








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT Code 58150 describes a total abdominal hysterectomy (TAH) involving removal of the corpus uteri and cervix, with or without tubes and/or ovaries, via open abdominal incision.
Do not separately report CPT 58700 (salpingectomy) or 58940 (oophorectomy) when performed during the same TAH encounter – NCCI bundling prohibits unbundling these services.
CPT 58150 carries a 90-day global surgical period under Medicare; post-operative visits within that window are included unless a separately identifiable problem arises.
Pabau’s claims management software helps OBGYN practices track modifier usage, manage global period billing, and reduce claim denials on high-value surgical codes like 58150.
CPT code 58150, maintained by the American Medical Association, covers a total abdominal hysterectomy (TAH) — open removal of the corpus uteri and cervix, with or without the fallopian tube(s) and/or ovary(s). It carries a 90-day global period, and salpingectomy (58700) and oophorectomy (58940) are bundled, not billed separately.
It is distinct from laparoscopic codes (58570–58573) and vaginal approach codes (58260–58294), and belongs to the Hysterectomy Procedures range 58150–58294. OBGYN practices billing this code need reliable OBGYN EMR software to capture procedure details, modifiers, and global period events accurately.
The code description’s phrase “with or without removal of tube(s), with or without removal of ovary(s)” means the salpingectomy and oophorectomy components are bundled into 58150 when performed during the same operative session. Reporting CPT 58700 or CPT 58940 separately on the same claim is a NCCI bundling violation, though anesthesia sits outside the surgeon’s bundle entirely and is reported by the anesthesia provider under an abdominal code such as CPT code 00700 (Anesthesia for upper anterior abdominal wall).
Selecting the wrong code in the TAH family is a frequent audit trigger. The table below maps the most commonly confused codes to their key differentiators.
A practical rule: if the operative note documents an abdominal incision and removal of both corpus and cervix, the base code is 58150. If the cervix was spared, use 58180. If the approach was laparoscopic, move to the 58570–58573 range. Dedicated practice scheduling and documentation software that captures approach and specimen details at time-of-service reduces downstream coding errors.
Three modifiers apply most frequently to CPT 58150.
Modifier 22 applies when the TAH involved substantially more work than usual. SGO coding guidance points to 58150-22 for cases like lysis of dense adhesions (with no separate debulking procedure). To get paid, payers usually want an operative note that spells out the extra time and the specific factors that made the case harder.
Common qualifying scenarios include: dense pelvic adhesions from prior surgeries or endometriosis, a significantly enlarged or fibroid uterus that substantially increases operative time, and unusual anatomical distortion requiring extended dissection. When adhesiolysis is instead performed as a stand-alone laparoscopic procedure, it maps to laparoscopic lysis of adhesions (58660), not 58150-22.
Most payers require a cover letter with the claim explaining the basis for Modifier 22; expect some to request the full operative note before adjusting reimbursement upward.
Use Modifier 52 when the planned TAH was intentionally reduced in scope at the surgeon’s discretion before the procedure was fully completed. This differs from a complication that stopped the case; it reflects an elective decision to perform less than the full service described by the code.
Modifier 59 is used when a second procedure performed on the same date is distinct from the TAH and would otherwise be bundled incorrectly by the payer’s editing system.
Apply it carefully: CMS expects documentation showing the procedure was performed on a different anatomical site or represented a separate patient encounter. Using 59 to override a legitimate NCCI edit is a compliance risk.
Document the modifier rationale in the operative note before the claim is submitted, not after a denial. Payers increasingly request supporting documentation at initial submission for Modifier 22 on high-value surgical codes. A one-paragraph operative summary explaining the complicating factors saves weeks of appeals work.
The CMS National Correct Coding Initiative (NCCI) explicitly prohibits unbundling the components of a total abdominal hysterectomy. Understanding which codes cannot be reported alongside CPT 58150 prevents the most common denial reasons for this procedure.
Billing CPT 58150 and CPT 58140 together on the same date requires careful review against current NCCI edits before submission. The clinical rationale would need to be clearly documented if a myomectomy and a total hysterectomy were separate procedures on distinct anatomical targets.
Verify the current NCCI edit table for this pair before submitting, as edit status can change with quarterly updates. Tracking accurate procedure pairing is one area where purpose-built claims management software adds measurable value.
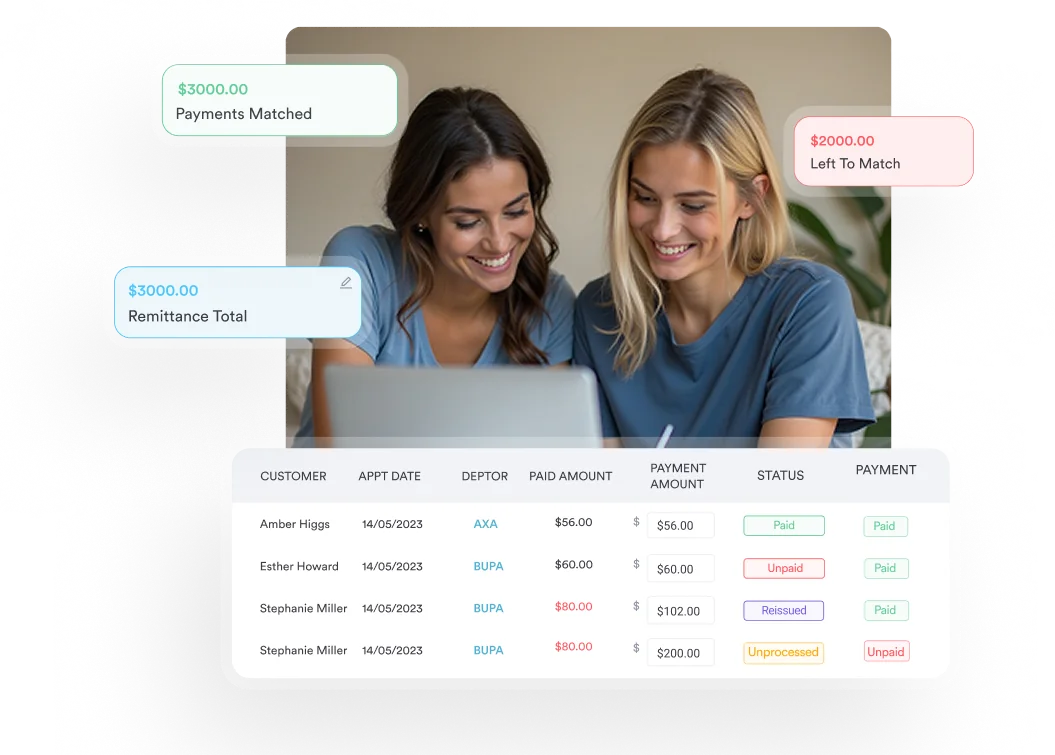
Pabau's claims management tools help OBGYN practices track modifier usage, flag NCCI bundling conflicts, and manage global period billing – so fewer 58150 claims come back as denials.

Medicare reimbursement for CPT 58150 is calculated using Relative Value Units (RVUs) from the CMS Physician Fee Schedule. The total payment reflects work RVUs, practice expense RVUs, and malpractice RVUs, each adjusted by the geographic practice cost index (GPCI) for the practice location.
Commercial payer rates for 58150 vary significantly by contract. Some payers use a percentage of the Medicare fee schedule (often 110-150%), while others negotiate flat rates per procedure. Always verify your contract terms for major surgical codes rather than assuming Medicare-equivalent rates apply.
CPT Code 58150 carries a 90-day global surgical period under the Medicare Physician Fee Schedule. This means the surgeon’s fee bundles all routine post-operative care from the day before surgery through 90 days after the procedure.
Tracking which visits fall inside the 90-day window — and whether each qualifies for separate billing — requires consistent documentation at the point of care. Surgical scheduling workflows that flag active global periods for returning patients reduce over-billing risk. HIPAA-compliant records for every post-operative encounter support audit defense if payers question global period billing decisions.
Thorough operative documentation is the most effective denial-prevention strategy for 58150 claims. Payers auditing this code look for specific elements that confirm medical necessity, support the approach chosen, and justify any modifiers appended.
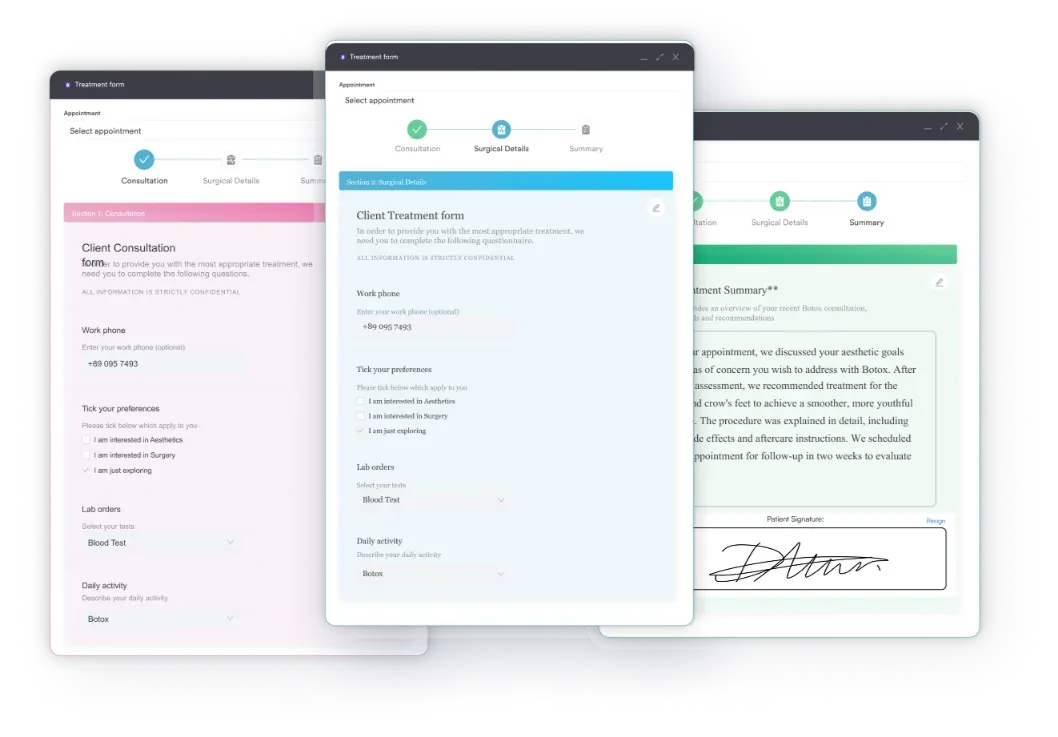
Standardized surgical documentation forms reduce the risk of omitting these elements. Digital intake forms and procedure templates — for example, a pelvic exam documentation template — that prompt for approach, structures removed, and complexity factors help ensure nothing is missed before the claim is submitted.
Every operative record must be stored securely with audit-ready access controls per HIPAA requirements. For practices also handling oncologic pelvic procedures requiring implantable materials, the HCPCS Code C1781 implantable mesh billing guide is a useful companion reference.
Medical necessity for a TAH is established by the linked ICD-10-CM diagnosis code. The primary diagnosis must justify the procedure under the payer’s coverage policy, and supporting workups such as a pelvic ultrasound help document that necessity. Common pairings include:
Always assign the most specific ICD-10-CM code available. Unspecified codes (e.g., N93.9) draw scrutiny and may trigger medical necessity review. Cross-reference the selected diagnosis against the payer’s applicable Local Coverage Determination (LCD) or National Coverage Determination (NCD) before submitting.
Run a pre-claim audit on every 58150 submission: verify the ICD-10 code supports medical necessity under the payer’s coverage policy, confirm no separately-prohibited companion codes (58700, 58940, 58146) are on the claim, and check that any Modifier 22 is supported by operative note language before the file leaves the practice.
Understanding the full hysterectomy code family helps coders select the right code and cross-reference adjacent procedures. Practices that also bill for fertility-related services may find the IVF CPT codes reference useful alongside gynecologic surgical codes. Standardizing how these codes are captured in a gynecology EHR reduces selection errors across the family.
For practices managing gynecologic oncology billing alongside general OBGYN, standardized surgical documentation forms that capture procedure type, approach, and specimen weight at time-of-service prevent the most common code-selection errors in this family.
Denials on CPT code 58150 are almost always preventable. When complex reconstructive procedures accompany oncologic resection, the CCSD Code T7602 microvascular free tissue transfer billing guide and the CPT Code 50825 continent diversion billing guide provide additional coding context for multi-procedure surgical claims.
The most common causes are NCCI bundling violations (separately billing 58700 or 58940), missing Modifier 22 documentation, and ICD-10 codes that do not establish medical necessity with the payer. Catching these before submission rather than resolving them on appeal saves significant time and revenue.
Pabau’s automated billing workflows help OBGYN practices flag modifier requirements, track global period windows, and maintain audit-ready documentation for high-value surgical codes. Book a demo to see how Pabau handles surgical billing for OBGYN practices.
Want to catch missing documentation before claims go out? Digital forms covers how Pabau’s customizable procedure templates prompt for operative details that support correct code selection and modifier use.
Continue your research: browse our latest coding guides, including critical care CPT code 99291 and CPT 97804 for medical nutrition therapy.
CPT Code 58150 is a total abdominal hysterectomy (TAH) involving removal of the corpus uteri and cervix through an open abdominal incision, with or without removal of the fallopian tubes and/or ovaries. The salpingectomy and oophorectomy components are bundled into 58150 when performed during the same surgical session and cannot be reported separately.
CPT 58152 describes a total abdominal hysterectomy combined with a colpo-urethrocystopexy (bladder neck suspension such as Marshall-Marchetti-Krantz or Burch procedure). Use 58152 only when the operative note documents both the TAH and a concurrent bladder neck suspension; 58150 is used for a standard TAH without the urethrocystopexy component.
Modifier 22 applies when the procedure required substantially more work than usual, such as lysis of dense adhesions. Modifier 52 is used for a reduced-scope procedure completed at the surgeon’s discretion. Modifier 59 identifies a distinct procedural service when a second procedure on the same date would otherwise be incorrectly bundled. All three require supporting documentation in the operative note.
Yes. CMS NCCI policy explicitly prohibits separately reporting CPT 58700 (salpingectomy) or CPT 58940 (oophorectomy) when these procedures are performed during the same TAH encounter. Doing so constitutes unbundling and will result in claim denial or recoupment on audit.
CPT Code 58150 has a 90-day global surgical period under Medicare. The surgeon’s payment includes all routine post-operative care from the day before surgery through 90 days after the procedure. Visits for unrelated conditions during this period can be billed separately with Modifier 24; return-to-OR complications use Modifier 78.
Common ICD-10-CM codes paired with CPT 58150 include D25.9 (uterine leiomyoma), N92.0 (heavy menstrual bleeding), N80.0/N80.1 (endometriosis), C54.1 (endometrial carcinoma), and N81.2/N81.3 (uterovaginal prolapse). The selected diagnosis must meet the applicable payer’s medical necessity criteria and should be as specific as possible to avoid unnecessary review.



