HCPCS Code A7033: Nasal pillow replacement billing guide 2026
A7033 bills replacement nasal pillows per pair, not per pillow. Medicare allows ...
Last Updated: August 6, 2026
HCPCS code J1459 covers injection of immune globulin Privigen, intravenous, non-lyophilized, billed per 500 mg administered
Units are calculated by dividing total grams administered by 0.5 – incorrect unit calculation is the leading cause of J1459 claim denials
Covered indications include primary immunodeficiency (D80-D84 range), ITP (D69.3), and CIDP (G61.81); ITP and CIDP coverage is set by each Medicare Administrative Contractor’s own local coverage determination, not one national policy, and off-label uses are not covered under Medicare Part B
Pabau’s claims management software helps infusion practices automate unit tracking, store NDC data, and manage prior authorization workflows
Most J1459 claim denials don’t come from the wrong diagnosis. They come from a unit calculation error that went unnoticed until the remittance arrived. Privigen is billed per 500 mg, and a single rounding mistake on a 30-gram infusion produces 4 extra units – enough to trigger an overpayment flag or a full denial.
HCPCS code J1459 has a narrow set of covered indications, strict documentation requirements, and mandatory NDC reporting that varies by vial size. This guide covers everything billing staff and practice managers need to submit clean J1459 claims, from dosage calculation to prior authorization.
IV therapy practices and wellness clinics billing Privigen use HCPCS code J1459 to report each infusion. J1459 is a HCPCS Level II code maintained by the Centers for Medicare and Medicaid Services (CMS) for outpatient drug claims under Medicare Part B and most commercial payers.
Privigen is a 10% liquid intravenous immunoglobulin (IVIg) product. It does not require reconstitution before infusion, which distinguishes it from lyophilized (freeze-dried) formulations billed under different J codes. CMS classifies J1459 as a separately payable outpatient drug under Medicare Part B.
J1459 billing units follow a straightforward formula, but precision matters. One unit of J1459 equals 500 mg of Privigen administered. To calculate units, divide the total dose administered (in grams) by 0.5.
Always base units on the actual dose administered, not the dose ordered. If a patient received 28 g due to an infusion rate adjustment mid-session, bill 56 units, not 60. Document the administered quantity in the infusion record before submitting the claim.
Verify units against the pharmacy dispensing record and the nursing infusion log before claim submission. A discrepancy between the two is a red flag that will invite auditor scrutiny. Bill what was administered, not what was dispensed.
Medicare Part B covers J1459 only when supported by an FDA-approved indication and a covered ICD-10-CM diagnosis code under the local coverage determination (LCD) published by your Medicare Administrative Contractor (MAC).
There is no single national LCD for IVIg – coverage policy is set locally, and the specific LCD number depends on which MAC processes your claims (for example, First Coast Service Options publishes L29205 for Jurisdiction N: Florida, Puerto Rico, and the US Virgin Islands, while Novitas Solutions publishes L34314 and L34074 for Jurisdictions H and L).
Understanding who can administer IV therapy and for which indications is the foundation of clean claim submission. Privigen carries three FDA-approved indications: Primary immunodeficiency (PI), chronic immune thrombocytopenic purpura (ITP), and chronic inflammatory demyelinating polyneuropathy (CIDP).
Coverage is limited to Privigen’s three FDA-approved indications – PI, ITP, and CIDP. Multiple sclerosis (G35), Guillain-Barré syndrome (G61.0), and other neurological or hematologic diagnoses are not FDA-approved indications for Privigen and are not reimbursable under Medicare Part B; treat any request to bill IVIg against these diagnoses as off-label and confirm coverage directly with the payer before proceeding.
Primary immunodeficiency has the broadest coverage basis of the three. National coverage of the IVIg drug itself for home infusion in PI traces to the Medicare Modernization Act of 2003, effective January 1, 2004 (CMS Pub. 100-02, Chapter 15, §50.6).
National coverage of the associated home-infusion supplies, equipment, and nursing for PI came later, under the Consolidated Appropriations Act of 2023, effective January 1, 2024.
ITP and CIDP don’t have a national coverage determination – coverage for these indications is set by each MAC’s own local coverage determination (LCD), so always verify the current covered-code list against the LCD that applies to your MAC jurisdiction before submitting a claim. Examples of active IVIg LCDs by jurisdiction:
This list is illustrative, not exhaustive – every MAC publishes its own LCD, and the covered-diagnosis list, documentation requirements, and review triggers differ between them. Confirm the LCD number and current covered indications with the MAC that processes your claims before billing, rather than assuming one LCD number applies nationally.
Medicare Part B covers HCPCS code J1459 as a separately payable outpatient drug when medical necessity is established. Reimbursement follows the Average Sales Price (ASP) plus 6% methodology.
Because ASP is recalculated quarterly by CMS, specific dollar amounts change four times per year. Consult the CMS Physician Fee Schedule lookup tool for current payment rates before estimating patient cost-sharing or modeling reimbursement projections.
Key coverage requirements under Medicare Part B include:
Practices should first confirm which MAC processes their Part B claims, then review that MAC’s specific IVIg LCD – for example, Novitas Solutions publishes L34314 and L34074 for Jurisdictions H and L, while First Coast Service Options publishes L29205 for Jurisdiction N.
Covered diagnoses and documentation requirements can differ between MAC policies, so don’t assume a policy written for one jurisdiction applies to your own.
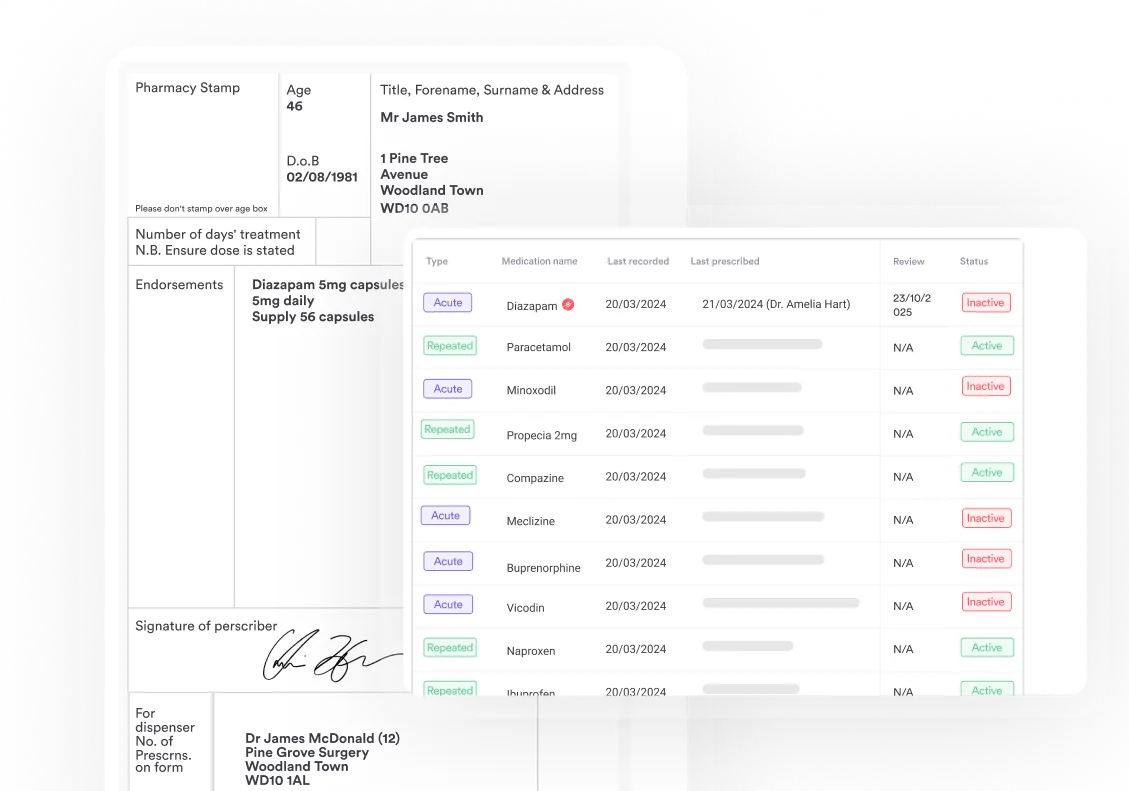
NDC (National Drug Code) reporting is mandatory on all Medicare Part B claims for HCPCS code J1459. Submitting a claim without a valid NDC results in an automatic rejection. Using prescription management software that stores current NDC data by vial size eliminates one of the most avoidable denial causes in infusion billing.
Privigen is available in multiple vial sizes, each with a distinct NDC number. The NDC format required for Medicare Part B claims is the 11-digit format (5-4-2 structure). Supply codes such as HCPCS code A4209 for syringes don’t carry the same requirement, since NDC reporting applies to drug codes, not supplies. Key NDC reporting rules:
Confirm current NDC values before each billing cycle. Outdated NDCs are a common cause of Part B drug claim rejections.
J1459 covers the drug product only. The infusion administration is billed separately using therapeutic infusion CPT codes. These two billing lines are always submitted together for an outpatient IVIg session. The AAPC HCPCS code reference provides additional guidance on pairing drug codes with administration codes.
96365 is the base administration code for most standalone Privigen infusions. 96366 is added for each complete additional hour. A 3-hour IVIg infusion would bill 96365 once and 96366 twice. Never bill 96365 more than once per drug per session.
A handful of modifiers apply to J1459 claims, most related to reporting discarded drug from single-use Privigen vials and confirming that LCD requirements are met. Missing or incorrect modifiers are a common cause of otherwise clean claims getting kicked back for review.
JW and JZ reporting has been mandatory since CMS’s 2023 discarded-drug policy took effect for single-dose container drugs, including Privigen – every J1459 claim line needs one or the other. The same requirement applies to other single-dose injectables, including HCPCS code J3301 and HCPCS code J0702. KX requirements vary by MAC, so confirm the specific instruction in the LCD that applies to your jurisdiction rather than assuming it’s required everywhere.
J1459 is specific to Privigen. Other IVIg products manufactured by different companies carry their own HCPCS codes. Using the wrong code for the administered product is a billing error that invites audit. If your practice administers more than one IVIg brand, confirm the correct J code against the dispensed product’s NDC before claim submission.
Verify each code’s active status annually. CMS publishes HCPCS Level II updates each January, and product-specific codes can be added, revised, or deleted with each cycle. Use the PGM HCPCS lookup tool to confirm the current descriptor and status of any J code before billing.
Prior authorization (PA) requirements for HCPCS code J1459 vary significantly by payer. Understanding these upfront prevents claim denials that take weeks to resolve. For practices managing mobile IV therapy operations or multi-site infusion programs, tracking PA status per patient per payer is especially critical.
Medicare Part B: Prior authorization is not universally required under traditional Medicare for J1459, but some MACs may require prior authorization for certain high-cost IVIg claims or in cases involving specific indications. Verify with the applicable MAC before assuming PA is not needed.
Commercial payers: Most commercial plans require prior authorization for IVIg. Documentation typically required for PA approval includes:
PA requirements differ by plan and are updated frequently. Verify with each commercial payer before every new authorization period. Further context on IV hydration business requirements by state also affects PA workflows in some jurisdictions.
Inadequate documentation is the second most common reason J1459 claims fail post-payment audit, behind unit calculation errors. Every claim must be supportable by the medical record at the time of submission, not reconstructed after an audit request. Good IV therapy documentation practices align the clinical record to billing requirements from the first patient visit.
Required documentation per your MAC’s active LCD for IVIg typically includes:
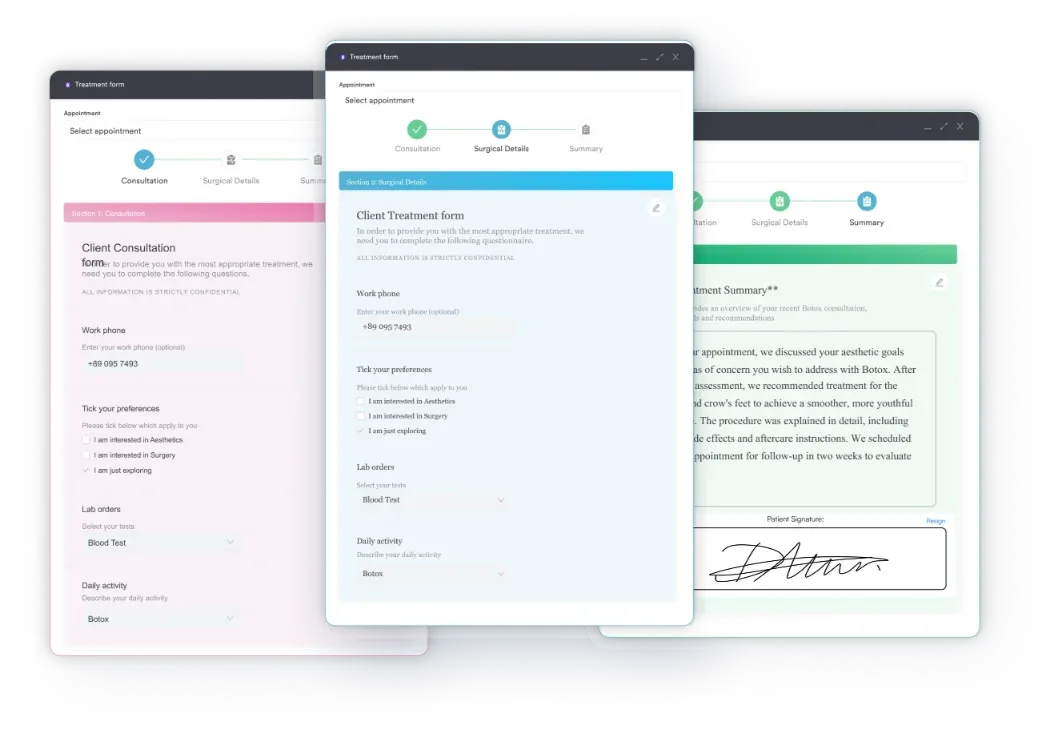
A well-structured IV therapy intake form captures the clinical baseline at intake and feeds the documentation chain required for ongoing J1459 claims. Store completed infusion records in the patient chart and link them to the billing encounter before claim submission. Using digital intake forms that feed directly into the patient record removes the transcription step that often introduces errors.
J1459 has a short list of recurring denial patterns. Most are preventable with a pre-submission checklist built into the billing workflow. Understanding common errors is where IV therapy practice management discipline pays the biggest dividends.
Billing HCPCS code J1459 involves multiple moving parts: Unit calculation, NDC capture, PA status tracking, diagnosis code validation, and documentation completeness. Any one of these can produce a denial when handled manually. IV therapy EMR software that integrates clinical documentation with billing reduces the handoff risk between the infusion nurse and the billing team.
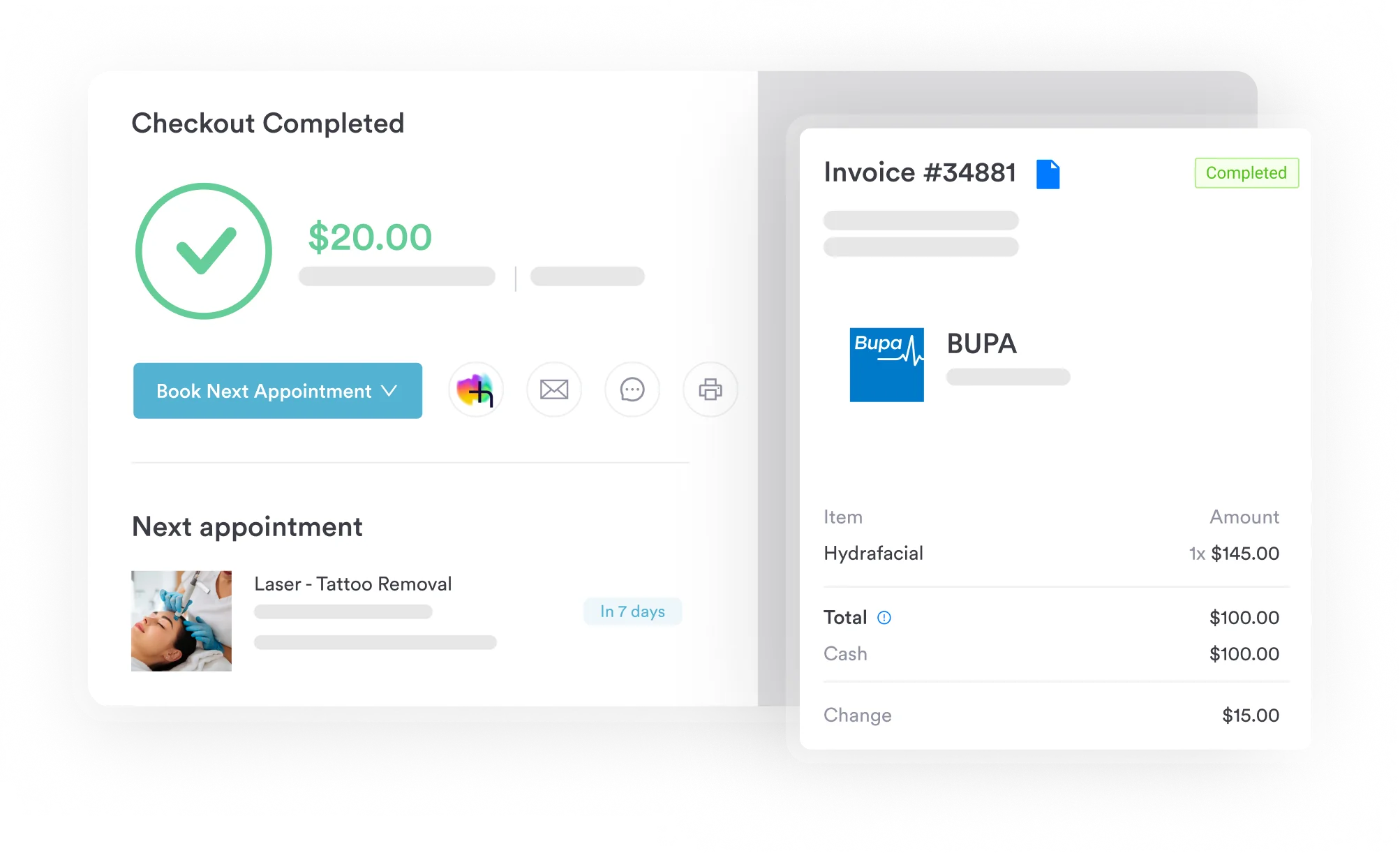
Practice management software like Pabau supports infusion billing workflows: its claims management software links patient records to charge capture, tracks NDC data within the prescription module, and surfaces missing documentation before a claim leaves the practice.
For practices opening an IV clinic or scaling an existing infusion program, a connected system eliminates the manual reconciliation step that produces most J1459 billing errors.
Pabau connects clinical documentation, NDC tracking, and claims management in one platform, so infusion practices submit cleaner claims with fewer manual steps.

J1459 claim errors almost always trace back to one of five root causes: Incorrect unit count, missing NDC, unsupported diagnosis, absent prior authorization, or incomplete documentation. Each is preventable with the right workflow in place before the infusion chair is occupied.
Pabau’s claims management software and integrated digital forms connect the clinical encounter to the billing submission, reducing manual reconciliation and catching incomplete documentation that turns clean infusion encounters into audit targets. For infusion practices ready to tighten their revenue cycle, see how Pabau handles end-to-end infusion billing by booking a demo.
Billing the infusion administration line separately? CPT code 96365 covers the IV infusion administration billing that pairs with drug codes like J1459.
Administering a different biologic infusion? HCPCS code J2323 walks through billing for natalizumab infusions in outpatient infusion clinics.
Running a home infusion program? HCPCS code S9379 covers billing rules specific to home infusion therapy services.
J1459 is the HCPCS Level II code for injection of immune globulin Privigen, intravenous, non-lyophilized (liquid), billed per 500 mg administered. It is used by medical billers to report Privigen infusions under Medicare Part B and most commercial payers when the indication meets coverage criteria under the local coverage determination (LCD) published by the Medicare Administrative Contractor (MAC) that processes the claim. There is no single national LCD for IVIg – for example, First Coast Service Options publishes L29205, but that only applies to Jurisdiction N.
Divide the total grams administered by 0.5 to get the number of units. A 30-gram infusion equals 60 units (30 ÷ 0.5 = 60). Always base units on the documented administered dose, not the ordered or dispensed dose.
Privigen has three FDA-approved indications, each with its own ICD-10-CM codes: Primary immunodeficiency (D80-D84 range, including D83.9 for common variable immunodeficiency), chronic immune thrombocytopenic purpura (D69.3 ITP), and chronic inflammatory demyelinating polyneuropathy (G61.81 CIDP). Coverage for ITP and CIDP is set by each Medicare Administrative Contractor’s own local coverage determination (LCD) – there is no single national LCD for IVIg, so confirm the covered-code list against the LCD that applies to your MAC jurisdiction.
Prior authorization requirements vary by payer. Traditional Medicare Part B does not universally require PA for J1459, but individual MACs may impose additional requirements. Most commercial plans do require prior authorization. Verify with each payer before scheduling the infusion.
J1459 is specific to Privigen (CSL Behring), while J1561 covers Gamunex-C (Grifols). Both are 10% liquid IVIg products billed per 500 mg, but they are distinct HCPCS codes tied to specific branded products. Bill the code that matches the NDC of the product actually administered.
Report the NDC of the specific Privigen vial size administered, in 11-digit format with the N4 qualifier. NDC numbers vary by vial size and can change with packaging updates. Confirm current NDCs from the CSL Behring Privigen coding guide or the product’s package insert rather than relying on static reference lists.