What is concierge medicine? A guide for practice owners
Concierge medicine swaps a 2,000-patient panel for 300-600 on retainer, typicall...
Last Updated: July 31, 2026
Who manages electronic health records depends on role: healthcare providers hold legal custodianship, while health information managers, practice managers, IT staff, and clinicians each carry distinct day-to-day responsibilities.
Legal custodianship (ownership) and operational management are different things. Providers own the record, but multiple staff roles keep it accurate, secure, and accessible.
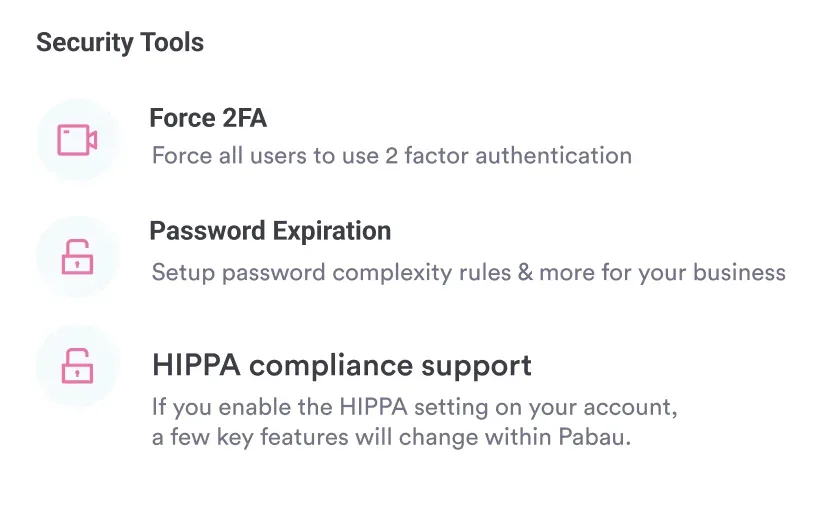
HIPAA requires covered entities to assign a Privacy Officer and implement access controls, audit trails, and data governance policies for EHR systems.
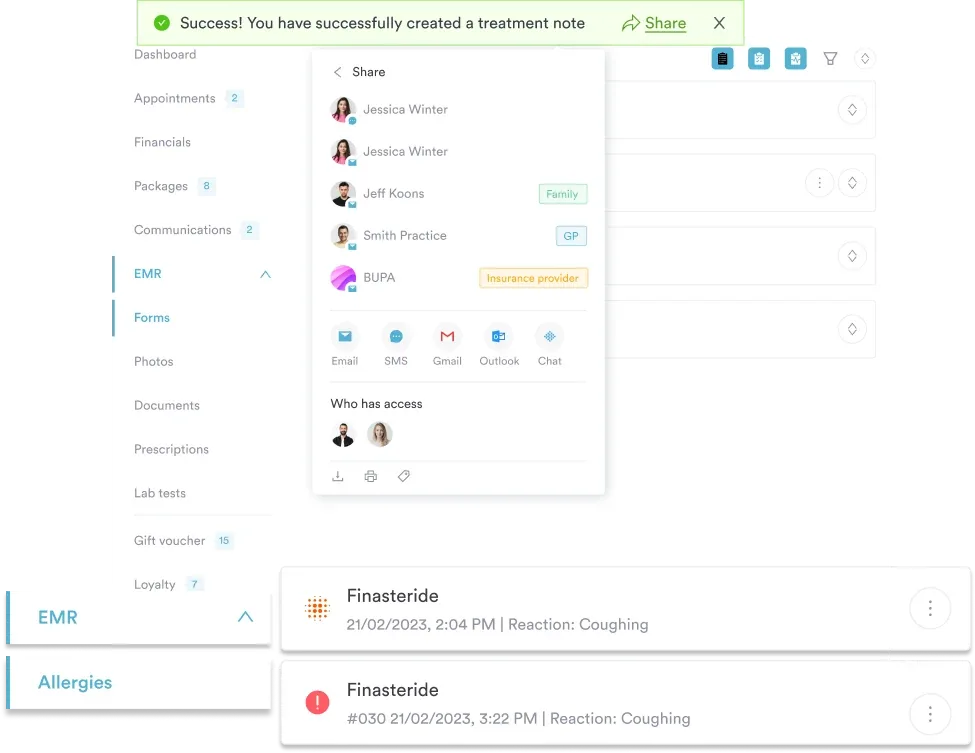
Pabau’s client record tools give private practices role-based access controls, automated audit trails, and digital forms, so every team member manages records within their permitted scope.
Most practices assume their EHR system manages itself once it is set up. It does not. The HHS defines an EHR as a record that can be “created, gathered, managed, and consulted by authorized clinicians and staff.” That word “managed” is doing a lot of work. Who manages electronic health records is not a single answer. It is a layered structure of legal responsibility, operational oversight, and daily clinical input that touches almost every role in a practice.
This guide breaks down each layer: who owns the data legally, who manages it operationally, and who interacts with it day to day. The focus throughout is what that means for private clinics, multi-disciplinary practices, and small healthcare teams.
There is no single person who manages electronic health records across a healthcare organization. Instead, responsibility is distributed across four distinct roles, each with a different scope of authority. Understanding these layers prevents governance breakdowns and costly compliance oversights.
Each role carries different obligations under federal law. Before examining them individually, it helps to distinguish between two concepts that are often conflated: EHR ownership and EHR management. They are not the same thing, and mixing them up creates governance problems.
The question of who owns the patient’s health record has a clear legal answer: ownership sits with the healthcare provider or organization, not the patient and not the software vendor. Once a clinician documents a patient encounter in electronic form, the practice becomes the legal custodian of that information. The patient retains rights to access, amend, and restrict disclosure of their data, but the record itself belongs to the practice.
Operational management is a separate question entirely. Who configures the system, who can view which fields, who corrects documentation errors, and who responds to an audit? These responsibilities are divided among roles that may or may not include the provider. For context on how a practice management system differs from an EMR, the distinction between clinical documentation and administrative oversight becomes even clearer. The same governance questions apply whether your system is technically an EHR or an EMR. The terminology differs, but the responsibility structure doesn’t change.
EHR vendors occupy a specific position here. They process patient data as business associates under HIPAA but do not own it. Business Associate Agreements (BAAs) contractually establish this separation, confirming that the vendor’s role is technical facilitation, not data custody. That distinction matters most when you switch systems. Because the practice owns the data, a vendor cannot hold it hostage, though the export formats and exit terms written into your BAA decide how easily you can actually move it.
When someone asks who is responsible for maintaining electronic health records, the primary answer is the treating clinician or their employing organization. An electronic health record is maintained by the provider over time, not by the patient or the software vendor, and that provider is the party accountable for the record’s existence, accuracy, and security. This is not merely an ethical standard. It is a federal one. CMS guidance on electronic health records frames the provider’s responsibility in terms of both clinical quality and data integrity: the EHR must enable better decisions, and the provider is accountable for the data that drives those decisions.
Under the American Recovery and Reinvestment Act (ARRA), all public and private healthcare providers were required to adopt and demonstrate meaningful use of electronic medical records by January 1, 2014 to maintain Medicare and Medicaid reimbursement levels. This mandate cemented the provider’s legal accountability for EHR adoption and maintenance.
Day to day, what does this legal custodianship look like for a small private practice? It means the practice owner or lead physician is ultimately accountable if a record is inaccurate, improperly shared, or inaccessible when needed. They cannot delegate that ultimate accountability to a software vendor or a practice manager, though they can and should delegate the day-to-day work of client record management to appropriately trained staff supported by the right systems.
Three bodies of regulation shape what providers must do with EHR data in the US. HIPAA’s Privacy Rule governs who can access patient information and under what conditions. The Security Rule mandates technical and administrative safeguards for electronic protected health information (ePHI). The ONC’s information-blocking rules, introduced under the 21st Century Cures Act, require providers to make patient data accessible without delay or restriction.
The Office of the National Coordinator for Health Information Technology (ONC) oversees interoperability standards and certification for EHR systems. A provider using a certified EHR can demonstrate compliance more readily, but certification does not transfer accountability. The provider’s governance obligations remain regardless of which platform they use.
Audit your EHR access logs quarterly. Providers are legally accountable for who views and modifies patient records. A quarterly access review catches privilege creep early (staff retaining permissions they no longer need) and provides documented evidence of active data governance if you face a HIPAA investigation.
Larger healthcare organizations typically employ a dedicated Health Information Manager (HIM) or Health Information Technology specialist. This is the role most people picture as the electronic health records manager, sometimes titled an electronic health record specialist: the person who owns data governance for the record system. In smaller practices, these responsibilities often fall to the practice manager or a senior administrative team member with specialist training.
The HIM role focuses on data governance: ensuring records are complete, accurately coded, and compliant with applicable standards. In coding-heavy environments, this means overseeing ICD-10 and CPT documentation to support accurate reimbursement, often backed by the NHA’s Certified Electronic Health Records Specialist (CEHRS) credential. In compliance terms, it means maintaining the policies and procedures that formally define and enforce who manages electronic health records within the organization.
| Responsibility area | Health information manager | Practice manager |
|---|---|---|
| Data quality audits | Leads and signs off | Supports and implements |
| Access control policies | Defines standards | Configures in system |
| HIPAA Privacy Officer | Often designated | May serve in small practices |
| Staff EHR training | Develops curriculum | Delivers and tracks completion |
| Breach response | Leads investigation | Coordinates notification |
A key HIM responsibility is maintaining the audit trail: the system-generated log of every action taken on a patient record, including who viewed it, who edited it, and when. HIPAA requires covered entities to retain these logs and produce them on request. For HIPAA compliance requirements for clinic software, this audit capability is a non-negotiable technical safeguard, not an optional feature.
The practice manager is typically the operational gatekeeper for EHR management in small to mid-sized practices. They do not write clinical notes, but they control who can. Configuring role-based access, onboarding new staff onto the system, and responding to day-to-day technical issues all sit within their remit.
Access control is the most consequential of these tasks. HIPAA’s minimum necessary standard requires that staff access only the patient information needed for their specific role. A receptionist booking appointments should not have access to clinical consultation notes. A billing coordinator needs invoice data but not medication records. Getting this configuration wrong is one of the most common sources of HIPAA violations in small practices.
IT administrators, whether internal or outsourced, handle the infrastructure layer: server security, backup protocols, software updates, and integration testing. As EHR integration workflows become more complex, with labs, pharmacies, and telehealth platforms all feeding into a central record, the IT role’s scope has grown considerably. In practices without dedicated IT staff, this responsibility defaults to the practice manager, often without the technical training to manage it well.
Strong compliance management tools within the EHR platform reduce the burden on both roles. Automated permission templates, configurable access levels by staff type, and real-time audit dashboards mean the practice manager does not need to manually track every access event.
Pabau gives practice owners, practice managers, and clinical staff role-based access to patient records with automated audit trails, digital consent forms, and HIPAA-aligned data governance built in. No separate compliance tools required.

For most patients, the person who manages their electronic health record in practice is the clinician they see. Physicians, nurse practitioners, nurses, therapists, and allied health professionals are the primary creators and updaters of the clinical record. Their daily actions include creating consultation notes, ordering and documenting tests, updating medication lists, and recording referral outcomes.
This is where the abstract governance framework meets clinical reality. A clinician who documents inaccurately, delays note completion, or fails to flag a record error creates downstream problems for every other role in the system. The practice manager cannot fix what the clinician has not flagged. The HIM cannot audit what was never documented. The legal custodian cannot defend what is incomplete.
Training is critical here. A well-chosen EHR for private practice reduces documentation burden through templates, autofill, and structured data entry, but staff still need to understand what each field means, when to update it, and how to correct errors without overwriting the original entry. The correction protocol matters as much as the documentation itself.
Patients have federally protected rights relating to their EHR data under HIPAA. They can request access to their records, request corrections, and restrict certain disclosures. Clinicians and front desk staff are typically the first point of contact when a patient exercises these rights, which means they need to know the practice’s response protocols.
The American Medical Association (AMA) provides guidance on common EHR myths, including misconceptions about who can amend records and what constitutes a valid correction. Clinical staff who understand these rules protect both their patients and the practice from liability. Ensuring your team follows patient data security protocols is an operational priority, not just a compliance checkbox.
The four-role model above assumes a degree of organizational scale. In a solo practice or a small multi-disciplinary practice, the same person often wears several hats at once. A practice manager might simultaneously serve as the HIPAA Privacy Officer, the de facto IT administrator, and the staff trainer. The lead clinician might handle their own data governance because there is no HIM on staff.
This concentration of responsibility is manageable, but only when the EHR platform is configured to compensate for staffing constraints. Automated audit trails, role-based access defaults, and built-in compliance alerts reduce the manual governance burden considerably. For practices exploring what good EHR governance looks like without a dedicated compliance team, running a paperless, HIPAA-compliant practice covers the practical steps in detail.
Multi-disciplinary practices face a variation of this challenge. When physiotherapists, GPs, and aesthetics practitioners all share a single patient record, role-based access control becomes operationally complex. Each discipline may need to see different fields. Some records may contain sensitive disclosures protected under specific state or federal rules. The question of who manages electronic health records in these environments cannot be answered with a single job title. It requires a documented governance policy that maps each role to specific access permissions.
Document your EHR governance policy before you need it. Write down which staff roles have which access permissions, who holds the HIPAA Privacy Officer designation, and what your correction and breach notification procedures are. A one-page policy document reviewed annually is far easier to defend than an ad hoc response to an HHS complaint.
Regardless of practice size, a few operational habits separate practices with robust EHR governance from those exposed to compliance risk.
Applying strong data protection best practices across all of these areas is not a one-time task. It requires regular review as staff, technology, and regulation evolve.
Keeping client records accurate and current sits at the intersection of clinical quality and legal compliance. A record that is three months out of date is both a clinical risk and a documentation liability.
Managing electronic health records is not a single job. It is a shared system of responsibility that runs from the legal custodian at the top to the clinician entering a consultation note at the bottom. The weak points in that system (unclear role definitions, unconfigured access controls, untrained staff) are where compliance failures and patient safety risks emerge.
Pabau’s patient record platform gives private clinics and multi-disciplinary practices the infrastructure to close those weak points: role-based permissions, automated audit trails, digital consent capture, and HIPAA-aligned data governance built into the core workflow. See how Pabau supports your EHR management responsibilities with a personalized demo.
Want to understand how EHR and practice management tools overlap? Practice management software covers how all-in-one platforms handle scheduling, billing, and clinical records in one place.
Concerned about what a HIPAA audit looks for? HIPAA compliance for medical offices walks through the documentation and technical safeguards auditors check first.
Need to demonstrate data governance to a regulator? GDPR checklist for UK clinics provides a structured framework for documenting your data protection obligations.
An electronic health record (EHR) is a digital file containing a patient’s medical history, diagnoses, medications, treatment plans, test results, and clinical notes, accessible to authorized clinicians and staff across a healthcare organization. Unlike a paper chart, an EHR can be updated in real time and shared across providers, which is why CMS identifies EHRs as a critical tool for improving care quality and reducing medical errors.
The healthcare provider or organization is legally responsible as the custodian of the record. In a private practice, this is typically the practice owner or lead physician. They cannot transfer ultimate legal accountability to software vendors, administrative staff, or health information managers, though operational management is routinely delegated to those roles.
The healthcare provider owns the record as its legal custodian. Patients own their personal health information and have federally protected rights to access, amend, and control disclosure of their data under HIPAA. EHR vendors do not own the data. Their role is technical facilitation, governed by a Business Associate Agreement with the provider.
In the US, HIPAA’s Privacy and Security Rules set the primary standards for EHR management, covering access controls, audit requirements, and breach notification. The ONC’s information-blocking rules under the 21st Century Cures Act require providers to share patient data without restriction. CMS oversees Meaningful Use and interoperability requirements that define how EHR systems must function to qualify for federal reimbursement programs.
An EHR manager, sometimes called an electronic health record specialist, oversees the data governance, quality, and compliance functions of an organization’s electronic record system. Day-to-day tasks include maintaining access control policies, conducting audit trail reviews, managing staff training, ensuring accurate clinical coding, and coordinating the practice’s response to record requests or breach incidents. In small practices, this role is usually absorbed by the practice manager or a senior clinician.