ICD-10 Code M89.9: Disorder of bone, unspecified
M89.9 is billable for disorder of bone, unspecified, and the only M89 code that ...
Last Updated: August 6, 2026
ICD-10 code M43.6 is the billable diagnosis code for torticollis (acquired), valid for FY2026 (October 1, 2025 through September 30, 2026)
M43.6 carries six Excludes1 codes that cannot be coded here: congenital deformity of the sternocleidomastoid (Q68.0), current spine injury, ocular torticollis (R29.891), psychogenic torticollis (F45.8), spasmodic torticollis (G24.3), and torticollis due to birth injury (P15.2)
Documentation must capture onset, laterality, clinical findings, and etiology to support medical necessity for payer review
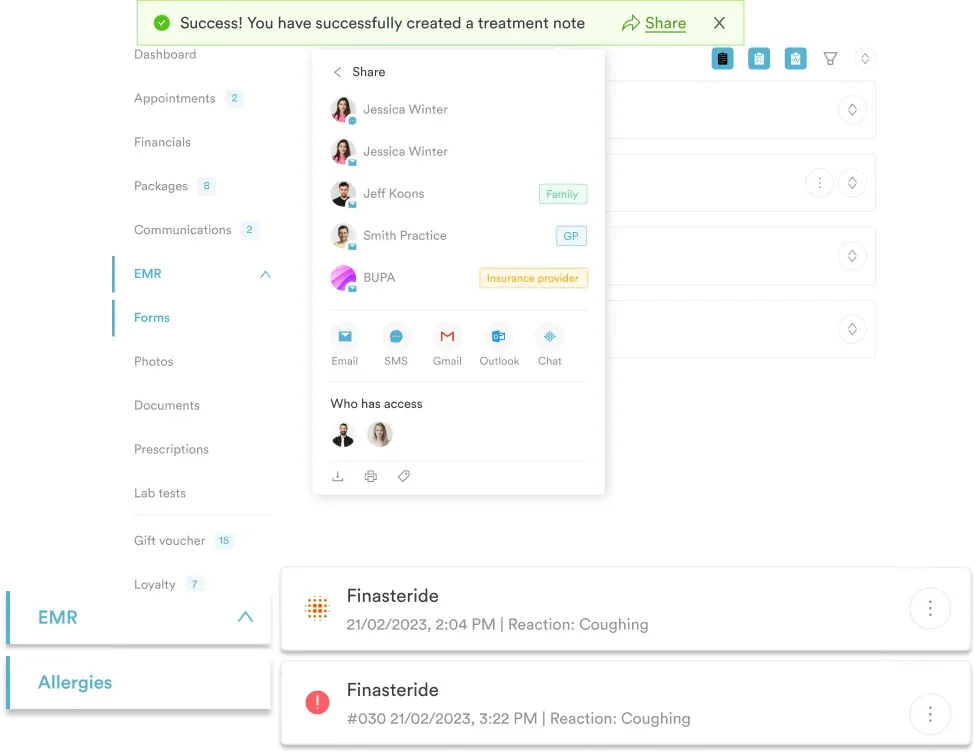
Practice management software like Pabau lets chiropractic and physical therapy practices attach ICD-10 code M43.6 directly to invoices without leaving the patient record
ICD-10 code M43.6 represents Torticollis in the CDC/NCHS ICD-10-CM browser. It is a billable/specific code, meaning it carries sufficient detail for claim submission without requiring a more granular child code. The 2026 edition became effective October 1, 2025 and is valid through September 30, 2026 for HIPAA-covered transactions.
The code sits within Chapter 13 of ICD-10-CM (Diseases of the Musculoskeletal System and Connective Tissue, M00-M99), under the Dorsopathies block (M40-M54), inside the parent category M43 (Other Deforming Dorsopathies).
Torticollis is a condition in which the head tilts or rotates to one side, typically due to muscle spasm or contracture involving the sternocleidomastoid (SCM) muscle. The term derives from the Latin for “twisted neck.” Clinically, it presents as a sustained abnormal head posture that may be painful, stiff, or intermittent.
ICD-10 code M43.6 covers acquired torticollis: cases arising after birth from musculoskeletal causes such as muscle injury, cervical spine pathology, or reactive spasm. It does not cover torticollis arising from neurological, congenital, psychogenic, or birth-injury origins, all of which have their own distinct codes.
Not every torticollis diagnosis maps to M43.6. The correct code depends on the underlying etiology. Selecting the wrong type is the most common audit trigger for this condition.
All exclusions under M43.6 are Excludes1 notes. An Excludes1 note means the excluded condition cannot be coded at the same encounter as M43.6 because they are mutually exclusive diagnoses. If the clinical documentation supports one of these, use that code alone.
The Excludes1 list for M43.6 spans several distinct etiologies, from neurological to congenital. The full list per the CMS ICD-10-CM official files:
Q68.0 (congenital) and M43.6 (acquired) are the pair most commonly confused. The clinical distinction hinges on timing and cause.
Understanding the parent code structure helps coders navigate the WHO ICD-10 classification and select the most precise billable code. This same hierarchy applies to codes across specialties, from musculoskeletal diagnoses to cardiology codes like I35.1.
The M43 category also includes M43.3, a related but distinct dorsopathy that shares the parent code yet requires its own documentation to support billing.
These codes are either commonly co-coded with M43.6 or frequently confused with it. Billing staff at chiropractic practices and musculoskeletal practices should keep this table close during chart review, alongside cervical-region codes like S13.4.
Pabau lets chiropractic and physical therapy practices attach ICD-10 diagnostic codes directly to patient invoices without switching between systems. See how it works for your practice.

M43.6 is paired with CPT procedure codes depending on the treatment delivered. The table below covers the most common pairings seen in chiropractic, physical therapy, and injection-based practices. Always verify current pairing requirements against the AAPC ICD-10-CM crosswalk before submission, as payer LCD policies vary.
Practices using a physical therapy EMR should confirm that their system supports ICD-CPT pairing at the invoice level. In the UK, private practices report procedures under OPCS or CCSD codes rather than CPT — CCSD code 0049C follows the same logic for diagnostic billing outside the NHS.
Note on botulinum toxin injections: Some references pair botulinum toxin injection codes with M43.6. However, botulinum toxin for torticollis is primarily indicated for spasmodic torticollis (G24.3), not acquired musculoskeletal torticollis (M43.6). Coders should verify clinical documentation confirms the etiology before pairing injection codes with M43.6.
Payer review of M43.6 claims focuses on whether the documentation supports medical necessity for acquired torticollis. Missing any of the five key elements below is the most common reason for initial denial. Using a structured chiropractic intake form or following safer clinical notes practices helps ensure each element is captured consistently.
Review the etiology statement in every M43.6 chart note before submission. If the note says ‘muscle spasm’ without explicitly ruling out neurological or congenital causes, add a brief differential documentation line. That single addition reduces denial rates on musculoskeletal torticollis claims significantly.
M43.6 is valid for submission across Medicare, Medicaid, and most commercial payers. Reimbursement is not guaranteed and depends on whether medical necessity criteria are met per each payer’s local coverage determination (LCD). Using claims management software that flags missing diagnosis-procedure pairs before submission can reduce first-pass denials.
Coding reference sites tell you what M43.6 means. Pabau handles what comes next.
Chiropractic and physical therapy practices using Pabau can search and attach ICD-10 code M43.6 directly within the patient record system, then carry that code through to the invoice in one workflow. There is no separate system to open and no manual transcription between lookup and billing.
Using digital clinical forms within the same platform means the documentation elements required for M43.6 (onset, laterality, clinical findings, etiology) are captured in a structured format that survives audit review. The five documentation fields outlined above can be built directly into a Pabau clinical note template for musculoskeletal encounters.
Most M43.6 denials trace back to one of two issues: an excluded etiology coded as acquired torticollis, or documentation that does not explicitly confirm the musculoskeletal origin. Getting both right means fewer resubmissions and faster reimbursement cycles.
Pabau’s integrated ICD-10 code search and structured clinical note templates give chiropractic and physical therapy practices everything needed to code M43.6 accurately at the point of care. Book a demo to see how the workflow looks in practice.
Billing manual therapy for musculoskeletal rehab? CPT 97140 covers the manual therapy techniques often billed alongside chiropractic care for conditions like torticollis.
Need to rule out a psychogenic cause before coding? HCPCS H0031 covers the mental health assessment billing that supports a psychogenic torticollis exclusion.
Ruling out a neurological cause of torticollis? This neurological exam checklist template helps document findings that separate M43.6 from spasmodic torticollis.
ICD-10 code M43.6 is the billable diagnosis code for Torticollis in the ICD-10-CM classification system. It covers acquired torticollis (wry neck) arising from musculoskeletal causes, valid for fiscal year 2026 (October 1, 2025 through September 30, 2026).
The ICD-10 code for torticollis is M43.6. It is billable and specific, meaning it can be submitted directly on a claim without a more detailed child code. It is valid for HIPAA-covered transactions in FY2026.
M43.6 covers acquired musculoskeletal torticollis caused by muscle spasm or cervical pathology; G24.3 covers spasmodic torticollis (cervical dystonia), a neurological movement disorder. They are mutually exclusive under an Excludes1 note, so they cannot be coded together at the same encounter.
The ICD-10 code for congenital torticollis is Q68.0 (Congenital deformity of sternocleidomastoid muscle). It is listed as an Excludes1 code under M43.6, meaning it cannot be used alongside M43.6 when the condition is congenital in origin.
Yes, M43.6 is a valid torticollis billing code for FY2026. Reimbursement still requires that documentation supports medical necessity, including onset, laterality, clinical findings, and confirmation of a musculoskeletal rather than neurological etiology.
Documentation must capture onset and duration (confirming acquired origin), laterality, objective clinical findings (range of motion, palpable spasm), a stated musculoskeletal etiology ruling out neurological or congenital causes, and a treatment plan. Missing any of these is the most common trigger for denial.