HCPCS Code A7033: Nasal pillow replacement billing guide 2026
A7033 bills replacement nasal pillows per pair, not per pillow. Medicare allows ...
Last Updated: August 6, 2026
HCPCS code B4152 describes enteral formula that is nutritionally complete, calorically dense (equal to or greater than 1.5 kcal/mL) with intact nutrients, billed 100 calories = 1 unit
Medicare covers B4152 under the Prosthetic Device benefit (Social Security Act §1861(s)(8)), not the DME benefit, when a physician order and Certificate of Medical Necessity (CMN) confirm functional impairment preventing adequate oral intake. Claims are still processed through the DME MAC for the supplier’s jurisdiction
Every code in the B4149-B4155 enteral formula series bills in 100-calorie units, not per mL or per container, and mixing up B4152 (calorically dense) with B4149 (blenderized natural foods) is the most common code-selection error
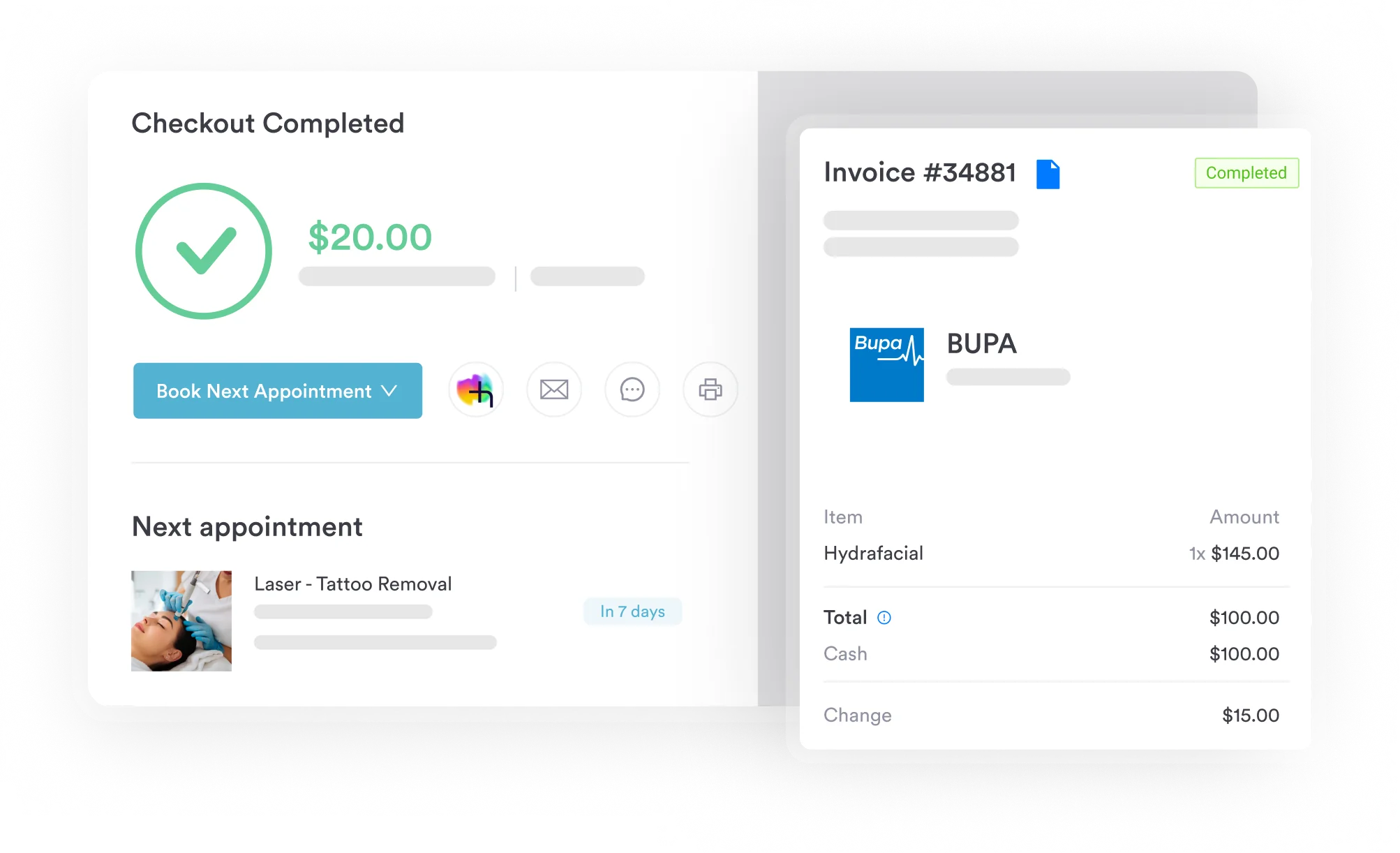
Practice management software like Pabau supports HCPCS code lookup, CMN tracking, and prior authorization workflows to reduce B4152 claim denials
HCPCS code B4152 describes enteral formula that is nutritionally complete and calorically dense (equal to or greater than 1.5 kcal/mL), billed 100 calories = 1 unit. Medicare covers it under the Prosthetic Device benefit, not the DME benefit. Even so, the DME MACs – CGS and Noridian – still process the claims.
HCPCS code B4152 is a Level II HCPCS code officially described as “enteral formula, nutritionally complete, calorically dense (equal to or greater than 1.5 kcal/mL) with intact nutrients, includes proteins, fats, carbohydrates, vitamins and minerals, may include fiber, administered through an enteral feeding tube, 100 calories = 1 unit.” The code sits within the B-code series maintained by CMS’s HCPCS coding system.
Clinicians reach for it when a patient needs tube feeding with a formula that packs more calories into a smaller fluid volume than a standard 1 kcal/mL product.
In practice, B4152 suits patients who cannot take enough nutrition by mouth because of a functional impairment, such as dysphagia after a stroke, head and neck cancer, or a severe neurological condition. Often, these patients also need fluid restriction, for conditions like congestive heart failure or chronic kidney disease, where standard-volume tube feeding would deliver too much fluid.
Calorically dense formulas differ from standard polymeric formulas (B4150) and from blenderized natural foods formulas (B4149) because they concentrate calories rather than change the ingredient source. Specifically, CMS Policy Article A58833 governs coverage and confirms that this formula type is a covered Prosthetic Device benefit once the provider establishes medical necessity.
The table below provides a quick-reference summary of the key billing attributes for HCPCS code B4152.
Medicare covers enteral nutrition under the Prosthetic Device benefit when a patient cannot meet nutritional needs through oral feeding, because of a permanent or long-term functional impairment of the gastrointestinal tract or a condition that blocks adequate absorption. This is the same benefit category as ostomy and tracheostomy supplies, since enteral feeding replaces the function of a permanently impaired digestive tract.
You still submit claims to the DME MAC for your jurisdiction, which then processes them. However, coverage for HCPCS code B4152 requires meeting all of the following criteria, per CMS Policy Article A58833.
Medicare Advantage plans follow CMS enteral nutrition coverage guidelines as a baseline, but many add extra prior authorization rules. So always verify plan-specific policies before you submit claims. Good HIPAA compliance practices also matter here: you need to keep the patient records behind each claim secure and ready to produce during an audit.
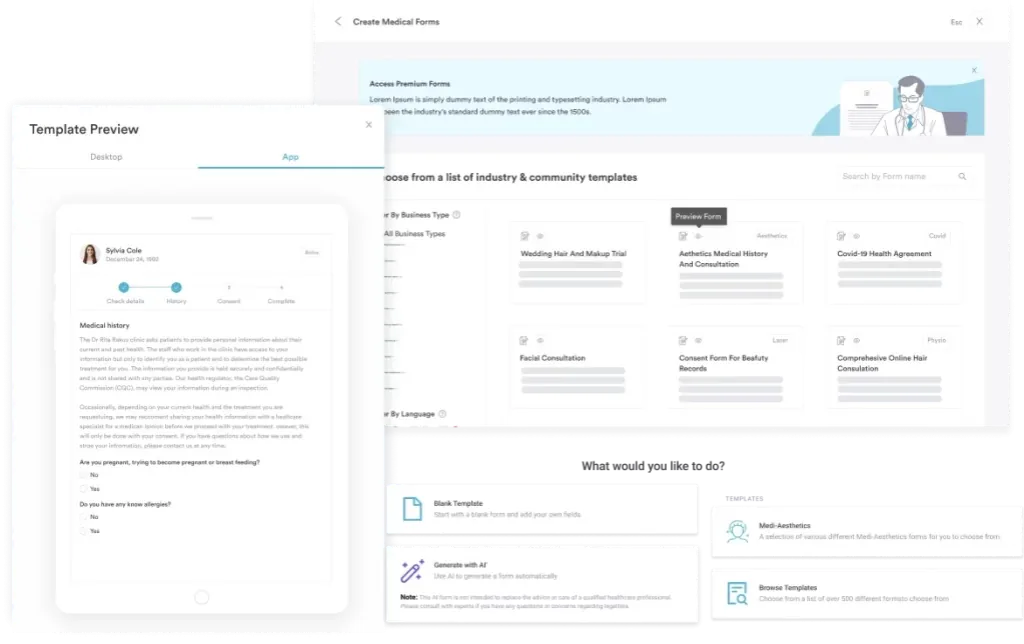
Missing or incomplete paperwork is the leading cause of B4152 claim denial, so every claim needs a complete documentation package. Digital forms software can standardize how you collect and store these documents in the patient record, which lowers the risk that a missing element triggers a denial.
Strong patient data security tools matter when you store CMN documents and delivery confirmations electronically, especially for DME suppliers handling large volumes of enteral nutrition claims. On demand, you must be able to produce these records for a post-payment audit.
Flag CMN expiry dates in your billing workflow. The most common audit finding for enteral nutrition claims is a lapsed or missing CMN recertification. Set a 60-day advance reminder to initiate recertification before the current CMN expires.
You bill HCPCS code B4152, like every code in the B4149-B4155 series, per 100 calories – not per mL and not per can or bottle. So one unit equals 100 calories of formula delivered, regardless of the formula’s volume. In fact, billing per mL or per container ranks among the most frequent unit-calculation errors that DME MACs flag in enteral nutrition correct-coding guidance.
Worked example: A patient’s physician order prescribes a calorically dense formula at 2,100 calories per day for a 30-day supply.
Because B4152 formulas are concentrated, the same daily calorie order needs less fluid volume than a standard formula – yet the billing unit count is identical either way, since units track calories, not mL. So never convert container size or fluid volume into billing units – always work from the prescribed daily calorie total.
Enteral nutrition claims must include an ICD-10-CM diagnosis code that supports the medical necessity of tube feeding. B4152 claims often also need a code that supports the fluid-restriction rationale for a calorically dense formula.
The table below lists commonly accepted supporting codes per the guidance in CMS Policy Article A58833. Verify the current CMS-published list annually, since codes are updated each fiscal year.
Primary care physicians who order home enteral nutrition for stroke, dysphagia, or chronic kidney disease patients are often the ones documenting this necessity. That’s why primary care practice software needs to surface the right diagnosis codes at the point of ordering.
These codes are examples of supporting diagnoses; the complete list of accepted ICD-10-CM codes is published by CMS and updated each October. Always cross-reference the active policy article for the most current list before submitting claims.
Medicare sets HCPCS code B4152 reimbursement through the CMS Physician Fee Schedule and DME fee schedule, updated each January 1. Rates are not uniform nationally.
Each DME MAC jurisdiction sets allowable amounts based on CMS methodology, so a claim submitted to CGS Medicare (Jurisdictions B and C) may receive a different payment than the same claim submitted to Noridian (Jurisdictions A and D).
As a general orientation, B4152 is billed in 100-calorie units (see the worked example above). A typical daily calorie order for a calorically dense formula might run 1,500-2,500 calories per day, meaning roughly 15-25 billing units per day. Monthly claim totals therefore reflect the prescribed calorie load, not the fluid volume delivered.
So always verify rates directly through your MAC’s published fee schedule before you build reimbursement projections. CMS updates both the national average and the MAC-specific allowables with each annual fee schedule release. Using claims management software with current fee schedule data lowers the risk of under-coding or writing off wrongly denied amounts.
Correct modifier use is critical for HCPCS code B4152 billing. A wrong or missing modifier is one of the fastest routes to a claim denial or a post-payment audit flag. The table below covers the modifiers most relevant to enteral nutrition B-code claims. Also, verify current modifier guidance with your specific MAC bulletin, since modifier rules can vary by jurisdiction.
Selecting the wrong enteral formula code is one of the most common claim errors in this category. B4152 is one of six currently billable codes in the B4149-B4155 series, each covering a distinct formula type and nutritional profile, all billed in 100-calorie units.
The crosswalk below helps billers and DME suppliers identify which code matches the ordered formula. The same detailed-descriptor approach applies to other single-purpose DME supply codes, such as A4356 and A4520. Check the AAPC’s HCPCS code lookup for full current descriptors.
The most common code confusion is between B4149 and B4152 – not because their descriptors overlap, but because billers frequently miscode both when they work from memory rather than from the physician order. B4149 is only for manufactured blenderized natural foods formulas, whereas B4152 is only for calorically dense (≥1.5 kcal/mL) formulas.
So if the physician order specifies a real-food blenderized product, B4149 is correct. If instead it specifies a concentrated-calorie formula for a fluid-restricted patient, B4152 applies. Note, too, that CMS deleted B4151 from HCPCS effective January 1, 2005, so it should never appear on a current claim.
Most HCPCS code B4152 claims come from the home setting under Medicare’s Prosthetic Device benefit, processed through the DME MAC system. Typically, DME suppliers – rather than hospitals or practices – bill these claims.
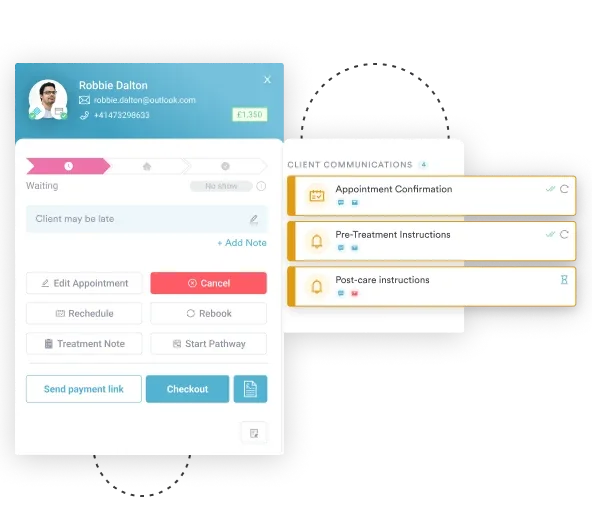
Because understanding the home billing workflow reduces the rate of avoidable denials, it pays to get the steps right. Automated billing workflows are especially useful for DME suppliers managing recurring monthly enteral nutrition claims across a large patient panel.
Pabau's claims management tools help DME suppliers and practice billing teams track HCPCS code B4152 documentation, manage CMN renewal dates, and automate prior authorization workflows.

Medicare fee-for-service does not generally require prior authorization for enteral nutrition under traditional Part B. However, Medicaid programs and Medicare Advantage plans frequently do. Time-saving features in high-volume DME billing operations often center on automating prior authorization tracking and renewal alerts.
Enteral nutrition billing under HCPCS code B4152 carries a higher-than-average denial rate across several MACs, largely because of its documentation-heavy requirements. The table below maps the most common denial reasons to their root causes and corrective actions. In addition, tracking denial patterns as part of broader revenue cycle management helps you spot systemic errors before they compound.
Standalone reference tools like AAPC and PayerPrice describe the code, but coders still have to copy the number into the billing system by hand. That manual transfer step is where B4149/B4152 mix-ups and missing modifiers most often creep in.
By contrast, embedding HCPCS code lookup directly inside the billing workflow, rather than treating it as a separate step, removes that transfer entirely and cuts the error rate at the code-selection stage.
Pabau’s claims management software embeds HCPCS code lookup within the active claim workflow so coders select from validated codes rather than re-entering them from memory. For enteral nutrition claims specifically, three workflow areas matter most.
Finally, practices and DME suppliers already handling compliance management across multiple payer contracts find that centralizing enteral nutrition records inside the practice management system reduces audit exposure – far more than storing CMNs and delivery records in separate folders or spreadsheets.
That documentation trail matters just as much for a nutrition-focused functional medicine practice as it does for a DME supplier, since both depend on the same CMN and physician-order paperwork.
The patient care management documentation trail becomes an automatic by-product of the normal billing workflow rather than a separate manual step.
Audit your B4152 claims quarterly. Pull all claims billed in the prior quarter, check that each has a current CMN, a signed proof of delivery, the correct 100-calorie unit count, and the KX modifier where applicable. Catching a documentation or unit-calculation error before submission, rather than after denial, saves significant rework time and protects against retrospective audits.
HCPCS code B4152 is a narrowly defined code for a specific clinical product: a nutritionally complete, calorically dense enteral formula (≥1.5 kcal/mL), billed 100 calories = 1 unit and covered under Medicare’s Prosthetic Device benefit.
Getting it right requires matching the physician’s order precisely to the correct B-code, rather than confusing it with B4149’s blenderized natural foods formula. It also means calculating units from calories rather than volume, maintaining a complete documentation package, and applying modifiers accurately for each payer’s requirements.
Pabau’s claims management tools integrate HCPCS code workflow directly into patient records and billing, closing the documentation shortfalls that drive most B4152 denials. To see how Pabau handles enteral nutrition billing workflows, book a demo.
Need to understand HCPCS billing more broadly? Bupa CCSD codes guide covers the UK private healthcare procedure code structure and billing rules in detail.
Billing a related infusion drug code? J1459 covers Privigen IVIg billing, processed through the same DME MAC system as enteral nutrition claims.
Need a documentation checklist for another DME supply code? A4322 carries the same physician-order and medical-necessity requirements DME suppliers already know from B4152.
HCPCS code B4152 is an enteral formula, nutritionally complete, calorically dense (equal to or greater than 1.5 kcal/mL) with intact nutrients, billed 100 calories = 1 unit. It covers the supply of concentrated-calorie tube feeding formulas for patients who cannot take adequate nutrition orally due to a functional impairment and who also need fluid restriction, administered via nasogastric, gastrostomy, or jejunostomy tube under Medicare’s Prosthetic Device benefit.
Medicare reimbursement for HCPCS code B4152 varies by DME MAC jurisdiction and is updated annually each January 1 via the CMS DME fee schedule. There is no single national rate. Verify current allowable amounts directly through your MAC’s published fee schedule or the CMS fee schedule search tool before building reimbursement projections.
Billing HCPCS code B4152 requires a detailed written physician order specifying the formula type, caloric density, and administration route, a completed Certificate of Medical Necessity (CMN) signed by the treating physician, ICD-10-CM diagnosis codes supporting medical necessity, and signed proof of delivery for each supply episode. Ongoing claims also require CMN recertification at MAC-specified intervals, typically every 12 months.
B4149 and B4152 are both enteral formulas billed 100 calories = 1 unit, but they describe entirely different products. B4149 covers manufactured blenderized natural foods formulas. B4152 covers calorically dense formulas (equal to or greater than 1.5 kcal/mL), used when a patient needs more calories in less fluid volume, such as patients with heart failure or chronic kidney disease. If the physician order specifies a real-food blenderized product, use B4149; if it specifies a concentrated-calorie formula for fluid restriction, use B4152. Mixing up these two codes is one of the most common formula-code errors in this code series.
Medicare Part B fee-for-service does not generally require prior authorization for B4152, though the KX modifier must confirm documentation is on file. Medicaid programs vary significantly by state and many require prior authorization for extended enteral nutrition. Medicare Advantage plans typically require prior authorization before initiating home enteral nutrition, with renewal periods of 6 to 12 months.
HCPCS code B4152 is covered under Medicare’s Prosthetic Device benefit (Social Security Act §1861(s)(8)), not the DME benefit, because enteral nutrition replaces the function of a permanently impaired digestive tract. Claims are still submitted to, and processed by, the DME MAC for your jurisdiction (for example, CGS or Noridian), so the supplier enrollment and claim-routing rules for DME suppliers still apply even though the benefit category itself is Prosthetic Device.