








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT Code 59510 is a global maternity code covering antepartum care, cesarean delivery, and postpartum care when a single provider manages all three phases.
The global package includes approximately 13 antepartum visits per AMA guidelines, the cesarean delivery, and postpartum follow-up through 6 weeks.
Billing 59510 when antepartum care was provided by a different physician is one of the most common and costly coding errors in OB-GYN practices.
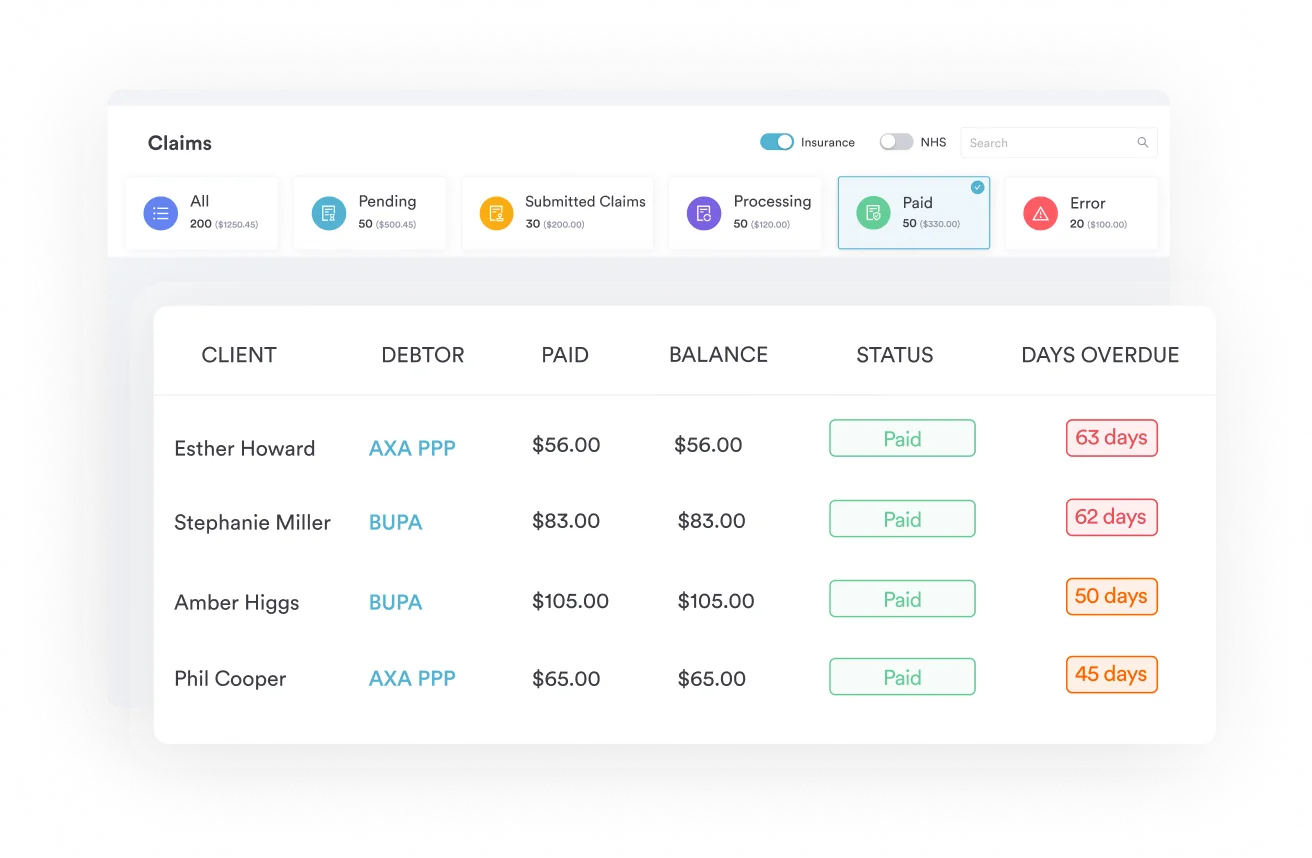
Pabau’s claims management software helps OB-GYN practices track global maternity package components and reduce claim denials before submission.
CPT code 59510 is the global maternity code for routine obstetric care by cesarean, bundling antepartum care, cesarean delivery, and postpartum care into one submission. It applies only when a single provider furnishes all three components for the same pregnancy; otherwise use 59514 or 59515 instead.
2027 CPT update: CPT 59510 and the related global OB codes covered in this guide (59400, 59514, 59515, 59610, 59618, 59425, and 59426) are scheduled for deletion effective January 1, 2027 under the AMA’s CPT 2027 maternity care restructuring. The global codes are being replaced with component-based, per-encounter E/M antepartum billing, new labor-management codes (59080–59083), and new delivery-only codes. CPT 59510 remains valid for dates of service through December 31, 2026 — practices should start adjusting documentation and billing workflows in 2026 to prepare for deliveries occurring in 2027.
CPT Code 59510 falls under the Maternity Care and Delivery section of Current Procedural Terminology, maintained by the American Medical Association (AMA). It is a bundled, single-code solution: one submission covers prenatal visits, the operative delivery, and the six-week postpartum period.
Practices that use OB-GYN EMR software with built-in global package tracking are significantly less likely to unbundle components that should be billed together.
CPT Code 59510 bundles three distinct service components into a single billable unit. Understanding what each component covers prevents incorrect unbundling and protects against National Correct Coding Initiative (NCCI) edit denials.
The AMA defines the antepartum care component as approximately 13 prenatal visits. This includes the initial comprehensive history and physical, subsequent routine prenatal visits, recording weight and blood pressure, fetal heart tones, and routine urinalysis. Visits beyond the 13-visit threshold, or those addressing complications beyond routine prenatal care, may be billed separately using appropriate evaluation and management (E/M) codes.
The delivery component covers the cesarean section itself, including admission to the hospital, the surgical procedure, and management of uncomplicated recovery in the immediate postoperative period.
Multiple gestation does not justify additional units: per AMA (2002) guidance cited by Blue Cross NC, only one unit of a single cesarean code (59510, 59618, 59514, 59515, 59620, or 59622) may be reported regardless of how many babies are delivered through the cesarean incision.
Postpartum care within the global package covers routine follow-up through approximately six weeks after delivery. This typically includes the standard postpartum visit at four to six weeks. The American College of Obstetricians and Gynecologists (ACOG) notes that extended postpartum care beyond the traditional single visit may be separately billable depending on payer policy, particularly for fourth-trimester services.
Choosing the correct cesarean delivery code depends on which components the billing provider actually furnished. Using 59510 when antepartum care was provided by a different practice is one of the most flagged patterns in OB coding audits. The table below shows the key distinctions.
For split-care scenarios where antepartum care transfers mid-pregnancy, modifier -54 (surgical care only) or modifier -56 (preoperative management only) may apply. Practices managing complex split-care billing benefit from claims management software that flags modifier requirements based on provider-of-record data.
Reviewing IVF CPT codes alongside OB global codes is useful for fertility-adjacent OB practices navigating similar bundling rules, as is comparing bundling logic against other GYN surgical codes such as CPT 58558 (surgical hysteroscopy).
When a patient transfers obstetric care mid-pregnancy, document the exact number of antepartum visits furnished by each provider. The receiving provider bills 59514 or 59515 for the delivery components only. The transferring provider bills antepartum-only codes (59425 for 4-6 visits or 59426 for 7+ visits) for the prenatal care furnished before transfer.
Incorrect modifier usage is one of the top triggers for OB claim audits by the Office of Inspector General (OIG). These are the modifiers most commonly applied to CPT Code 59510.
CPT 58611 (tubal ligation performed at the time of cesarean) is typically reported as an add-on code alongside 59510 when the procedure is documented in the operative note. Verify current NCCI edit tables before reporting both codes together, as payer policies on bundling 58611 with global OB codes vary.
Anesthesia for the tubal ligation portion is billed separately under CPT 00851, not bundled into the cesarean delivery anesthesia code.
Pabau's claims management tools help OB-GYN practices track global maternity package components, flag split-care scenarios, and reduce denial rates on complex cesarean delivery claims.

Reimbursement for CPT Code 59510 varies significantly by payer, geographic location, and year. Practices should verify current rates directly through the CMS Physician Fee Schedule lookup tool rather than relying on static published rates.
Medicare rarely applies to obstetric patients given age eligibility criteria, but Medicare Advantage plans and certain dual-eligible populations may encounter this code. Medicaid is the dominant payer for obstetric care in many states.
The New York State Medicaid MOMS (Medicaid Obstetrical and Maternal Services) program, for example, publishes specific procedure code guidance for global OB care that OB-GYN practices in New York must follow. State Medicaid programs can differ substantially in what they bundle or allow separately.
UnitedHealthcare’s commercial reimbursement policy categorizes CPT codes for global OB care into three categories: antepartum-only, delivery-only, and three-component global codes. CPT 59510 falls into the three-component category alongside 59400, 59610 (routine obstetric care including antepartum, vaginal delivery after previous cesarean, and postpartum), and 59618.
BlueCross BlueShield policies generally align with AMA global package definitions but may apply state-specific contract adjustments. Anthem provider guidelines for obstetrical package coding and documentation require that the billing provider furnished all three components before submitting 59510.
Practices comparing billing platforms for OB-GYN-specific reimbursement tracking can review broader options in this guide to the best medical billing software in the US, and a grounding in healthcare revenue cycle management helps contextualize where global OB coding fits into the larger claims lifecycle.
Reviewing coaching CPT codes alongside OB global codes illustrates a broader principle: any multi-visit bundled code requires strong pre-submission documentation of all component services to survive payer review. The same discipline applies to 59510.
Pull your practice’s 59510 claims data for the past 12 months and compare denial reasons. If more than 5% of denials cite ‘global package component not verified,’ your documentation workflow needs a structured visit-count tracking process before billing the global code.
Incomplete documentation is the primary reason 59510 claims are downcoded to 59514 or denied entirely. Payers auditing global OB claims look for three categories of evidence.
Maintain a running count of prenatal visits tied to each patient. Document the date, chief complaint, vital signs, fetal heart tones, and provider of record for each visit. If visits fall below the 13-visit threshold, document the clinical reason (late presentation, premature delivery, transfer of care) so the billing code reflects the actual services furnished.
When a pelvic ultrasound is performed during a prenatal visit, log it separately: CPT 76857 (limited pelvic ultrasound) is billed in addition to the global package when medically indicated and properly documented.
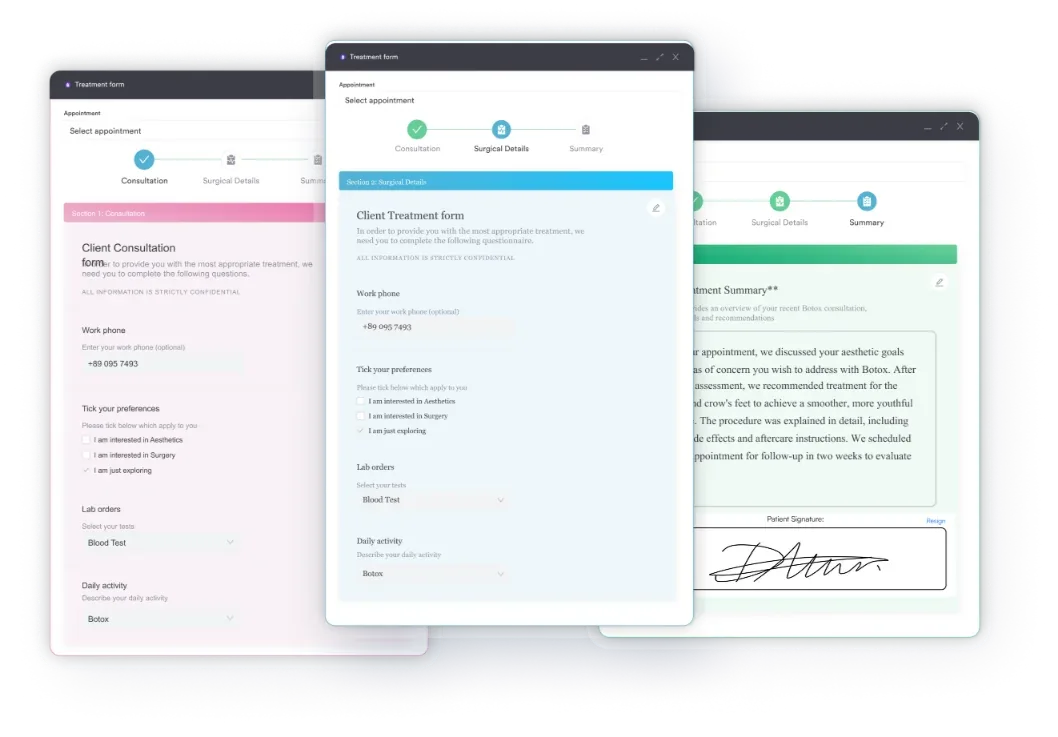
Practices that capture this data in digital intake forms and structured prenatal records reduce the time required to produce documentation on audit request. Good HIPAA-compliant documentation practices also ensure that prenatal visit logs remain retrievable for the standard three-to-seven year payer audit window.
The operative report must identify the primary surgeon, the indication for cesarean, the procedure performed, the anesthesia type, and any additional procedures (such as tubal ligation under CPT 58611). If modifier -22 is applied, the note must explicitly describe the unusual complexity.
Document the postpartum visit date, findings, and the provider who performed it. If postpartum care is transferred to another provider, confirm which modifier applies to split postpartum care billing.
ACOG-aligned postpartum care standards increasingly include screening for postpartum depression at each fourth-trimester touchpoint; if these visits extend beyond the standard six-week window, document their clinical justification for separate billing consideration.
Maintaining a structured medical forms workflow across all three care phases is the most reliable way to produce clean documentation for 59510 claims. Bundling edits and documentation requirements for the 59510-59525 code range are covered in AAPC’s Codify CPT reference tools.
Understanding where practices go wrong with CPT 59510 is as important as knowing the code rules themselves. These are the errors that generate the most rework.
A paperless, HIPAA-compliant practice workflow that ties billing codes to verified clinical documentation before submission catches most of these errors at the source rather than at the denial stage. Consistent HIPAA compliance for medical offices also reduces audit exposure across the practice’s entire OB coding portfolio.
Coders handling OB-GYN claims often field documentation and coding questions that span other specialties in the same practice. Related billing and documentation references include the CPT Code 99347 home visit billing guide, the ICD-10 Code G90.1 coding guide for familial dysautonomia, and the assisted living assessment tool template for practices coordinating care with long-term care facilities.
CPT Code 59510 is one of the most valuable codes in an OB-GYN practice’s billing arsenal, but only when applied correctly. Getting it right means confirming all three global package components were furnished by the billing provider, using modifiers accurately for split-care and surgical assist scenarios, and maintaining a complete documentation trail across antepartum, delivery, and postpartum phases.
CPT 59510 and the global OB codes referenced in this guide are scheduled for deletion on January 1, 2027, under the AMA’s restructured maternity care code set. Claims for 2026 deliveries are unaffected, but 2026 is the year to update documentation and billing workflows ahead of the shift to component-based antepartum E/M coding and the new labor-management and delivery-only codes.
Pabau’s patient record management and claims management tools give OB-GYN practices the infrastructure to track global package components and catch coding errors before submission. To see how Pabau can reduce OB billing denials in your practice, book a demo with the team.
Need OB-GYN-specific practice management tools? Pabau’s OB-GYN EMR software covers scheduling, digital documentation, and claims workflows in one platform.
Want to reduce claim denials across your billing workflow? Pabau’s claims management software helps practices flag common coding errors before submission.
Looking for a structured way to manage prenatal documentation? Pabau’s digital forms support structured antepartum visit records that hold up to payer audit requests.
CPT Code 59510 is a global maternity billing code that covers routine obstetric care including antepartum care, cesarean delivery, and postpartum care when a single provider furnishes all three components of care during the same pregnancy.
CPT 59514 covers cesarean delivery only, with no antepartum or postpartum care included. Use 59514 when the billing provider performed the delivery but did not manage prenatal or postpartum care. Use 59510 only when the same provider furnished all three global package components.
The AMA defines approximately 13 antepartum visits as included in the global package. Visits beyond this threshold, or visits addressing complications outside routine prenatal care, may be separately billable using appropriate E/M codes. Verify exact visit thresholds against your payer contracts, as some insurers follow slightly different standards.
CPT 58611 (tubal ligation at the time of cesarean delivery) is generally reportable alongside CPT 59510 when documented in the operative note. However, verify current NCCI edit tables and your payer’s bundling policy before submitting both codes together, as payer-specific rules vary.
Common ICD-10-CM codes paired with CPT 59510 include O82 (encounter for cesarean delivery without indication) and O34.211 (maternal care for low transverse scar from a previous cesarean delivery) when prior uterine surgery is the delivery indication. O34.21 is a non-billable parent category; O34.211 through O34.219 differentiate by scar type (low transverse, vertical, other, or unspecified), not by trimester. Less commonly, obstetric infection codes such as A34 (obstetrical tetanus) may pair with 59510 when a maternal infection complicates the delivery. The primary diagnosis code should always reflect the clinical reason for the cesarean.
Common modifiers for CPT Code 59510 include modifier -22 (increased complexity), -52 (reduced services), -54 (surgical care only), -55 (postoperative management only), -56 (preoperative management only), and -80 (surgical assistant, billed on the delivery-only code 59514 rather than on 59510 itself). Modifier selection depends on which care components the billing provider furnished and whether an assistant surgeon participated.



