Amniocentesis test documentation records prenatal diagnostic fluid withdrawal between 15-20 weeks of pregnancy to screen for chromosomal disorders and genetic conditions in the fetus.
Proper documentation of needle insertion attempts, ultrasound guidance, amniotic fluid volume, and sample chain of custody is mandatory for clinical accuracy, liability protection, and regulatory compliance per ACOG and NIH standards.
The template captures pre-procedure consent (including risk disclosure for the approximately 0.1%–0.13% (about 1 in 769–900) miscarriage risk), intra-procedure data (needle passes, ultrasound confirmation, fluid volume), and post-procedure monitoring instructions and result communication.
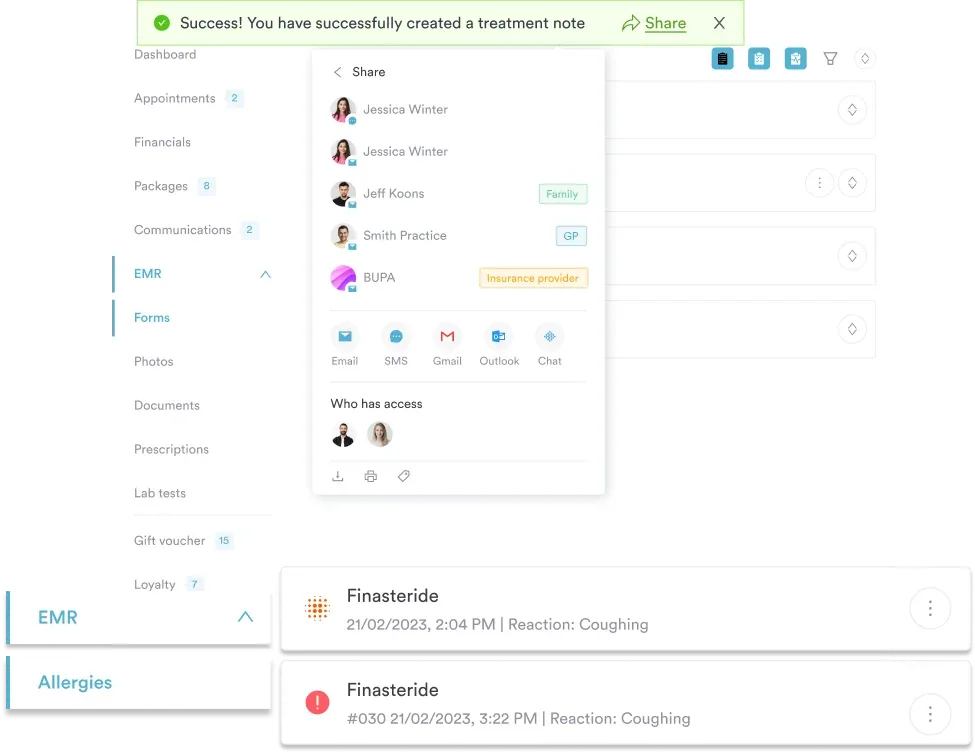
Practice management software like Pabau lets practices complete amniocentesis test documentation electronically, so digital consent forms and patient records capture every field systematically and store it in a HIPAA-compliant way without the paper burden.
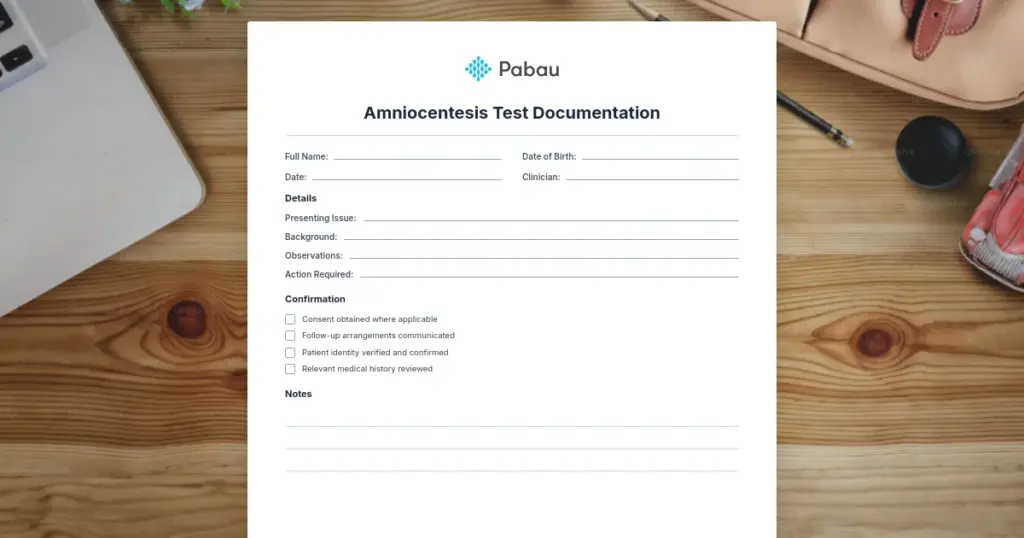
Download your free amniocentesis documentation template
A ready-to-use prenatal procedure form covering patient details, test indications, ultrasound guidance fields, needle insertion attempt logging, amniotic fluid volume measurement, sample chain of custody, and post-procedure monitoring instructions aligned with ACOG and NIH documentation standards.
Amniocentesis test documentation is the clinical record of a prenatal diagnostic procedure, typically performed between 15–20 weeks of pregnancy. Complete, standardized records determine whether results are defensible, auditable, and actionable for the patient and their care team.
What is amniocentesis test documentation?
Amniocentesis test documentation is a clinical record that captures every element of a prenatal diagnostic procedure performed under ultrasound guidance. The procedure involves inserting a thin needle through the maternal abdomen and uterine wall to withdraw 15-20 mL of amniotic fluid for laboratory testing.
Structured medical forms for amniocentesis serve three critical functions: (1) informed consent and risk disclosure, (2) real-time intra-procedure data capture, and (3) result communication and post-procedure monitoring instructions. Each function has legal, clinical, and laboratory implications.
According to NIH StatPearls, proper procedure documentation is mandatory: the number of needle insertion attempts, ultrasound guidance confirmation, amniotic fluid volume, and specimen chain of custody must all be recorded.
Missing or vague documentation undermines diagnostic accuracy claims, complicates result interpretation, and exposes practices to regulatory findings and malpractice liability. For related prenatal screening forms, see the Down Syndrome Test Form for a complementary documentation reference.
Informed consent component: Discloses procedure indications, technical steps, risks (including the approximately 0.1%–0.13% miscarriage risk, about 1 in 769–900, per current ACOG/SMFM guidance), alternatives, and expected result turnaround time.
Procedure documentation component: The amniocentesis procedure note records patient positioning, ultrasound-confirmed needle approach, number of insertion attempts, fluid volume withdrawn, and specimen labeling for laboratory chain of custody.
Result communication component: Documents which genetic tests (karyotype, FISH, chromosomal microarray) were performed, interpretation of findings, and counseling provided to the patient about results. Many practices deliver results through a patient portal to speed communication and confirm receipt.
Post-procedure monitoring: Records follow-up instructions, signs of complication (amniotic fluid leakage, cramping, infection), and patient contact information for urgent concerns. Confirming reassuring fetal heart tones before discharge is standard practice; see the normal fetal heart rate template for a compatible monitoring reference.
How to use amniocentesis test documentation in your practice
A complete amniocentesis test documentation workflow spans five operational steps, from pre-procedure planning through post-procedure follow-up. Each step integrates specific documentation fields and clinical decision points.
Step 1: Pre-procedure assessment and consent (1–2 weeks before). Record maternal age, obstetric history, indication for testing, and blood type/Rh factor. Note contraindications (active infection, inaccessible placenta, refusal). Obtain informed consent documenting risk disclosure — procedure-related miscarriage risk (approximately 0.1%–0.13%, about 1 in 769–900, per ACOG/SMFM Practice Bulletin 162) and diagnostic (amniocentesis) vs. screening-only (NIPT) approaches. If Rh-negative, document RhoGAM given within 72 hours per ACOG.
Step 2: Procedural planning and ultrasound (day of procedure). Before needle insertion, confirm gestational age, viability, placental location, fluid volume, and safe needle approach. Document findings and planned approach (transabdominal; anterior vs. posterior placenta). Position patient and prep abdomen with sterile technique.
Step 3: Needle insertion and fluid withdrawal (intra-procedure). Under continuous ultrasound guidance, insert a 22-gauge spinal needle into the amniotic sac. Document: entry location, number of attempts, depth fluid was encountered, volume withdrawn (15–20 mL), fluid color/clarity, specimen labeling with identifiers and time, and any maternal pain or fetal movement.
Step 4: Specimen handling and chain of custody. Record tube type and additives (sterile for culture, EDTA for cytogenetics), specimen temperature, transport time, and receiving technician’s name/credentials. Note tests ordered (karyotype, FISH for trisomy 13/18/21, microarray) and turnaround (7–14 days culture; 24–48 hours FISH).
Step 5: Post-procedure monitoring and results (1–2 weeks after). Give written instructions: rest 24 hours, avoid strenuous activity 48 hours, report clear fluid leakage, heavy bleeding, fever ≥38°C, or severe cramping. Schedule follow-up ultrasound at 48–72 hours. On results, document genetic counseling, patient understanding (normal/abnormal/VUS), next steps, any MFM or pediatrics referral, and the patient’s elected management or continuation plan.
Using patient record management software with structured data entry ensures every field is completed systematically. Amniocentesis test documentation embedded in the patient’s digital record prevents data loss and enables rapid retrieval during follow-up visits, transfer of care, or regulatory audit.
Clarifying who manages electronic health records within your practice keeps these responsibilities assigned across clinicians, lab staff, and administrative teams.
Comprehensive EMR & patient record management.
Ready to streamline prenatal procedure documentation?
See how Pabau's digital forms and patient records simplify amniocentesis test documentation for OB-GYN practices.
Amniocentesis test documentation is essential for any OB-GYN practice offering invasive prenatal diagnosis. Primary users include:
Maternal-fetal medicine (MFM) specialists – perform amniocentesis procedures and oversee documentation accuracy for diagnostic claims and patient safety.
OB-GYN clinicians in private practice – provide full obstetric care including genetic counseling and invasive testing for patients with abnormal screening results or family history.
Fertility and IVF practices – coordinate amniocentesis timing post-conception and result interpretation for high-risk pregnancies, often alongside an infertility consultation notes template for continuity of care.
Genetic counselors – integrate amniocentesis results into reproductive genetic risk assessment and patient decision-making conversations.
Prenatal diagnostic center coordinators – manage scheduling, consent, specimen transport, result reporting, and patient follow-up across multiple clinicians and laboratories.
Benefits of standardized amniocentesis test documentation
Standardized amniocentesis test documentation delivers measurable outcomes for maternal-fetal medicine practices:
Regulatory compliance and audit readiness: ACOG clinical practice bulletins and ACOG amniocentesis guidance explicitly recommend documented informed consent, procedural details, and result tracking. Standardized documentation passes CMS audits, CLIA laboratory inspections, and state health department reviews.
Clinical accuracy: Systematic recording of needle insertion attempts, fluid volume, and specimen chain of custody enables laboratory validation of results and confidence in reporting. When a test comes back abnormal, the clinical record demonstrates that proper procedure technique was followed.
Liability protection: Comprehensive consent documentation showing that the approximately 0.1%–0.13% (about 1 in 769–900) miscarriage risk was disclosed, understood, and accepted protects against wrongful birth litigation. Procedure documentation demonstrating careful technique (single needle pass, adequate fluid volume, immediate specimen handling) supports the defensibility of any adverse outcome.
Operational efficiency:Compliance documentation integrated into a digital system eliminates paper forms, reduces transcription errors, and enables quick retrieval of prior amniocentesis records when patients return for subsequent pregnancies or require transferred care. Pairing this with dedicated medical billing software also reduces claim denials tied to incomplete procedure documentation.
Patient safety: Clear post-procedure monitoring instructions and rapid access to emergency contact details enable early detection and management of rare complications (amniotic fluid leakage, infection, preterm labor).
Data quality for quality improvement: Amniocentesis records aggregated across your practice’s procedures enable tracking of success rates (single-pass vs. multiple-attempt rates), complication rates, and result accuracy — metrics required by many credentialing bodies and malpractice carriers.
Pro Tip
Document the exact number of needle insertion attempts during amniocentesis — this is the single most important procedural detail. Studies show that multiple-pass procedures (≥2 attempts) carry a slightly higher risk of complications. Recording this detail protects your practice’s quality metrics and supports transparent discussion of risks if any adverse outcome occurs.
Informed consent requirements in amniocentesis documentation
Informed consent is the legal and ethical cornerstone of any amniocentesis procedure. Your documentation template must capture five essential consent elements:
Indication: Why is amniocentesis being offered? (e.g., abnormal quad screen, advanced maternal age, prior trisomy pregnancy, family history of genetic disorder).
Procedure steps: Clear description of what happens: ultrasound guidance, needle insertion through abdomen and uterus, fluid withdrawal, specimen labeling.
Risks: Miscarriage risk (approximately 0.1%–0.13%, about 1 in 769–900, per ACOG/SMFM Practice Bulletin 162 — older estimates of 1 in 300–500 or higher are now considered outdated), rare infection, amniotic fluid leakage, maternal bleeding, needle injury to fetus (extremely rare with ultrasound guidance).
Benefits: High analytic sensitivity (laboratory detection rate >99% for full trisomy 21 with standard karyotype analysis, subject to rare culture failure or mosaicism limitations), rapid results for FISH testing, ability to plan for affected births or pursue further counseling.
Alternatives: Non-invasive prenatal testing (NIPT), standard ultrasound screening, expectant management with serial monitoring, termination of pregnancy if major anomaly detected.
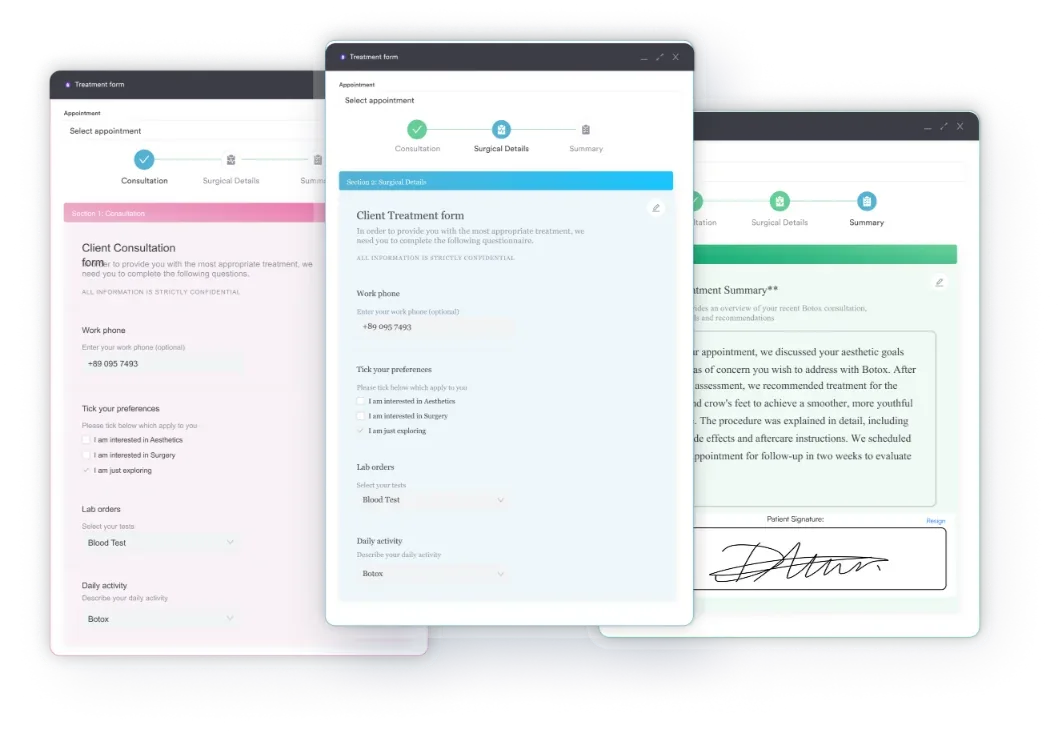
Many practices build these five elements into a single digital amniocentesis consent form embedded in their EMR, so risk disclosure stays consistent and complete and the patient signs on the spot. Digital forms also timestamp consent and record any questions the patient asked, which is valuable documentation if a dispute arises later.
When results are shared with a referring physician or outside laboratory, pair consent with a HIPAA authorization form to document the patient’s release of records.
Customizable consent and intake forms.
ACOG, NIH, and CLIA documentation standards
Your amniocentesis test documentation template should align with these authoritative standards:
ACOG Practice Bulletin #162 (Prenatal Diagnostic Testing for Genetic Disorders, 2016, reaffirmed 2022): Recommends detailed consent documentation, ultrasound confirmation of fetal viability and placental location, post-procedure monitoring instructions, and result communication protocols. ACOG does not mandate a specific form but requires documentation of all elements listed above.
NIH/NCBI StatPearls (Diagnostic Amniocentesis module): Emphasizes that “the number of needle insertion attempts should be recorded” and “ultrasonography before the procedure is done.” The StatPearls review highlights that proper documentation is necessary for clinical governance and legal defensibility.
CLIA laboratory requirements: Laboratories performing cytogenetic testing on amniocentesis fluid require specimen chain of custody documentation: patient identifiers, collection date/time, specimen type and volume, transport conditions, accession number, and testing performed. Your practice’s template must capture these fields to meet CLIA oversight.
State-specific informed consent laws: Some US states (e.g., California, New York) have specific legal requirements for genetic testing consent. Document which state’s requirements your consent form meets and update annually to reflect any legislative changes.
Staff training and documentation standardization
Rolling out amniocentesis test documentation across your practice requires staff training on form completion and procedure technique. Key training topics:
Why each documentation field matters (informed consent, procedure safety, laboratory validation, audit readiness)
How to complete consent forms accurately and obtain genuine informed patient signature
Technical procedure steps and real-time ultrasound-guided needle insertion documentation
Specimen handling, labeling, and chain of custody procedures for laboratory submission
Post-procedure monitoring instructions and complication recognition (fluid leakage, fever, bleeding, severe cramping)
Result interpretation and patient counseling workflows when abnormal findings are reported
Structured clinical note formats embedded in your EMR reduce variation and ensure consistent documentation across all staff and all procedures. Standardized amniocentesis documentation makes audits straightforward and quality improvement data-driven.
Conclusion
Amniocentesis test documentation is the clinical and legal record that protects both your patients and your practice. Comprehensive documentation of informed consent, procedure technique, specimen handling, and result communication enables your maternal-fetal medicine team to offer invasive prenatal diagnosis with confidence, audit readiness, and liability protection.
Download the template above and customize it to your practice’s workflow, then integrate it into your patient record system so every amniocentesis procedure is documented consistently and completely.
Practices billing related obstetric care episodes can also reference the CPT Code 59510 guide for routine obstetric care, cesarean, and postpartum billing. Book a demo and see how Pabau’s digital forms support amniocentesis test documentation for maternal-fetal medicine practices.
Expert resources for amniocentesis documentation
Continue your research
Need guidance on compliance requirements for prenatal testing?HIPAA-compliant storage of patient records ensures amniocentesis documentation and genetic testing results are protected under federal privacy law.
Looking for tools to capture forms electronically?Digital form capture enables your practice to collect consent and procedure documentation on tablets or desktop systems during the patient visit.
Coding for an unrelated corneal finding? The ICD-10 Code H18.9 guide was recently added to Pabau’s diagnostic coding library.
Need historical billing context? The HCPCS Code G2023 guide covers the deleted COVID-19 specimen collection code.
Frequently asked questions
What is amniocentesis test documentation?
Amniocentesis test documentation is the complete clinical record of a prenatal diagnostic procedure performed between 15-20 weeks of pregnancy. It captures informed consent (including risk disclosure), procedure details (needle insertion, ultrasound guidance, fluid volume), specimen chain of custody, and post-procedure monitoring instructions.
Who needs to document amniocentesis procedures?
Any OB-GYN practice, maternal-fetal medicine practice, or fertility practice offering invasive prenatal diagnosis must document amniocentesis procedures. Documentation is mandatory for regulatory compliance (ACOG, CLIA, state oversight), malpractice liability protection, and laboratory validation of genetic test results.
What should an amniocentesis consent form include?
Informed consent must disclose: the procedure indication, step-by-step description of the technique, risks (including the approximately 0.1%–0.13% (about 1 in 769–900) miscarriage risk per ACOG/SMFM Practice Bulletin 162), benefits, alternatives (such as NIPT or standard screening), and expected result turnaround time. Patient signature and clinician signature must be documented with date and time.
How do I document needle insertion attempts during amniocentesis?
Record the exact number of needle passes required to withdraw amniotic fluid: single-pass success (preferred) or multiple attempts (≥2). Document the anatomic needle entry location, depth to amniotic sac, fluid volume withdrawn, fluid color/clarity, and any maternal or fetal response noted during insertion.
What is chain of custody documentation in amniocentesis?
Chain of custody documents the specimen journey from collection to laboratory analysis: tube type, additives used, collection time/date, specimen volume, temperature during transport, time received by lab, lab technician name, and tests ordered (karyotype, FISH, microarray). This is mandatory for CLIA compliance and laboratory result validation.
How long should I keep amniocentesis documentation?
Retain amniocentesis test documentation for a minimum of 7 years post-delivery (often longer depending on state law and whether the child develops a genetic condition related to testing). Digital archival systems with strong EHR security ensure secure, long-term retention and enable rapid retrieval during subsequent pregnancies or medical record requests.