ICD-10 Code L88: Pyoderma gangrenosum coding reference
L88 is the billable ICD-10-CM code for pyoderma gangrenosum. One Excludes1 note ...
Last Updated: August 4, 2026
ICD-10 code M43.3 describes recurrent atlantoaxial dislocation with myelopathy, a condition involving repeated C1-C2 joint displacement with spinal cord compression.
M43.3 is a billable ICD-10-CM code valid for FY2026 (effective October 1, 2025 through September 30, 2026) and accepted for all HIPAA-covered transactions.
The most common coding error is using M43.4 (other recurrent atlantoaxial dislocation) when myelopathy is explicitly documented. M43.3 requires confirmed neurological findings.
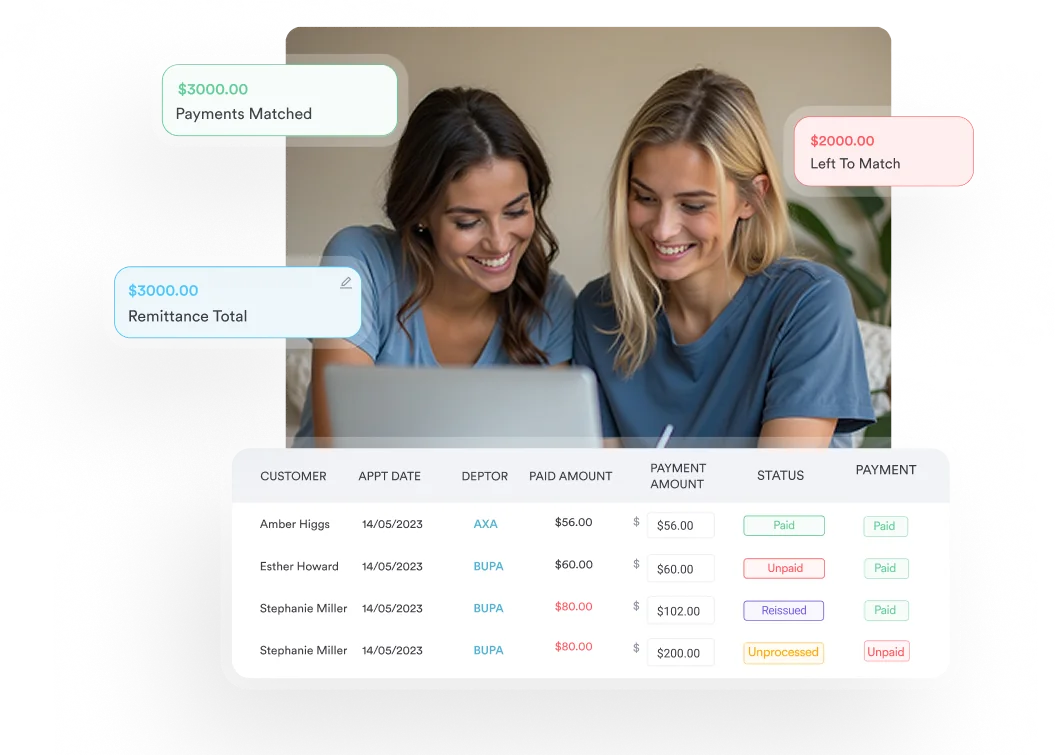
Pabau’s claims management software and structured clinical records help providers capture the documentation needed to support M43.3 without manual errors.
ICD-10 code M43.3 is the billable diagnosis code for recurrent atlantoaxial dislocation with myelopathy: Repeated displacement of the C1-C2 joint with confirmed spinal cord involvement. Physicians assign it only when a prior dislocation episode and current neurological deficits are both documented, distinguishing it from the more general M43.4.
M43.3 is a billable, specific ICD-10-CM code valid for use in all HIPAA-compliant documentation and reimbursement transactions. The FY2026 edition became effective on October 1, 2025, and remains valid through September 30, 2026.
The short description is “Recurrent atlantoaxial dislocation w/ myelopathy.” The long description is “Recurrent atlantoaxial dislocation with myelopathy.” This code sits within the M43 category (Other deforming dorsopathies), which falls under the M40-M43 block and the broader M00-M99 musculoskeletal and connective tissue chapter.
According to CMS, ICD-10 code M43.3 is valid for use across all payer types covered by ICD-10-CM reporting requirements.
The table below summarizes the key reference fields coders and billing staff need when working with the M43.3 diagnosis code.
Coders and clinicians sometimes enter condition descriptions before code numbers in their EHR. The following alternate terms all map to M43.3 and are accepted in crosswalk and encoder searches. Familiarity with these helps prevent mismatch when querying coded diagnoses against clinical notes referencing a related cervical spine code such as S13.4.
These synonyms are clinically equivalent for coding purposes. However, the physician documentation must explicitly confirm both recurrence and myelopathy for M43.3 to be a valid code assignment.
The atlantoaxial joint connects the atlas (C1) and axis (C2) vertebrae at the top of the cervical spine. This joint allows roughly 50% of all head rotation and is stabilized by the transverse atlantal ligament and alar ligaments. When those stabilizers are compromised, the C1-C2 joint can sublux or dislocate, potentially compressing the spinal cord in the narrow atlantoaxial canal.
Recurrent dislocation means the displacement has occurred more than once, distinguishing M43.3 from a first-episode event. Myelopathy indicates the spinal cord itself is affected, producing neurological signs beyond localized neck pain. Common causes include rheumatoid arthritis (which erodes the transverse ligament), Down syndrome (ligamentous laxity), trauma sequelae, and congenital abnormalities.
Clinicians working in physical therapy documentation workflows and neurosurgery frequently encounter this condition when patients present with progressive upper motor neuron signs after a prior atlantoaxial event. ICD-10 code M43.3 captures the full clinical picture: Anatomical recurrence plus cord involvement.
Documenting myelopathy is a prerequisite for M43.3. The following findings support that documentation:
The diagnostic workup typically proceeds from plain cervical radiographs to CT (bony anatomy) to MRI (cord signal, soft tissue). According to the CDC/NCHS ICD-10-CM web tool, accurate code assignment depends on physician documentation linking radiographic findings to the neurological examination, not radiology reports alone.
M43.3 sits within category M43 (Other deforming dorsopathies). Understanding the hierarchy helps coders navigate adjacent codes and avoid selecting an overly broad parent code. The table below shows the relevant M43 siblings most commonly encountered alongside M43.3.
Because M43.3 and M43.4 share the same parent and the same anatomical site, the distinction hinges entirely on whether myelopathy is documented. The non-billable parent M43 should never be submitted for reimbursement when a more specific child code applies. Coders managing codes like M47.812 in similar spinal categories will recognize this specificity requirement as standard across the chapter.
The differentiation between M43.3 and M43.4 is the most common coding error in this subcategory. Both codes describe recurrent atlantoaxial dislocation, but only one requires documented myelopathy.
The practical rule: If the attending physician documents any neurological deficit attributable to cord compression at C1-C2, M43.3 is the correct code. If the note describes instability or recurrent dislocation without neurological findings, M43.4 applies. Never infer myelopathy from imaging alone. Physician attestation is required.
Check the neurological exam section of the note, not just the imaging report. Radiologists may note cord contact or mild compression on MRI, but myelopathy as a coded diagnosis requires the treating physician to document clinical signs of cord dysfunction. Imaging findings alone do not justify M43.3.
Coders frequently encounter the following codes in the same encounter or as secondary diagnoses when billing M43.3. The AAPC Codify ICD-10-CM lookup is a useful tool for confirming hierarchy and sequencing rules across these related codes.
Pabau helps clinics capture structured clinical notes, ICD-10 codes, and claim-ready records in one place. See how it supports musculoskeletal and spinal documentation workflows.

Accurate code assignment depends on what is in the medical record, not on the clinical presentation alone. The ICD-10-CM Official Guidelines for Coding and Reporting require that the diagnosis be coded to the highest degree of specificity supported by documentation. For M43.3, that means four elements must all be present in the physician’s note.
Practices using chiropractic practice software with structured note templates reduce the risk of incomplete documentation because key fields for recurrence history, neurological exam findings, and imaging references are built into the encounter workflow rather than left to free-text entry.
The ResDAC Medicare ICD reference explains how diagnosis codes submitted on claims are validated against documented clinical criteria, making complete documentation a billing prerequisite, not just a clinical one.
These four errors generate the majority of denials and audit flags on claims using M43.3 or adjacent M43 codes. Teams billing anesthesia codes such as CPT 00600 alongside M43.3 procedures will recognize these patterns.
A structured documentation workflow linking the encounter note to the assigned diagnosis code before submission — whether that code is M43.3 or another musculoskeletal diagnosis such as M47.9 — catches most of these errors before the claim leaves the practice. Coders should also review the ICD10Data.com M43.3 page for code edits and any payer-specific coverage determinations.
Query the provider if you see cord contact or compression on the MRI report but no myelopathy language in the clinical note. A brief provider query prevents both undercoding (M43.4 when M43.3 is appropriate) and overcoding (M43.3 without the clinical basis). Document the query and response in the chart.
Accurate M43.3 coding depends on structured documentation that captures all four required elements at the point of care, before the claim is built. Missing one element at note completion means a coder query, a delayed claim, or a denial.
Practice management software like Pabau links the clinical record directly to the billing workflow through its claims management features, cutting down on the coder queries, delayed claims, and denials that missing documentation causes.
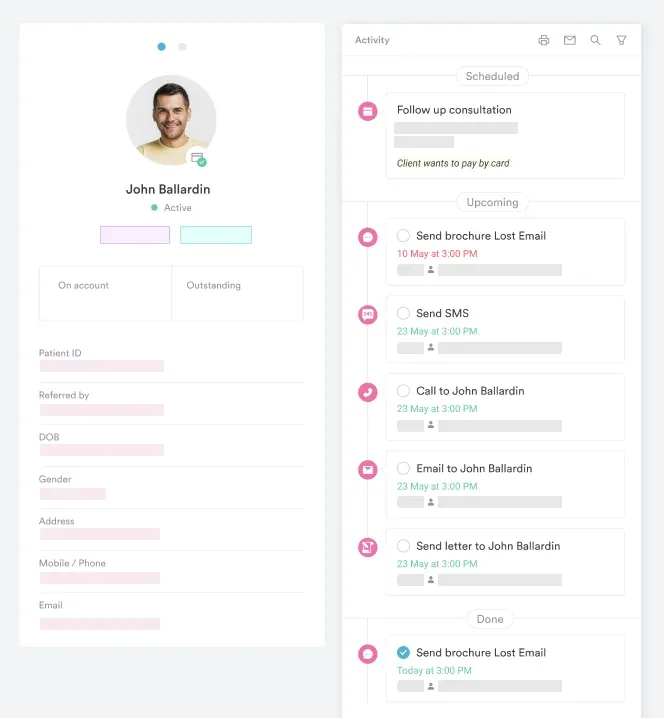
With structured clinical records, providers can build encounter templates that include dedicated fields for recurrence history, neurological examination findings, imaging results, and physician attestation. These fields feed directly into the claim record rather than sitting in unstructured text. The result is a chart that coders can review against M43.3 criteria without having to chase free-text notes across multiple documents.
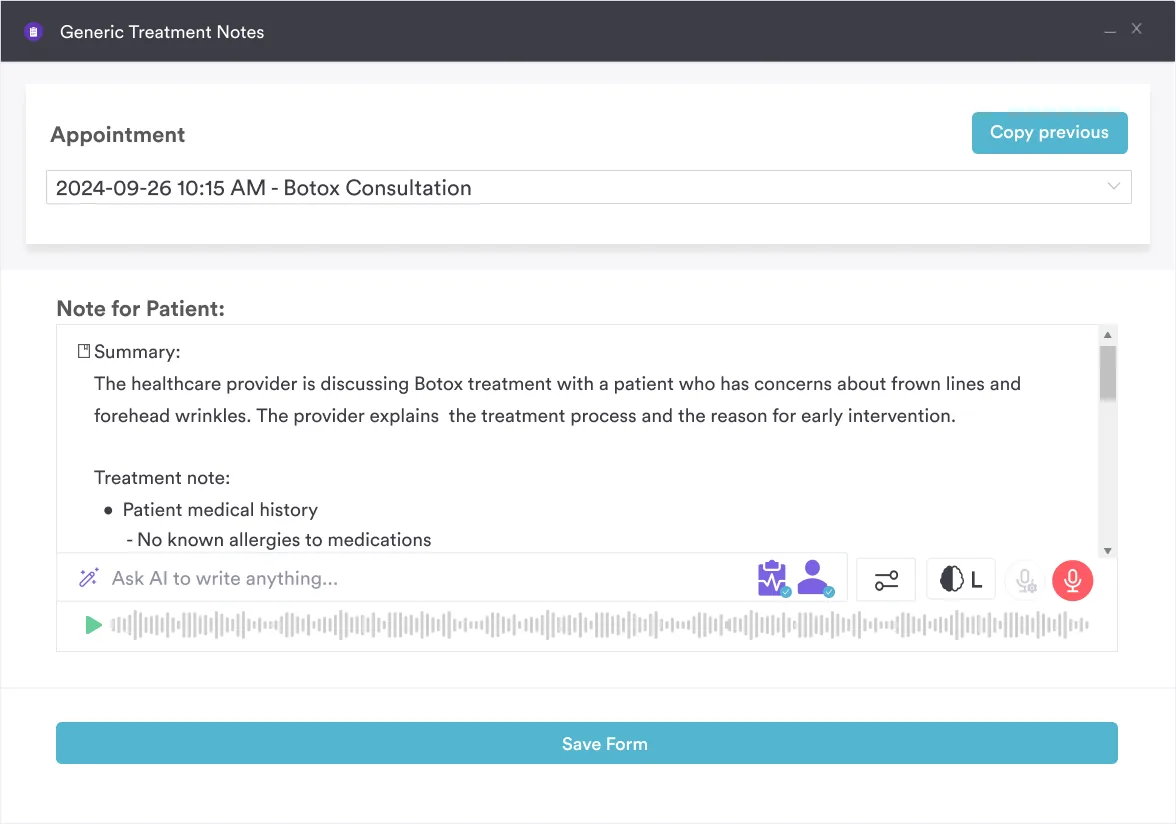
Pabau’s AI-assisted clinical documentation can also transcribe and structure consultation notes in real time, capturing neurological exam findings and recurrence language as the provider speaks rather than relying on post-encounter recall.
For practices managing complex spinal patients across multiple encounters, this cuts down on the coding queries that incomplete notes generate. Structured digital intake forms further support M43.3 accuracy by capturing prior episode history and current symptom patterns before the consultation begins.
ICD-10 code M43.3 requires both recurrence and documented myelopathy: Two conditions that must be explicitly present in the physician’s note before the code can be assigned. The most expensive coding mistake in this subcategory is the M43.4/M43.3 mix-up, and it is entirely preventable with a structured documentation review at the point of care.
Pabau’s structured clinical records and claims management tools help practices capture the documentation M43.3 demands before the claim is built, reducing queries, denials, and audit exposure. To see how Pabau supports musculoskeletal and spinal documentation workflows, book a demo.
Coding for related musculoskeletal comorbidities? M16.0 covers bilateral primary hip osteoarthritis, a common comorbidity documented alongside chronic cervical spine conditions.
Need a catch-all for non-specific soft tissue findings? M79.9 is the default code when soft tissue disorder documentation doesn’t support a more specific diagnosis.
Billing rehabilitation services alongside M43.3 care? CPT 97799 covers unlisted physical medicine and rehabilitation procedures that don’t fit a standard code.
ICD-10 code M43.3 is used to report a diagnosis of recurrent atlantoaxial dislocation with myelopathy, a condition involving repeated displacement of the C1-C2 joint accompanied by spinal cord compression and associated neurological deficits. It is a billable code used for medical claim reimbursement when both recurrence and myelopathy are documented by the treating physician.
Yes, M43.3 is a billable and specific ICD-10-CM code valid for FY2026 (effective October 1, 2025 through September 30, 2026). It is accepted for all HIPAA-covered transactions and can be submitted on claims to indicate this specific diagnosis for reimbursement purposes.
M43.3 requires documented myelopathy (spinal cord dysfunction with neurological findings), while M43.4 (other recurrent atlantoaxial dislocation) applies when the dislocation recurs without cord involvement. Both require documented recurrence, but M43.3 demands physician-documented neurological deficits such as weakness, spasticity, or sensory changes. Using M43.4 when myelopathy is present is the most common coding error in this subcategory.
Four documentation elements are required: Confirmation of a prior atlantoaxial episode (recurrence), identification of the C1-C2 anatomical site, physician-documented neurological findings attributable to cord compression (not imaging alone), and corroborating imaging such as MRI or CT showing atlantoaxial instability. All four must appear in the treating physician’s note, not the radiology report.
Accepted alternate terms include: Recurrent C1-C2 dislocation with myelopathy, recurrent atlantoaxial subluxation with cord compression, recurrent upper cervical dislocation with myelopathy, and atlantoaxial dislocation recurrent with spinal cord compression. These synonyms are used in EHR encoders and crosswalk tools and all map to M43.3 when myelopathy is confirmed.
CPT codes commonly paired with M43.3 include cervical spine MRI (CPT 72141, 72142), cervical CT (72125, 72126), cervical fusion procedures (22590 for occiput-C2, 22595 for atlas-axis/C1-C2 arthrodesis), and posterior decompression codes (63001, 63015). Specific pairings depend on the treatment provided and the individual payer’s coverage policies. Verify medical necessity requirements with each payer before billing.