ICD-10 code S42.409P: Unspecified fracture of lower end of humerus with malunion
ICD-10 code S42.409P: Quick reference and billable status ICD-10 code S42.409P i...
Last Updated: July 31, 2026
ICD-10 Code H53.2 is the billable diagnosis code for Diplopia (double vision), classified under Chapter 7: Diseases of the eye and adnexa
H53.2 is valid for binocular diplopia; when an underlying cause is identified, code the etiology first and use H53.2 as a secondary code
Documentation must distinguish monocular from binocular diplopia and capture ocular deviation measurement to support medical necessity and reduce audit risk
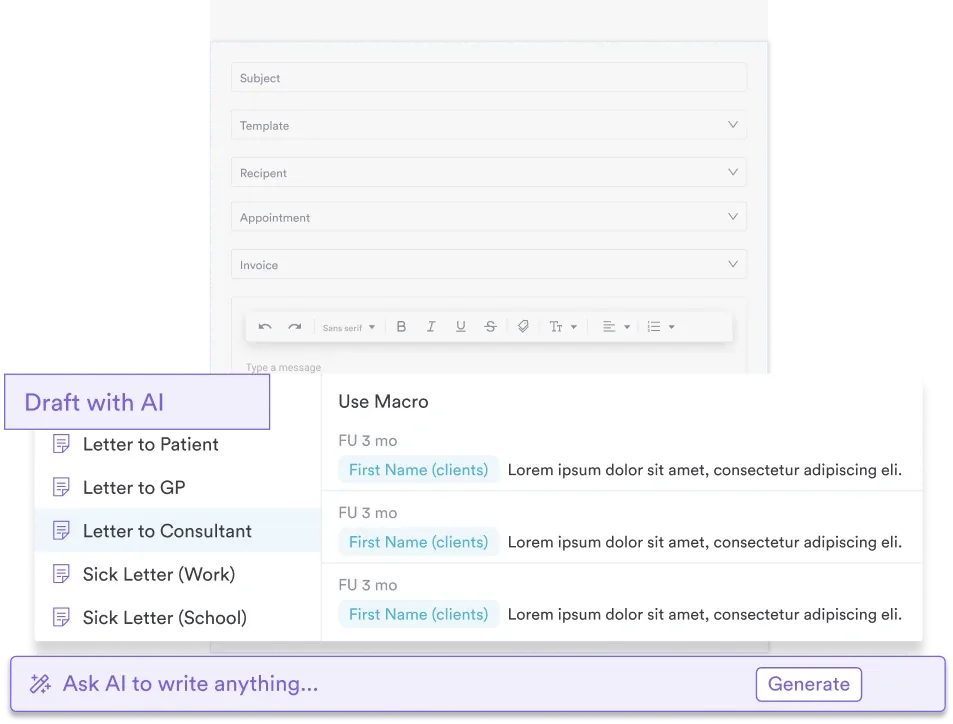
Pabau’s claims management software and digital intake forms help ophthalmology and eye care practices document H53.2 encounters accurately and submit clean claims
ICD-10 Code H53.2 is the diagnosis code ophthalmologists, neurologists, and primary care clinicians use to document diplopia, or double vision. H53.2 works both as a standalone diagnosis and as a secondary code once an underlying cause is identified, so correct sequencing has a direct effect on claim acceptance.
This guide covers the code’s definition, billing rules, documentation requirements, and how it relates to nearby H53 codes.
ICD-10 Code H53.2 is the billable ICD-10-CM diagnosis code for diplopia, or double vision. It sits under the H53-H54 range covering visual disturbances and blindness within Chapter 7 of the ICD-10-CM classification.
Coders and clinicians in ophthalmology, neurology, and general practice use this code regularly. Sequencing errors and incomplete documentation are common causes of denied claims in eye care billing.
Diplopia is the clinical term for seeing two images of a single object. It can be binocular, present with both eyes open and resolving when either eye is covered, or monocular, persisting even when one eye is closed.
The CDC/NCHS ICD-10-CM tool lists H53.2 as valid for fiscal year 2026. Its ICD-9 predecessor was code 368.2, which carried a direct one-to-one crosswalk when the US transitioned to ICD-10-CM in October 2015.
This section covers the clinical definition, billability, documentation rules, sequencing conventions, related codes, and the IRIS56 quality-improvement measure that ties into H53.2 encounters in ophthalmology practices.
H53.2 is a fully billable ICD-10-CM diagnosis code. It can be submitted on a claim without requiring a more specific sub-code, making it a leaf node in the ICD-10-CM hierarchy. According to the AAPC Codify ICD-10-CM lookup, H53.2 is classified by the World Health Organization under the Visual disturbances and blindness range and carries these official attributes:
Practices using claims management software that supports ICD-10-CM code validation can flag H53.2 automatically when documentation does not include the required clinical specificity, reducing the chance of a clean claim going out with insufficient supporting detail.
H53.2 applies when a patient presents with diplopia and no underlying etiology has been identified or confirmed at the time of the encounter. When the cause is known, ICD-10-CM sequencing conventions require coding the underlying condition first. H53.2 then moves to a secondary position as a manifestation code.
Common etiologies that would shift H53.2 to a secondary code include:
When diplopia is the presenting complaint and the workup is still underway, H53.2 is appropriate as the principal diagnosis for that encounter. The same principal-vs-secondary sequencing logic applies to isolated cranial nerve palsy codes like H49.12: code what is confirmed at the time of the encounter, not the suspected final diagnosis.
Document the laterality and type of diplopia in every H53.2 encounter. Note whether diplopia is binocular (resolves on covering one eye) or monocular (persists with one eye covered). Binocular diplopia has different etiological implications than monocular diplopia, and payers increasingly request this distinction during audit reviews.
Because H53.2 is a symptom code, its position on the claim can change as the workup progresses. This two-encounter example shows how the sequencing shifts once an etiology is confirmed:
The rule to remember: code what is confirmed at the time of the encounter, and update the sequencing at each subsequent visit as the diagnosis becomes clearer.
Coding H53.2 accurately starts with the clinical note, not the claim form. Incomplete documentation is the primary reason auditors downcode or deny diplopia-related claims. The CMS ICD-10-CM guidelines require that the diagnostic statement in the record support the code assigned, and H53.2 encounters have specific elements that need to be present.
Practices that use digital intake forms can structure the ophthalmology history-taking workflow to capture these elements before the patient sees the clinician. Pre-populating visual symptom fields, gaze complaint descriptions, and onset details reduces the documentation burden at point of care.
A structured eye movement test and a routine CPT 92002 exam can supply the gaze-position and deviation detail auditors look for. For practices managing high volumes of eye care documentation, structured medical forms improve consistency across encounters and reduce the per-chart audit exposure from incomplete records.
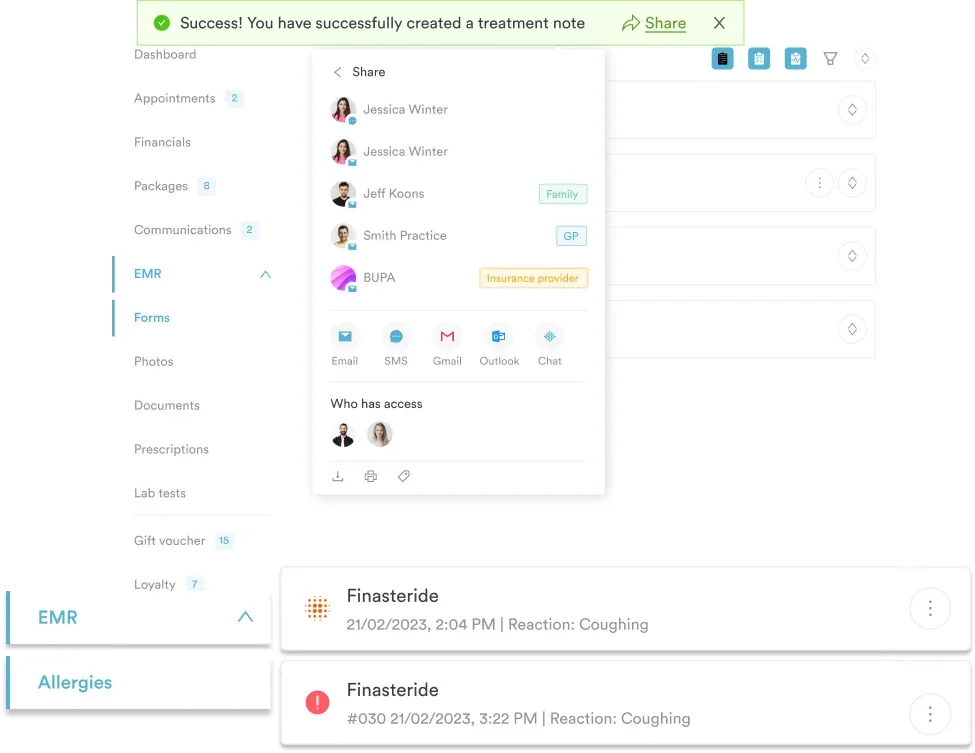
Pabau helps ophthalmology and eye care practices capture structured clinical documentation, manage ICD-10 coded records, and submit clean claims, all from one platform.

H53.2 sits within the broader H53 subcategory. Understanding the adjacent codes helps coders select the most specific option and avoid defaulting to H53.2 when a more precise code exists. The ICD10Data H53 reference provides a useful overview of the full H53 family.
The distinction between H53.2 and H53.8 is clinically meaningful. H53.8 covers “other visual disturbances,” including situations where a patient reports seeing multiple images but the pattern does not fit the classic diplopia definition.
H53.9 (unspecified visual disturbance) should not be used when the clinical note clearly documents diplopia as the presenting complaint. The same caution applies elsewhere in ophthalmic coding: unspecified codes such as H49.9 draw the same audit scrutiny when a more specific code was available in the documentation.
The same principal-vs-secondary sequencing logic extends to other ocular motility codes, including H49.40, where the confirmed diagnosis is sequenced first and H53.2 is added only if diplopia persists as a distinct symptom.
H53.2 and H53.8 are frequently confused. The test is straightforward: if the patient describes seeing two separate images of a single object, the clinical term is diplopia and H53.2 applies. If the visual complaint involves multiple images, distortions, or patterns that do not fit the binocular double vision definition, H53.8 is the better fit.
Monocular diplopia is another common coding question. The inclusion term in H53.2 specifies binocular diplopia. Monocular diplopia, which persists when the other eye is covered, generally reflects a refractive or corneal issue, such as H18.10, rather than a neuromuscular one.
Some coders default to H53.2 for monocular presentations, but documentation should clearly support this. When monocular diplopia is the complaint and the note does not specify binocular, H53.8 or a more specific lens/cornea code may be more defensible.
Review your documentation before claim submission: if the note says ‘binocular diplopia’ or ‘double vision with both eyes open,’ H53.2 is correct. If the note documents diplopia in one eye only, or if the complaint resolves on closing the fellow eye but not the affected eye, reassess whether H53.2 or a more specific code is appropriate.
Ophthalmology practices participating in the AAO’s IRIS Registry should be aware that H53.2-coded encounters may be tracked under the IRIS56 quality-improvement measure. IRIS56 is not approved for MIPS reporting and is not a MIPS-scored measure.
According to the AAO IRIS56 measure page, this measure tracks the percentage of adult diplopia patients who achieve improvement of ocular deviation. Improvement means reducing strabismus in primary gaze to less than 10 prism diopters horizontal or less than 2 prism diopters vertical, or achieving absence of diplopia or functional improvement.
This has direct documentation implications. For any H53.2 encounter that may contribute to IRIS56 reporting:
Practices using AI-assisted clinical documentation can structure templates to prompt for these measurement fields during ophthalmology encounters, reducing the risk of missing IRIS56-relevant data points after the patient has left.
For EHR for private practice ophthalmology settings, building these prompts into the encounter workflow is far more reliable than relying on retrospective chart review.
Diplopia coding draws audit attention in two specific scenarios: when H53.2 is used as a primary diagnosis despite a known underlying condition appearing elsewhere in the record, and when the claim includes imaging orders that do not match the documented clinical picture.
The most common errors in H53.2 coding include:
Practices managing ophthalmology coding through EHR integration for ophthalmology benefit from audit trail visibility. When a payer requests documentation for an H53.2 claim, the complete encounter record, including the assessment, orders, and follow-up plan, is accessible in one system.
Patient record management that keeps all encounter data linked to the coded visit reduces the administrative burden of responding to post-payment audits.
Coders working across multiple specialties in one system may also want to check a few of our newest coding and documentation guides, including CPT 00322, HCPCS J1940, and our emotional support animal template.
ICD-10 Code H53.2 is the correct billable code for diplopia when documentation supports the diagnosis and no confirmed etiology has been coded as primary. The sequencing rules, documentation requirements, and IRIS56 quality measure linkage make H53.2 encounters more documentation-intensive than a simple code lookup suggests.
Practice management software like Pabau helps eye care and ophthalmology practices structure their clinical documentation, from intake through to primary care EHR workflows that keep sequencing notes tied to the coded visit. To see how Pabau handles ophthalmology documentation end-to-end, book a demo.
Need a structured approach to ophthalmology EHR workflows? EHR integration for ophthalmology covers how to connect your clinical record system with billing and coding workflows.
Managing billing across multiple specialties? Claims management software from Pabau helps practices reduce denial rates with ICD-10-coded claim validation built into the submission workflow.
Looking to reduce documentation burden at point of care? Structured medical forms explores how pre-built clinical form templates reduce per-encounter documentation time.
ICD-10 Code H53.2 is the billable ICD-10-CM diagnosis code for Diplopia, the clinical term for double vision, classified under Chapter 7 (Diseases of the eye and adnexa) in the H53-H54 Visual disturbances and blindness range. It is valid for fiscal year 2026 and carries a direct one-to-one crosswalk from ICD-9 code 368.2.
Yes, H53.2 is a fully billable ICD-10-CM diagnosis code for fiscal year 2026. It does not require a more specific sub-code to submit on a claim, though the supporting clinical documentation must clearly establish diplopia as the diagnosis for the encounter.
H53.2 (Diplopia) applies when a patient sees two separate images of a single object, specifically binocular double vision. H53.8 (Other visual disturbances) covers visual complaints that do not fit the diplopia definition, including multiple images in patterns that do not resolve on covering one eye. Use H53.2 when the note specifically documents diplopia; default to H53.8 only when the presentation does not clearly meet that threshold.
Use H53.2 as the principal diagnosis when diplopia is the presenting complaint and the underlying etiology has not yet been confirmed. Once an underlying cause such as cranial nerve palsy, thyroid eye disease, myasthenia gravis, or strabismus is established, code that condition first and list H53.2 as a secondary code, or remove it if it is fully explained by the primary diagnosis code.
H53.2 is used when the etiology is unconfirmed. Conditions that commonly cause diplopia, and which would become the primary code once confirmed, include cranial nerve palsies (third, fourth, sixth nerve), thyroid eye disease, myasthenia gravis, multiple sclerosis, and strabismus. When any of these is documented as confirmed, the specific condition code takes the principal position and H53.2 becomes secondary or is dropped.