ICD-10 Code M32.9: Systemic lupus erythematosus, unspecified
M32.9 codes SLE when the notes name no organ involvement. Treat it as the fallba...
Last Updated: August 3, 2026
ICD-10 code H35.89 is a billable 2026 ICD-10-CM diagnosis code for other specified retinal disorders not captured by a more specific H35 code
H35.89 sits under category H35 (Other retinal disorders), subcategory H35.8, alongside sibling codes H35.81 (retinal edema) and H35.82 (retinal ischemia)
Use H35.89 only when the retinal condition is documented but does not fit any more specific code; documentation must name the specific disorder to avoid claim denial
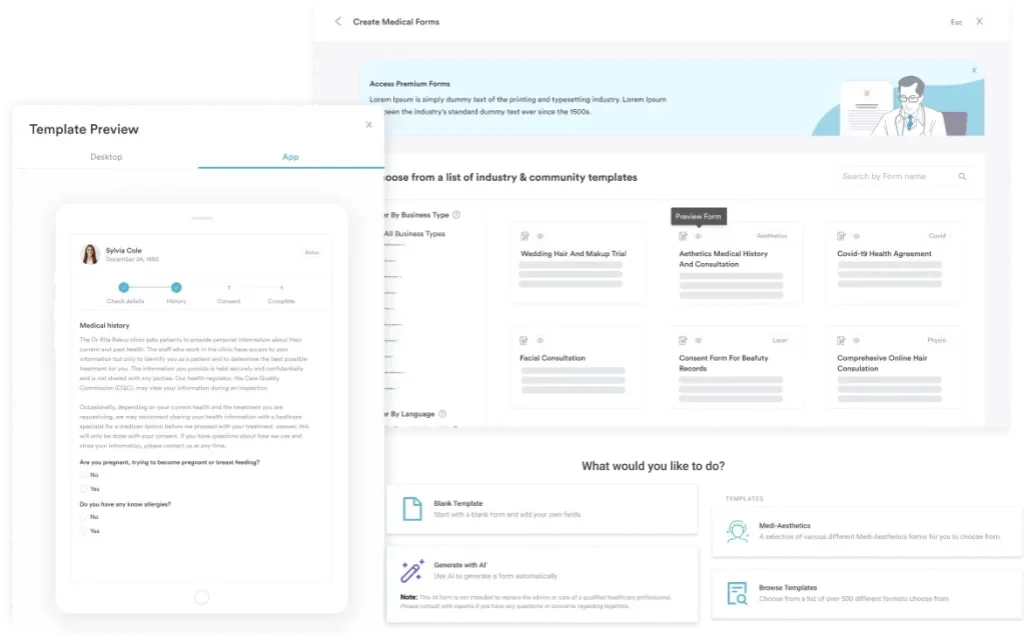
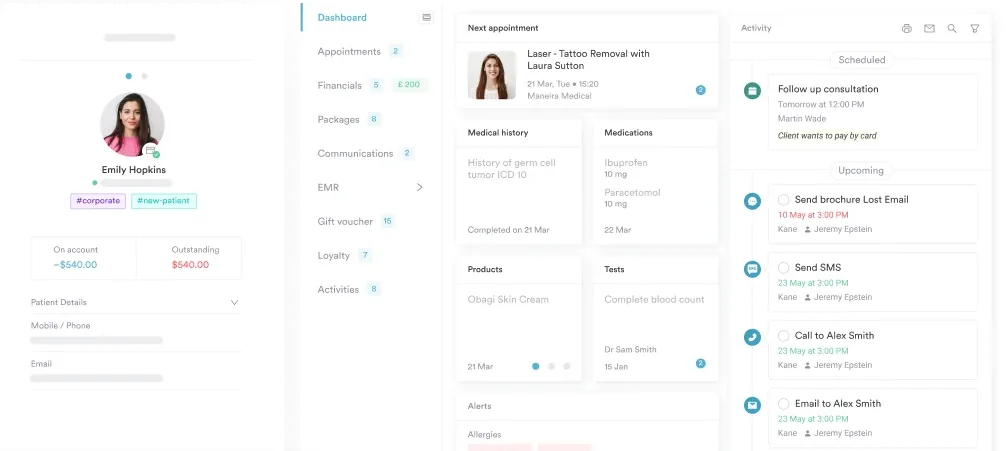
Pabau’s claims management software and digital forms help ophthalmology and optometry practices capture the diagnosis documentation needed to support H35.89 at audit
Ophthalmology coders encounter H35.89 when a patient presents with a retinal condition that is clinically documented but does not match any of the more specific codes within the H35 category. Payers scrutinize “other specified” codes more closely than specific ones, and a vague or incomplete diagnosis note is the fastest route to a denial.
This reference guide covers what ICD-10 code H35.89 represents, how it fits into the retinal disorder hierarchy, which conditions it captures, how it compares to H35.9, and what documentation coders and clinicians need to support the code at billing. It also includes the ICD-9-CM crosswalk and the adjacent codes most relevant to ophthalmology and optometry practice.
ICD-10 code H35.89 is the billable ICD-10-CM diagnosis code for other specified retinal disorders. It is valid for the 2026 ICD-10-CM code year and may be used to indicate a diagnosis for reimbursement purposes wherever payer and CMS guidelines permit.
The CMS (Centers for Medicare and Medicaid Services) and the National Center for Health Statistics (NCHS) maintain the ICD-10-CM tabular list under which H35.89 is classified.
The official code description is: Other specified retinal disorders. The phrase “other specified” is the key clinical signal. It tells the payer that the clinician has identified a definite retinal condition, that it is not unspecified, and that it simply does not have its own dedicated code in the ICD-10-CM system.
Coders working within ophthalmology practices should note that H35.89 is a leaf-level code. There are no more specific subcodes beneath it. Assign H35.89 directly when the condition falls here. The same hierarchy logic applies elsewhere in the H30-H36 block, including H31.9 and the other specified disorders of choroid (H31.8), so always reference the current-year tabular before billing.
H35.89 is a billable and specific ICD-10-CM code. Confirmed across multiple authoritative sources including the CDC/NCHS ICD-10-CM web tool and the AAPC Codify platform, it carries no non-billable parent-only restriction. Practices may submit it on a claim for the 2026 code year.
Being billable does not guarantee reimbursement. Payers evaluate medical necessity independently. Because H35.89 is an “other specified” code rather than a highly specific one, supporting documentation needs to carry more weight, not less. The physician’s note must name the condition and establish why it does not fit a more granular retinal code.
Practices using claims management software can flag H35.89 encounters for documentation review before submission, reducing the risk of payer queries downstream.
H35.89 serves as the coding home for retinal disorders that are genuinely diagnosed but sit outside the existing named codes within H35. Several conditions frequently land here.
This list is not exhaustive. If the clinician documents a retinal finding by name and that name does not correspond to an existing specific code, H35.89 is the appropriate assignment. The key is specificity in the clinical note, not specificity of the code.
A myelinated nerve fiber layer is one of the conditions coders most often assign to H35.89. Myelinated retinal nerve fibers show up as white, feathered patches along the retinal nerve fiber layer, usually spotted incidentally on a dilated fundus exam or optical coherence tomography (OCT).
They are typically benign and non-progressive, and they have no dedicated ICD-10-CM code of their own.
Because the finding is named but not separately classified, H35.89 is the correct assignment once the note records “myelinated nerve fiber layer” or “myelinated retinal nerve fibers.” Document the affected eye and the exam or imaging basis so the diagnosis holds up if the claim is reviewed.
For practices that see a volume of complex retinal cases, building structured encounter templates into your digital forms workflow ensures the retinal finding is named consistently across visits, which supports both coding accuracy and continuity of care.
Before assigning H35.89, run a quick check against H35.81 (retinal edema) and H35.82 (retinal ischemia). If the condition fits either of those sibling codes precisely, use the more specific one. Payers and audit tools flag unnecessary use of ‘other specified’ codes when a specific sibling code was available.
This is one of the most common questions in ophthalmology coding. The difference is clinically and financially significant.
CMS ICD-10-CM Official Guidelines instruct coders to assign the most specific code supported by the documentation. H35.9 (unspecified retinal disorder) is appropriate only when a definitive retinal diagnosis has genuinely not been established. If a clinician writes “retinal nerve fiber bundle defect” in the note, H35.89 is the correct code, not H35.9.
The same specificity-first principle governs other eye codes, including H51.9, where an unspecified code is a last resort rather than a default.
Consistent application of this distinction across your practice improves claim acceptance rates and reduces the audit exposure that comes with repeat use of unspecified codes. Practices managing high-volume ophthalmology billing can track code-level denial patterns through reporting and analytics to identify where H35.9 is being used instead of H35.89.
Pabau helps eye care practices manage clinical records, digital intake forms, and claims workflows in one place, so your coding team has the documentation it needs before a claim goes out the door.

Understanding where H35.89 sits relative to its siblings and neighbors helps coders apply the correct code the first time. The H35 category contains many more specific codes that should always be ruled out before landing on H35.89.
The H36 category is particularly important. When a retinal disorder is a manifestation of diabetes, sickle cell disease, or another systemic condition, the retinal code from H36 should be assigned alongside or in place of H35.89, depending on the sequencing rules.
This mirrors the sequencing logic behind other manifestation codes, such as E35 and H82.9, where the underlying disease code must be listed before the manifestation code on a claim. Always check whether the retinal finding has a primary cause that owns a more specific code.
Isolated fluid or bleeding findings usually point away from H35.89 rather than toward it. Subretinal fluid, for example, is more often captured by a retinal detachment code (H33) or central serous chorioretinopathy (H35.71), and retinal hemorrhage carries its own code (H35.6). Rule these more specific options out before landing on H35.89.
Practices that still reference legacy records or handle older payer audits may need the ICD-9-CM equivalents for H35.89. The conversion is approximate, not exact. Three ICD-9-CM codes map to H35.89.
The three-to-one mapping reflects ICD-10-CM’s increased granularity. For coding verification and crosswalk lookups, the AAPC Codify ICD-10-CM tool and the official CDC/NCHS ICD-10-CM web tool both support forward and backward crosswalk searches for H35.89.
When transitioning older records for historical audits, practices should document that the crosswalk is approximate. The ICD-9-CM codes did not carry identical clinical scope to H35.89, and a direct one-to-one mapping does not exist. The same crosswalk caution applies to other ophthalmic codes, such as H43.9, when reviewing legacy records.
Always treat ICD-9 to ICD-10 crosswalks as approximate. If an older claim is being audited and the ICD-9 code was 362.82 (retinal exudates and deposits), H35.89 is a reasonable forward crosswalk, but the original clinical note still governs the correct modern code assignment.
Payers reviewing claims with H35.89 look for one thing above all: proof that the clinician identified a specific retinal condition. The word “specified” in the code description is a contract with the payer. If the documentation cannot name what the condition is, the code does not hold up.
Practices can structure their ophthalmology encounter templates to capture these elements routinely. Pabau’s client record and digital forms tools allow practices to build condition-specific documentation prompts directly into the encounter workflow, so the billing team receives the named diagnosis, laterality, and clinical basis in every retinal encounter note rather than having to chase the clinician after the fact.
H35.89 is not universally covered across payers, and prior authorization requirements vary by plan. Some insurers treat “other specified” retinal codes as requiring additional clinical context before approving procedures billed alongside them, such as retinal imaging or intravitreal injections. Coders should verify the payer’s medical necessity criteria for the associated procedure code before submission, not just for H35.89 in isolation.
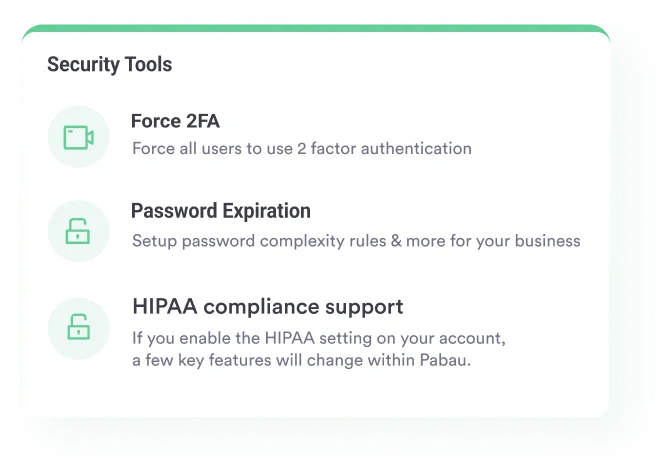
Practices using compliance management software can document payer-specific rules at the code level, flagging H35.89 encounters for pre-authorization checks where required.
Accurate use of ICD-10 code H35.89 is not just a coding exercise. It affects claim acceptance, audit readiness, and the clinical record’s usefulness for ongoing patient management. Three workflow points matter most.
The World Health Organization‘s ICD classification framework underpins all ICD-10-CM coding. Understanding where H35.89 sits within that framework, and why the “other specified” designation exists, helps clinicians and coders treat code selection as a clinical decision rather than a billing task.
The automated workflows built into practice management platforms can support this by routing retinal encounters through a documentation checklist before the claim is finalized.
Multi-specialty groups that manage eye care alongside services such as primary care or sports medicine benefit most from a single system that keeps retinal documentation standards consistent across every department.
A centralized AI-powered clinical documentation tool can assist in structuring retinal findings from dictated notes into structured encounter records, reducing the gap between what the clinician said and what the coder needs to see.
ICD-10 code H35.89 fills a genuine clinical need: a billable code for retinal disorders that are real, documented, and specific in the clinician’s mind, but that sit outside the named entries in the H35 category. Used correctly, it reflects high-quality diagnostic practice. Misused as a shortcut for vague or incomplete documentation, it becomes a denial risk and an audit flag.
Practices that invest in structured documentation workflows, whether through encounter templates, digital forms, or AI-assisted note tools, produce the clinical specificity that makes H35.89 defensible. Pabau’s claims management and client record features support that workflow for ophthalmology and optometry teams. To see how the platform handles complex retinal encounter documentation end to end, book a demo with the Pabau team.
Need to see the ‘other specified vs. unspecified’ coding decision applied to a different eye condition? H40.9 walks through the same specificity question for glaucoma.
Looking for practical guidance on keeping clinical records audit-ready? Medical forms at your healthcare practice covers how structured forms support documentation completeness and compliance.
Want to understand how EHR integration supports coding accuracy across specialties? EHR integration explains how connected systems reduce the gap between clinical findings and claim submission.
ICD-10 code H35.89 is used for other specified retinal disorders, meaning a retinal condition that a clinician has identified and named but that does not have its own dedicated code within the ICD-10-CM H35 category. Common examples include retinal exudates and deposits, retinal nerve fiber bundle defects, solar retinopathy, and crystalline retinopathy from drug deposition.
Yes, H35.89 is a billable and specific ICD-10-CM code valid for the 2026 code year. It may be submitted on a claim to indicate a diagnosis for reimbursement purposes, subject to payer medical necessity criteria and adequate supporting documentation.
H35.89 means the clinician has identified a specific retinal condition that lacks its own dedicated code. H35.9 means the nature of the retinal disorder is genuinely unknown or undetermined. When a diagnosis is named in the clinical note, H35.89 is the correct choice; H35.9 should be used only when no diagnosis has been established at all.
Three ICD-9-CM codes approximate H35.89: 362.82 (retinal exudates and deposits), 362.85 (retinal nerve fiber bundle defects), and 362.89 (other retinal disorders). All crosswalks are approximate; the original clinical documentation governs the appropriate modern code assignment.
The clinical note must name the specific retinal condition (not just “retinal finding”), record which eye or eyes are affected, identify the clinical or imaging basis for the diagnosis (fundus photo, OCT, fluorescein angiogram), and ideally note why more specific codes such as H35.81 or H35.82 did not apply. This documentation is what a payer reviews when scrutinizing an “other specified” code claim.
Retinal disorders coded under H35.89 include retinal exudates and deposits, retinal nerve fiber bundle defects, solar retinopathy, crystalline retinopathy from drug deposition (such as tamoxifen), paracentral acute middle maculopathy, and other named but non-specifically coded retinal conditions documented by an ophthalmologist or optometrist.
The ICD-10 code for a myelinated nerve fiber layer is H35.89, other specified retinal disorders. Myelinated retinal nerve fibers are a named finding with no dedicated code of their own, so H35.89 applies once the clinician documents them by name and records the affected eye.
Usually not. Subretinal fluid is more often coded to a retinal detachment (H33) or central serous chorioretinopathy (H35.71), depending on the cause. H35.89 fits only when a documented retinal disorder has no more specific code, so rule those options out first.