Capsular contracture: causes, grading, and treatment options
What is capsular contracture? Capsular contracture is the most common long-term ...
Last Updated: August 4, 2026
A pediatric neurological exam checklist covers six core domains (mental status, cranial nerves, motor function, sensory assessment, reflexes, and cerebellar testing), plus the pediatric-specific layer: primitive reflexes and developmental milestones scored against the child’s age.
With children you rarely examine in textbook order. Lead with observation during play, save distressing maneuvers for last, and involve the caregiver so a squirming toddler still yields a complete record.
Persistence of primitive reflexes past 4 to 6 months, or loss of milestones a child had already reached, are red flags that warrant urgent referral rather than watchful waiting.
Practice management software like Pabau turns the checklist into a digital form, so findings drop straight into the child’s structured record and stay comparable at the next visit.
A structured checklist covering mental status, cranial nerve testing, motor and sensory assessment, reflexes, cerebellar function, and red-flag recognition for pediatric neurological evaluation in clinical practice.
Download templateA pediatric neurological exam checklist is a clinical tool for systematically assessing a child’s nervous system. It covers primitive reflexes, developmental milestones, and behavioral cooperation alongside the cranial nerve, motor, and sensory domains of a standard neuro exam. Whether you’re evaluating a child with developmental concerns or running a routine screen, the checklist keeps the assessment complete when the patient will not sit still for it.
A neurological exam checklist breaks a full nervous system evaluation into organized, testable components. It captures mental status, cranial nerve function (CN I-XII), motor strength and tone, sensory perception, deep tendon reflexes, and cerebellar coordination. The pediatric version adds two things the adult exam does not need: primitive reflexes and developmental milestones, both scored against what is normal for the child’s age.
The point of a checklist is to standardize the exam so you assess every domain the same way each time, rather than relying on memory. A documented exam also creates a baseline. If symptoms change, the next clinician can see exactly what was normal before, which supports diagnostic reasoning and continuity of care across a multidisciplinary team.
With adults you work through the domains in order. With children you do not, because a crying toddler makes half the exam impossible. The order below front-loads what you can observe passively and holds the distressing maneuvers until the end.
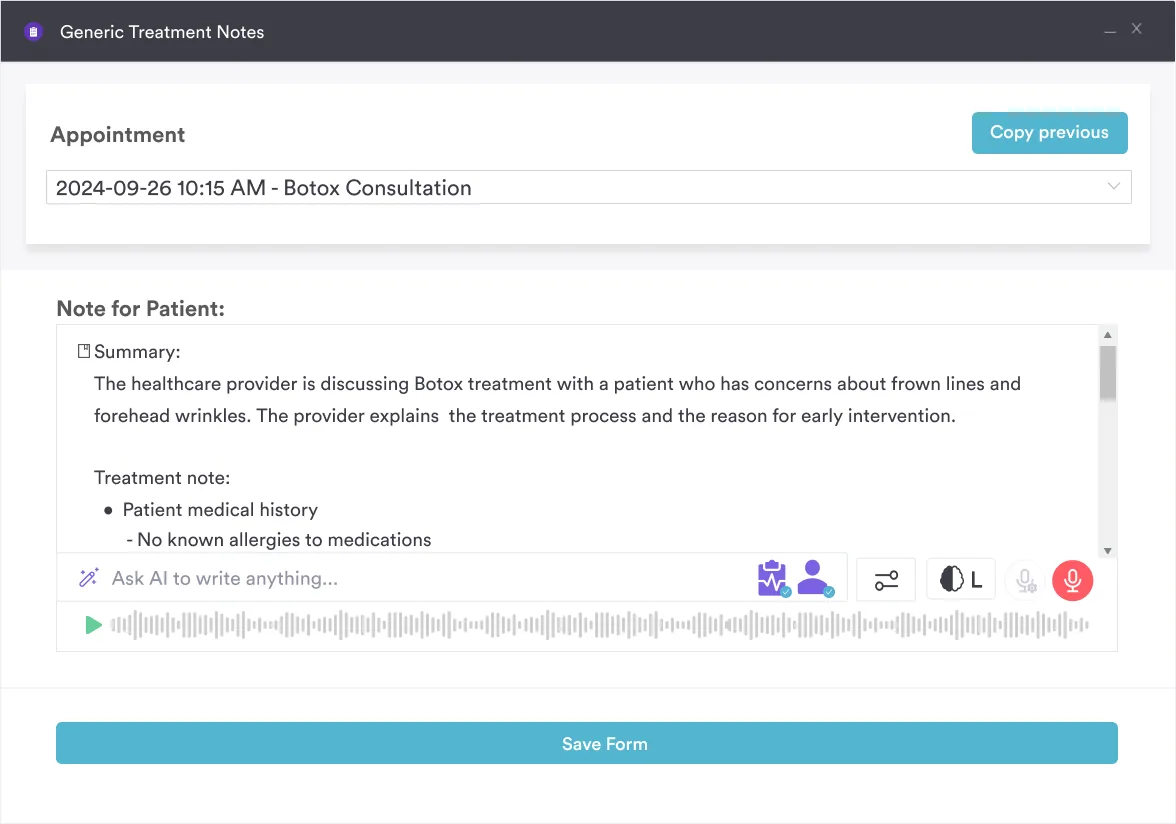
Document findings in SOAP note structure using precise, measurable language rather than subjective phrases. A focused rapid exam of selected domains takes 5 to 10 minutes; a comprehensive exam covering all domains takes 15 to 30 minutes. Once the findings are gathered, AI-powered documentation tools can speed up note entry.
This is the part of the pediatric exam that has no adult equivalent, and it is where a generic checklist falls short. Primitive reflexes are normal in infancy and should integrate (disappear) on a predictable schedule as the nervous system matures. Their timing is the signal: a reflex that lingers too long, or that never appeared when it should have, points to a problem.
Persistence of primitive reflexes past 4 to 6 months is associated with cerebral palsy and other central nervous system disorders, per StatPearls. Pair the reflex check with developmental milestones (gross motor, fine motor, language, and social) scored against the child’s age, and note explicitly whether the child is meeting, exceeding, or falling behind expected norms. Treat exact ages as approximate windows, not rigid cutoffs.
This checklist serves several disciplines, each using the version that fits its scope of practice:
Compliance and documentation. A thorough, documented exam demonstrates systematic assessment relevant to the presenting complaint, which is what professional standards and medical boards expect. Consistent records also stand up better to later review.
Diagnostic accuracy and safety. Systematic evaluation reduces missed red flags, such as asymmetric pupils suggesting raised intracranial pressure, hyperreflexia indicating upper motor neuron disease, or one-sided weakness hinting at stroke. Early recognition enables timely specialist referral.
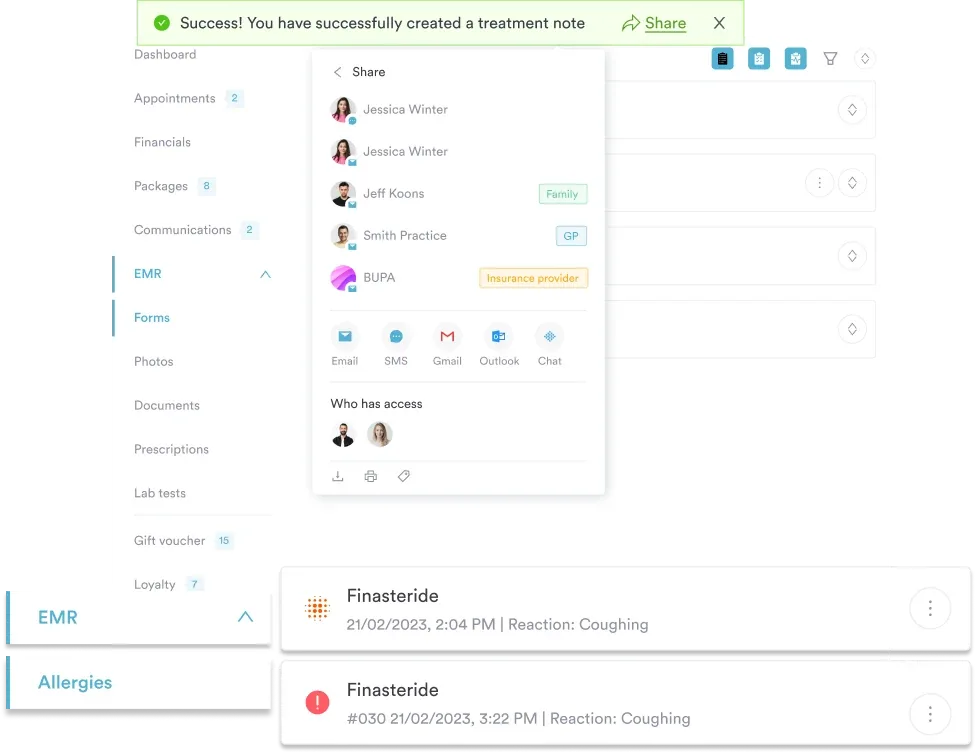
Continuity of care. Structured documentation creates a baseline for team-based care. If a child returns weeks later with new symptoms, the prior exam gives the context to judge what has changed. Client record systems that store neurological findings make that comparison instant.
Workflow efficiency. A printed or digital checklist keeps the exam on track and prevents omissions, so you spend less time deciding what to assess next. Digital patient intake forms capture data straight into the record and remove the transcription step.
For infants and toddlers, record the exact age at which each primitive reflex is present or absent (e.g., ‘Moro absent at 7 months, ATNR persists’). Reflex timing is more informative than a single snapshot, and dated entries let you track integration across visits.
Red flags are findings that signal urgent or emergent pathology and require prompt specialist referral or emergency care. Recognizing them is the most clinically important use of the checklist.
Document red-flag findings immediately and escalate care. For structured guidance on pediatric neurological assessment, the University of Utah pediatric neurologic exam and Nationwide Children’s Hospital are useful references.
Once the exam is complete, translate the findings into the child’s record using SOAP note format. The checklist findings populate the Objective section: document what you observed and measured (pupils, reflexes, strength grades, reflex integration) without interpretation. The Assessment interprets them, for example “normal exam for age” or “persistent Moro at 8 months, refer to pediatric neurology.” The Plan sets next steps: reassurance, imaging, or referral.
Storing findings in a structured record keeps them accessible to the next clinician and supports longitudinal assessment. With practice management software like Pabau, digital forms auto-populate SOAP sections from checklist responses, which cuts documentation time and keeps entries consistent across the care team.
Schedule a demo to see how Pabau’s clinical documentation workflow connects to examination checklists.
The right equipment and setting make the assessment accurate and less distressing for the child. Essential supplies include:
Keep the room quiet, well-lit, and comfortable. Patient care management best practices call for a private, respectful setting where patients feel safe, which matters most with young children who may be anxious about being examined. Let the caregiver stay close, and ensure adequate privacy when sensory testing requires exposing the extremities.
Screening for pediatric ADHD alongside a neuro exam? ADHD handout for parents gives families a plain-language explanation to pair with your clinical findings.
Assessing developmental red flags in young children? Autism pattern recognition test adds a structured screening layer alongside primitive reflex and developmental checks.
Need a focused test for upper limb motor function? Action Research Arm Test breaks grasp, grip, and reach down into scorable tasks.
A pediatric neurological exam checklist turns an ad-hoc assessment into a systematic evaluation of every relevant domain, from primitive reflexes through cranial nerve function. Across primary care, pediatrics, mental health, and rehabilitation, that structure reduces missed diagnoses, improves safety, and produces documentation that holds up over time. The template above is ready to download and customize for your practice.
Pairing the checklist with Pabau’s digital forms and client record system lets your practice capture findings in real time, share them with the whole care team, and build a record that supports continuity of care while cutting administrative work.
The six core components are mental status (alertness, orientation, cognition), cranial nerves (CN I-XII function), motor assessment (strength, tone, gait), sensory function (light touch, proprioception, vibration), reflexes (deep tendon reflexes, Babinski sign), and cerebellar testing (coordination, balance, tremor). A pediatric checklist adds primitive reflexes and developmental milestones scored for the child’s age.
Lead with observation while the child plays, gather cranial nerve and motor findings opportunistically using toys and the caregiver, and save any startling or uncomfortable maneuvers (like reflex testing) for the end. Involving the caregiver and turning tests into games captures a complete exam without forcing textbook order.
Document the specific finding precisely (e.g., “1/5 weakness in left lower extremity, unable to lift leg against gravity”), assess whether it meets red-flag criteria, and escalate accordingly by ordering imaging, referring to neurology, or sending the child to the emergency department for acute findings such as stroke symptoms.
A screening exam (5 to 10 minutes) tests key components to rule out obvious pathology, typically mental status, gross motor strength, and pupillary response. A comprehensive exam (15 to 30 minutes) evaluates all domains in detail, including subtle findings like proprioception or individual cranial nerve function, and is used when symptoms suggest neurological disease.
Most primitive reflexes integrate by around 4 to 6 months: the Moro, palmar grasp, and asymmetric tonic neck reflex all fade in that window, while the plantar grasp persists to about 9 to 12 months. An upgoing Babinski response is normal until roughly age 2. Persistence beyond these windows is a red flag associated with cerebral palsy.
Red flags that warrant urgent escalation include loss of previously acquired milestones, persistent or absent primitive reflexes, a sudden or rapidly progressing deficit, asymmetric findings such as one-sided weakness, altered consciousness, and a new severe headache with neurological signs. Any of these should prompt immediate imaging or specialist referral.