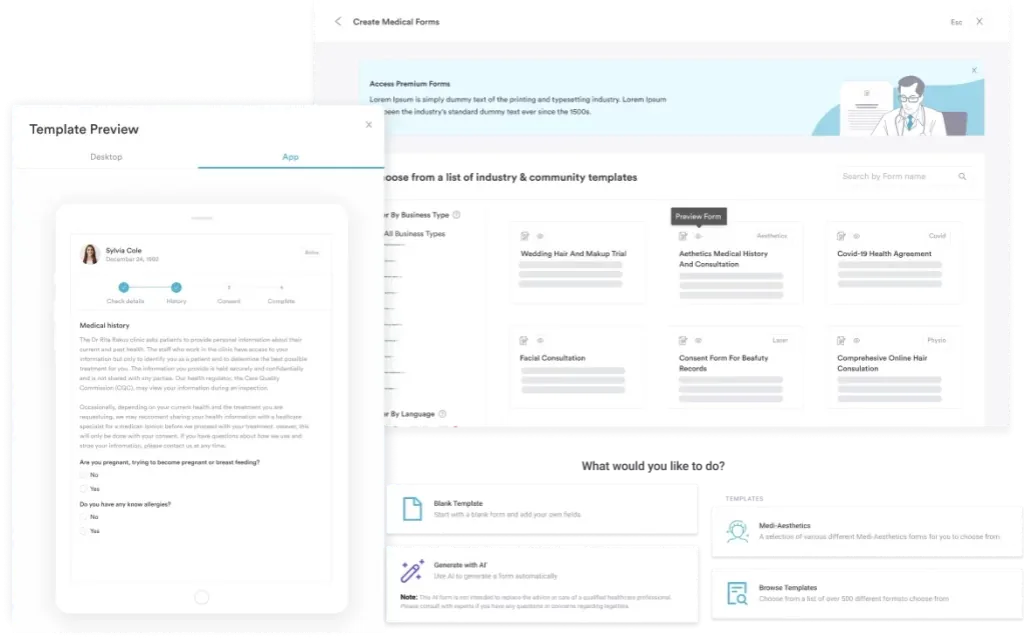
Structured documentation via digital forms or templates like Pabau’s accelerates compliance reporting, reduces coding errors, and enables automated MIPS Measure 117 quality tracking for practices.
A ready-to-use diabetes eye exam form covering visual acuity, dilated fundus assessment, retinal photography documentation, HEDIS EED compliance checkboxes, diabetic retinopathy grading (NPDR/PDR), ICD-10 coding fields, and referral sections for endocrinologists and primary care teams.
Download templateDiabetes is the leading cause of vision loss in people aged 18-64, yet early detection through structured eye exams can prevent or reverse sight-threatening complications. A comprehensive diabetes eye exam combines clinical assessment with documented findings that satisfy both regulatory requirements (HEDIS EED, MIPS Measure 117) and clinical best practices.
This guide covers what a diabetes eye exam encompasses, how to perform one systematically, and how to document findings in a way that supports patient care, compliance reporting, and team communication. Whether you are an optometrist, ophthalmologist, or referring clinician, a structured template ensures no critical findings are missed and payer documentation requirements are met every time.
A diabetes eye exam is a specialized dilated and comprehensive eye assessment that focuses on detecting diabetes-related complications affecting ocular health. Unlike a routine vision check, a diabetes eye exam systematically screens for:
The clinical purpose is early detection. Screening and early treatment can often halt or reverse the level of diabetic retinal disease, protecting vision. Regulatory bodies including the National Committee for Quality Assurance (NCQA) mandate documentation of these findings as part of the HEDIS EED (Eye Exam for Patients with Diabetes) measure, which tracks quality of diabetes care across health plans.
For clinicians, a structured diabetes eye exam template ensures comprehensive documentation that supports both clinical decision-making and compliance with payer requirements. Digital forms within practice management systems streamline data capture and reduce transcription errors.
A systematic approach ensures consistency and completeness. Start by capturing the patient’s diabetes history and intake details (diabetes type, duration, most recent HbA1c, and current medications), then work through this operational sequence:
Using a diabetes eye exam template or integrated appointment scheduling with pre-populated form fields accelerates this workflow, ensures no steps are skipped, and produces documentation ready for payer submission.
According to NCQA and CMS eCQM specifications, a qualified eye care professional must perform the exam. This includes:
Primary care clinicians (GPs, internists, endocrinologists) may screen for gross visual changes or refer patients; however, they typically cannot bill for the formal dilated exam unless they have specific training. Practices integrating endocrinology and preventive care often partner with local optometrists or ophthalmologists to ensure timely referral and coordinated documentation.
Structured documentation delivers operational and clinical gains:
Flag exams with vision-threatening findings (PDR, DME with foveal involvement, severe glaucoma) for same-day or next-day specialist referral. Many practices integrate automated SMS/email alerts into their workflow software to notify referring providers immediately when urgent pathology is detected.
The HEDIS EED measure applies to all adults aged 18-75 with type 1 or type 2 diabetes. For compliance, documentation must capture:
For MIPS Measure 117 (Diabetes: Eye Exam), clinicians must report the percentage of their diabetic patients who had a documented eye exam. Practices using HIPAA-compliant EMRs with structured clinical records can extract this data automatically and submit via MIPS registry or EHR vendor.
A diabetes eye exam template ensures all required fields are present before the clinician hits “Save,” eliminating incomplete submissions and audit flags.
Accurate coding supports billing and research tracking. Common codes for diabetes-related eye conditions include:
The template guides coders to select the appropriate code based on retinopathy severity and DME presence, reducing the risk of under-coding (losing revenue) or over-coding (triggering audits). Always verify codes against the current ICD-10-CM edition, as coding updates occur annually.
Structured templates, automated compliance reporting, and integrated patient communication in one platform.

Different professional bodies publish slightly different diabetic eye exam guidelines, so understanding both sets of diabetes eye exam frequency recommendations keeps your practice aligned with evidence-based standards:
Both organizations emphasize that Medicare Part B covers one dilated eye exam annually for people with diabetes. A well-designed template includes a “Next Exam Date” field that auto-populates based on current findings, ensuring your team schedules follow-up appropriately and patients do not miss critical screening windows.
In many clinics, endocrinologists or primary care physicians order diabetic eye exams, but the exam is performed by a local optometrist or ophthalmologist. Coordinated documentation is essential:
Using a standardized template ensures both the eye care professional and the referring clinician document in a format that integrates seamlessly into the shared record, reducing missed communication and duplicated testing.
Early stages of diabetic retinopathy often cause no symptoms. By the time a patient notices blurred vision, significant retinal damage may already be present. Routine, structured diabetes eye exams catch complications before vision is compromised:
Diabetic retinopathy progression can be slowed, halted, or in some cases reversed with aggressive glycaemic, blood pressure, and lipid control. Practices that organize diabetes eye exam workflows with templates report higher completion rates, faster specialist referrals, and better patient compliance with follow-up appointments.
Need a framework for structuring your clinic’s diabetes care workflow? Clinic management software guides explain how scheduling, EMR templates, and automated referrals work together to ensure no patient misses their annual screening.
Want to track compliance metrics for your practice? Pabau Insights Plus provides automated quality reporting, including HEDIS EED completion rates and MIPS Measure 117 tracking so you always know your compliance standing.
Looking to improve documentation speed and accuracy? Data protection best practices for clinics demonstrate how secure, structured EMRs protect patient privacy while speeding up clinical workflows and reducing documentation burden.
A structured diabetes eye exam template is the backbone of consistent, compliant diabetic retinal screening. By standardizing documentation, practices ensure that vision-threatening complications are caught early, regulatory requirements are met, and teams can coordinate seamlessly across providers.
The free template above covers every element required for clinical decision-making and payer compliance-visual acuity, IOP, retinal findings, HEDIS EED checkboxes, ICD-10 coding, and referral pathways. Integrating this template into your practice management system (such as Pabau’s digital forms and clinical records) eliminates blank fields, reduces time per exam by 10+ minutes, and keeps your team aligned on follow-up care. Book a demo to see how Pabau streamlines diabetic care workflows and automates compliance reporting so your practice never misses a screening or fails an audit.
A diabetes eye exam is a comprehensive dilated eye assessment performed by an optometrist or ophthalmologist to screen for retinopathy, macular edema, glaucoma, and cataracts.
Recommendations differ by diabetes type. For type 2 diabetes, the American Diabetes Association recommends an initial dilated exam at the time of diagnosis. For type 1 diabetes, the initial exam should take place within 5 years of disease onset. After one or more annual exams with no retinopathy and well-controlled glycemia, the interval may be extended to every 2 years. If retinopathy is detected, annual exams are recommended. Medicare Part B covers one dilated eye exam per year for people with diabetes.
A diabetes eye exam detects diabetic retinopathy, diabetic macular edema, glaucoma, cataracts, and other retinal or optic nerve changes related to diabetes.
Yes — Medicare Part B covers one dilated and comprehensive eye exam per year for people with diabetes, performed by a licensed optometrist or ophthalmologist.
Documentation must include a dilated eye exam, visual acuity, intraocular pressure, presence or absence of retinopathy, exam date, and provider name.
Include visual acuity, intraocular pressure, anterior segment and dilated retinal findings, retinopathy grade, imaging results, recommended follow-up interval, and any urgent referrals.
A routine eye exam checks vision and screens for common eye conditions, while a diabetic eye exam adds a dilated retinal assessment focused on diabetic retinopathy, macular edema, and vascular changes. It also captures the visual acuity, intraocular pressure, and retinopathy findings that HEDIS EED and MIPS reporting require.
Yes. Retinal changes such as microaneurysms, small hemorrhages, or leaking blood vessels can show up during a dilated exam before a patient has been diagnosed, prompting a referral for blood glucose testing.
Ultra-widefield retinal imaging can screen for retinopathy without drops in some cases, but a dilated fundus exam remains the standard for a complete assessment and for meeting documentation requirements.
Coding depends on the findings: Z01.00 or Z01.01 for the screening encounter, E11.9 for type 2 diabetes without retinopathy, and the E11.3 series when retinopathy or macular edema is present.
Most exams run 30 to 60 minutes, including the 20 to 30 minutes needed for dilating drops to take effect. Vision stays blurry for a few hours afterward, so patients should arrange a ride home.