ICD-10 Code M36.0: Dermatomyositis in neoplastic disease
ICD-10 Code M36.0 is the billable, specific ICD-10-CM code for dermatomyositis i...
July 24, 2026
ICD-10 code H16.8 (Other keratitis) is a billable, specific diagnosis code valid for reimbursement claims for dates of service on or after October 1, 2015.
H16.8 applies when keratitis does not fit a more specific H16 subcode, covering conditions such as sclerokeratitis, autoimmune keratitis, bacterial keratitis, and fungal keratitis without a more precise classification.
H16.8 and H16.9 are frequently confused: H16.8 applies when a defined but non-categorized type of keratitis is documented; H16.9 is reserved for keratitis with no further clinical specification.
Pabau’s claims management software supports accurate ICD-10 coding workflows for ophthalmology and optometry practices, reducing coding errors and claim denials.
ICD-10 code H16.8 (Other keratitis) covers keratitis presentations that a clinician has specifically identified but that do not fit any of the more specific subcategories under H16.
According to the Centers for Medicare and Medicaid Services (CMS), ICD-10-CM codes are required for all reimbursement claims with a date of service on or after October 1, 2015. H16.8 is classified under the chapter H15-H22 (Disorders of sclera, cornea, iris and ciliary body), maintained in the United States by the National Center for Health Statistics (NCHS) and CMS.
H16.8 is a billable, specific ICD-10-CM diagnosis code. It can be used directly on insurance claims and does not require a higher-specificity child code. This distinguishes it from parent codes such as H16 (Keratitis) or the broader H15-H22 chapter header, which are non-billable header codes that exist only for classification purposes.
Ophthalmology and optometry practices using claims management software should confirm that H16.8 appears in their code set for the relevant date of service and is mapped correctly to the encounter diagnosis before submission.
The defining clinical characteristic of H16.8 is that it covers keratitis types that are specifically identified by the clinician but do not correspond to any of the dedicated H16 subcategories. Based on official ICD-10-CM inclusion notes and coding references, the following conditions are commonly coded to H16.8:
| Condition | Clinical notes |
|---|---|
| Sclerokeratitis | Inflammation involving both the sclera and cornea; does not fit H16.0-H16.4 specifically |
| Autoimmune keratitis | Immune-mediated corneal inflammation without a defined systemic category |
| Bacterial keratitis (non-ulcerative) | Bacterial corneal inflammation, commonly from Pseudomonas or Staphylococcus, that does not constitute a corneal ulcer (H16.0) |
| Fungal keratitis (organism unspecified) | Mycotic corneal inflammation reported as H16.8 with an additional B35-B49 code identifying the organism, when known |
| Autosomal dominant keratitis | Hereditary keratitis not specified under interstitial or deep subtypes |
| Bilateral keratitis (non-specified type) | When bilateral presentation does not align with a more specific bilateral H16 subcode |
Fungal (mycotic) keratitis doesn’t have its own H16 subcode, so it’s reported as H16.8. Because H16.8 only identifies the corneal manifestation, coders add a secondary code from the B35-B49 mycoses range to identify the causative organism: B49 (Unspecified mycosis) when the specific fungus isn’t documented, or a more precise code from that range when it is (for example, a named Candida or Aspergillus species).
Chemical and toxic keratitis are handled differently and don’t code to H16.8 at all. A keratitis presentation caused by a chemical burn falls under the T26 (burn and corrosion of eye) codes, since ICD-10-CM classifies chemical exposure as an injury rather than a diagnosed keratitis type. Toxic keratitis from UV exposure, such as welder’s keratitis, is coded as photokeratitis under H16.1, not H16.8.
Clinicians should review inclusion notes in the current ICD-10-CM tabular list to confirm a condition qualifies for H16.8 before coding. The CDC/NCHS ICD-10-CM web tool provides the authoritative tabular list and inclusion notes for the current fiscal year.
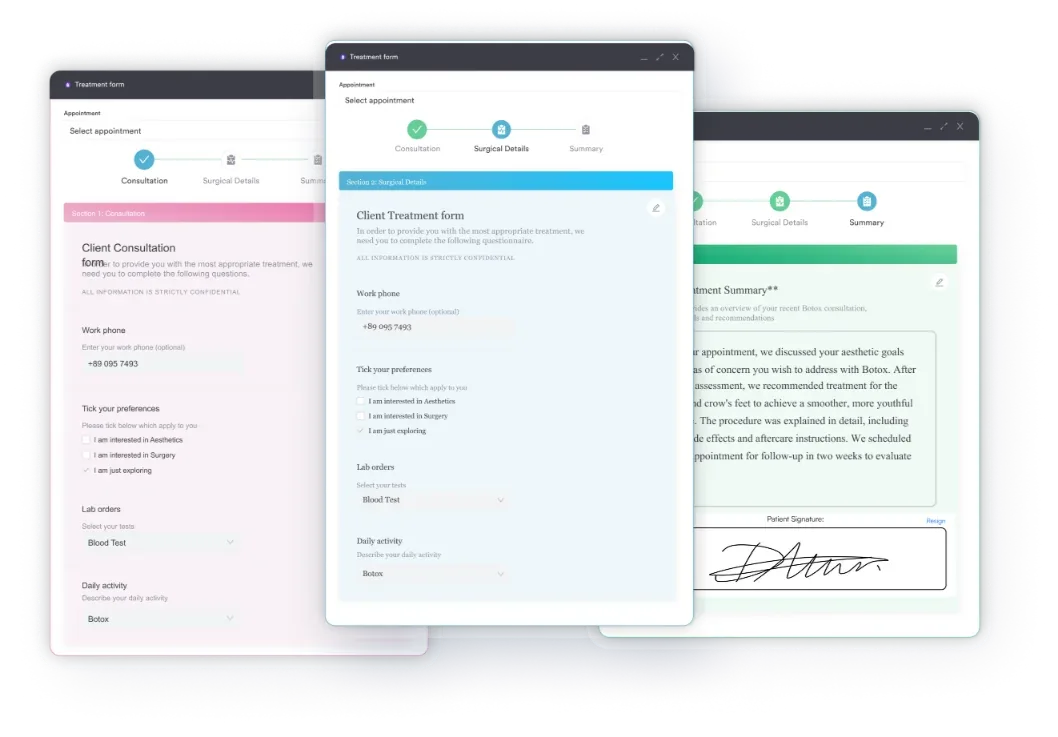
Accurate documentation of the specific type of keratitis in the clinical note is essential, as it is the foundation for selecting H16.8 over H16.9 (unspecified keratitis). Practices can simplify this step using digital intake and clinical documentation forms that prompt for diagnosis specificity at the point of care.
Selecting the correct code within the H16 family is a frequent source of ophthalmology coding errors. The difference between H16.8 and its neighboring codes matters for reimbursement accuracy and audit defensibility.
H16.9 (Unspecified keratitis) applies when the clinical record contains no further detail about the type of keratitis. H16.8 requires that a specific type of keratitis has been identified and documented, but that type does not correspond to H16.0 through H16.4.
In practice, this means H16.8 should only be used when the clinician has named the keratitis type in the record. If the note simply states “keratitis” without further description, H16.9 is more appropriate.
Documenting the corneal findings in detail, including onset, suspected etiology, and laterality, supports the use of H16.8 and reduces the risk of a claim denial on specificity grounds.
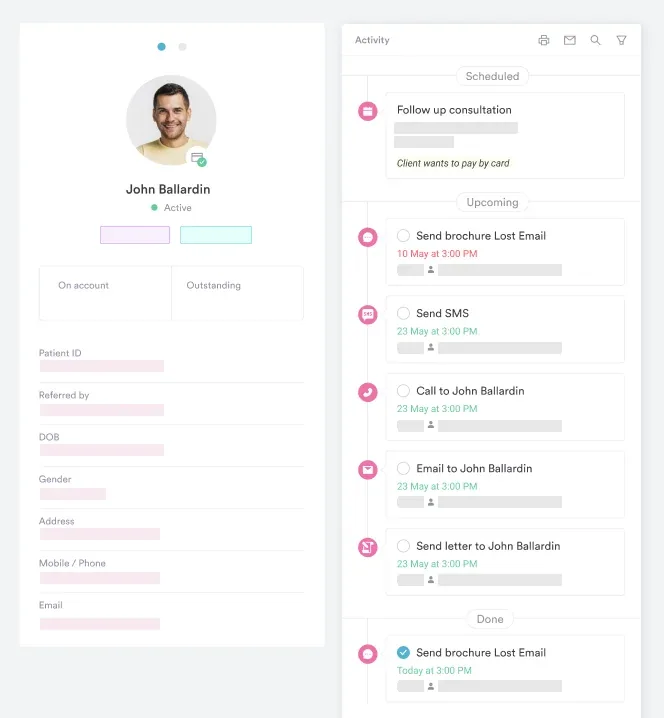
Maintaining structured electronic patient records makes this documentation step easier to standardize across a practice.
Before defaulting to H16.8, coders and clinicians should rule out the more specific subcategories:
If the clinical presentation matches any of the above, use the more specific code. H16.8 is a residual category and should not be a first-choice code when a more precise option exists. Good coding practice, supported by well-structured clinical documentation workflows, ensures that the coding team has enough information to make the right selection every time.
Review your H16.8 claim volume quarterly. A high proportion of H16.8 codes relative to the more specific H16.1-H16.4 subcodes may indicate that clinicians are under-documenting keratitis type in their encounter notes. An internal audit of five to ten records can quickly reveal whether documentation prompts need to be added to your intake or consultation template.
For inpatient hospital billing, ICD-10-CM diagnosis codes are grouped into Medicare Severity Diagnosis Related Groups (MS-DRGs) to determine reimbursement. H16.8 maps to the following groupings under MS-DRG v43.0:
| MS-DRG | Description | Condition |
|---|---|---|
| 124 | Other disorders of the eye with MCC or thrombolytic agent | When a major complication or comorbidity is present |
| 125 | Other disorders of the eye without MCC | When no major complication or comorbidity is present |
H16.8 keratitis presentations rarely result in inpatient admission, so these DRG groupings are less commonly triggered in typical ophthalmology or optometry billing. They are most relevant for hospital-based ophthalmologists managing complicated keratitis cases. Verify DRG groupings against current CMS IPPS tables annually, as grouper versions update each fiscal year.
The CMS ICD-10 codes page publishes updated grouper files each October. Practices managing complex eye cases should review how their EHR integrations handle DRG-relevant comorbidity documentation to ensure the record supports the appropriate grouping.
Pabau gives ophthalmology and optometry practices structured clinical documentation, digital forms, and integrated claims workflows that support accurate ICD-10 coding from the point of care through to submission.

Payers and auditors expect the clinical record to support the specificity of any diagnosis code submitted. For H16.8, the documentation must justify that the keratitis type was identified but does not match a more specific H16 subcode. The following elements should appear in the encounter note:
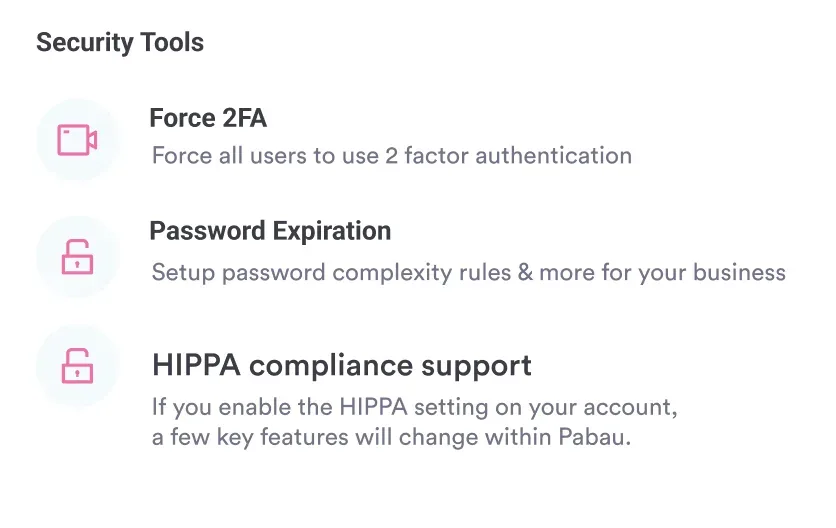
Maintaining these documentation standards is straightforward when practices use structured clinical documentation software tied to their diagnosis workflow. Compliance-focused practices can layer this into a broader compliance management workflow to ensure documentation standards are met consistently across all clinicians.
Accurate ICD-10 coding depends on both the clinician and the coder: the clinician documents the diagnosis, and the coder or biller translates it into the correct code. Breakdowns happen when documentation is vague or when coding staff are not regularly updated on specificity requirements. For H16.8, the following workflow steps reduce error rates:
Practices managing a high volume of ophthalmology encounters benefit from linking their coding workflow to their broader practice management system, so documentation and code selection stay consistent across the team.
The AAPC Codify ICD-10-CM lookup is a useful supplementary reference for verifying code descriptions and inclusion notes before submission.
Set up a diagnosis-specific documentation prompt in your clinical note template for keratitis encounters. The prompt should ask the clinician to specify type, laterality, etiology, and whether corneal ulceration or conjunctival involvement is present. This single addition to your template can significantly reduce the proportion of H16.9 (unspecified) codes and improve coding specificity across the practice.
H16.8 sits within a broader family of corneal and ocular surface codes, such as H17.9 for unspecified corneal scar and opacity. Coders working in ophthalmology should be familiar with the adjacent codes to avoid misclassification.
| ICD-10 code | Description | Key distinction from H16.8 |
|---|---|---|
| H16.0 | Corneal ulcer | Keratitis with epithelial defect or ulceration |
| H16.1 | Other superficial keratitis without conjunctivitis | Superficial types including photokeratitis, filamentary, punctate keratitis |
| H16.2 | Keratoconjunctivitis | Keratitis with conjunctival involvement |
| H16.3 | Interstitial and deep keratitis | Stromal and disciform presentations, including herpes-associated |
| H16.4 | Corneal neovascularization | Primary finding is corneal vascularization |
| H16.8 | Other keratitis | Identified type not captured by H16.0-H16.4 |
| H16.9 | Unspecified keratitis | No further clinical specification in the record |
| H18.6 | Keratoconus | Structural corneal condition, not inflammatory |
Note that H18.6 (Keratoconus) is a non-billable header code requiring a more specific child code (H18.60, H18.601, etc.). It is included here because keratoconus can present with corneal inflammation and is occasionally confused with keratitis at the coding stage.
Practices that handle a range of corneal diagnoses should align their procedure code workflows with accurate ICD-10 diagnosis coding.
H16.8 is a legitimate, billable code, but it is a residual category. Using it correctly means confirming that a specific keratitis type has been documented and that no more precise H16 subcode applies — the kind of detail auditors review.
Practices that build this discipline into their documentation workflow, rather than leaving it to code selection at submission, see better claim acceptance rates.
Pabau’s integrated clinical documentation and claims management tools help ophthalmology and optometry practices capture the right diagnostic detail at every encounter. To see how Pabau supports accurate ICD-10 coding workflows for eye care practices, book a demo.
Vision correction billing: HCPCS code V2103 for single-vision lenses walks through optical billing for optometry practices.
Point-of-care exam form: the PERRLA eye exam form template standardizes pupil and ocular documentation.
Chronic eye monitoring: the diabetes eye exam template supports structured vision assessments.
Oculoplastic documentation: the eyelid surgery (blepharoplasty) template covers surgical eye-care records.
Office visit coding: CPT code 99202 for new-patient office visits is often paired with an eye examination.
Inflammatory diagnosis coding: ICD-10 code M31.9 (necrotizing vasculopathy) is another documentation-driven, non-specific inflammatory code.
Billing fundamentals: what is medical billing breaks down the full claim lifecycle.
Software comparison: best medical billing software in the US compares platforms for claim accuracy.
Automating notes: AI clinical documentation explains how automated scribing improves diagnosis specificity.
Full documentation workflow: the ICD-10 renal mass coding guide demonstrates end-to-end clinical documentation.
ICD-10 code H16.8 is a billable diagnosis code for “Other keratitis,” covering corneal inflammation conditions that are specifically identified by the clinician but do not correspond to the more precise subcategories H16.0 through H16.4. It is classified under H15-H22 (Disorders of sclera, cornea, iris and ciliary body) and is valid for claims with dates of service from October 1, 2015.
Yes. H16.8 is a billable, specific ICD-10-CM diagnosis code that can be used directly on insurance claims without requiring a more specific child code. It is confirmed as valid and active for fiscal year 2026.
Conditions coded to H16.8 include sclerokeratitis, autoimmune keratitis, non-ulcerative bacterial keratitis, autosomal dominant keratitis, and bilateral keratitis presentations that do not align with a more specific H16 subcode. The key requirement is that the clinician has identified a specific type of keratitis that falls outside H16.0-H16.4.
H16.8 applies when a specific type of keratitis has been identified and documented but does not fit H16.0-H16.4. H16.9 (Unspecified keratitis) applies when the clinical record contains no further detail about the type. If the clinician has named the keratitis type, use H16.8. If the note simply states “keratitis” with no further description, use H16.9.
Under MS-DRG v43.0, H16.8 groups to DRG 124 (Other disorders of the eye with MCC or thrombolytic agent) when a major complication or comorbidity is present, and DRG 125 (Other disorders of the eye without MCC) when none is present. Verify current groupings annually against CMS IPPS tables, as grouper versions update each fiscal year.
Yes. Fungal (mycotic) keratitis is reported as H16.8 because there’s no dedicated fungal subcode under H16. Add a secondary code from the B35-B49 mycosis range alongside it — typically B49 (Unspecified mycosis) when the organism isn’t identified in the record, or a more specific code when it is.
No. A chemical burn to the cornea is coded under the T26 burn and corrosion range, since ICD-10-CM treats chemical exposure as an injury rather than a diagnosed keratitis type. Toxic keratitis caused by UV exposure, such as welder’s keratitis, is coded as photokeratitis under H16.1.
There’s no single code for keratitis. ICD-10-CM splits it by type under H16: H16.0 for corneal ulcer, H16.1 for superficial keratitis without conjunctivitis, H16.2 for keratoconjunctivitis, H16.3 for interstitial and deep keratitis, H16.4 for corneal neovascularization, H16.8 for other identified types, and H16.9 for unspecified keratitis.