What is concierge medicine? A guide for practice owners
Concierge medicine swaps a 2,000-patient panel for 300-600 on retainer, typicall...
Last Updated: July 31, 2026
Medical billing converts clinical care into payer claims
Coding accuracy is the leading driver of denials
Clearinghouses validate claims before payer submission
The cycle spans registration through payment posting
Integrated software reduces error rates and accelerates reimbursement
A single coding error can delay reimbursement for weeks or push a claim into the denial pile that costs roughly $25 in staff time to rework. The problem is widespread: ACA marketplace insurers denied an average of 17% of in-network claims in 2021, according to a KFF analysis, tying up cash flow and pulling clinical staff into appeals work.
Medical billing is the workflow that turns patient encounters into paid claims, and it is where most preventable revenue leakage happens. Get registration, coding, scrubbing, and follow-up right and payment lands within 30 days. Miss any of them and the entire cycle stalls.
Medical billing encompasses all activities that generate revenue from clinical services. It starts when a patient schedules an appointment and ends when the clinic receives full payment. According to the American Academy of Professional Coders, billing professionals review patient medical records, identify appropriate diagnosis and procedure codes, and submit claims to payers using standardised forms.
The scope includes insurance verification, charge capture, claim submission, payment posting, denial management, and patient billing for outstanding balances. For private healthcare practices in the UK, this extends to processing claims through private medical insurance providers using CCSD codes. In the US, practices navigate Medicare, Medicaid, and commercial insurance requirements. Regardless of geography, the core function remains constant: ensuring providers receive payment for services rendered.
Billing differs from medical coding. Coders assign CPT, ICD-10, and HCPCS codes based on clinical documentation. Billers use those codes to prepare and submit claims. Many small practices combine these roles, but the skill sets diverge. Coders need deep clinical knowledge to interpret medical records. Billers focus on payer rules, claim formats, and reimbursement workflows.
The billing cycle follows a predictable sequence. Understanding each stage helps practices identify where delays or errors occur.

Before the appointment, staff collect demographic and insurance information. They verify coverage with the payer to confirm the patient’s plan is active and the provider is in-network. This prevents surprise denials after service delivery. Practices check benefits, deductibles, co-pays, and prior authorisation requirements at this stage.
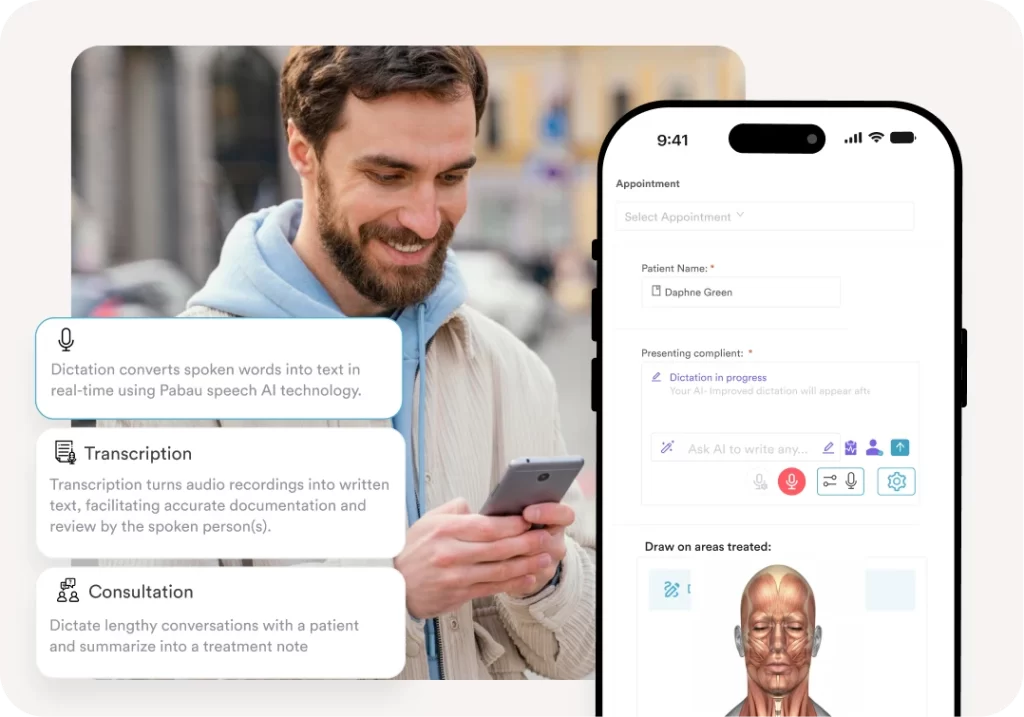
During the visit, clinicians document diagnoses, treatments, and procedures in the patient’s medical record. This documentation must support the codes billed. Incomplete or vague notes lead to downcoding (billing a lower-level service than performed) or outright denials. Many clinics now use AI-powered clinical documentation tools to streamline this step and improve accuracy.
Coders translate the clinical notes into standardised codes. CPT codes describe procedures and services. ICD-10-CM codes identify diagnoses. HCPCS codes cover supplies, equipment, and non-physician services. The codes must align-the diagnosis codes should justify why each procedure was medically necessary. Coding errors are the leading cause of claim denials.
Only assign codes that the documentation explicitly supports. If a clinical note says “patient presents with knee pain” but does not record exam findings, history, or duration, billing a higher-level evaluation code invites audit scrutiny. Build a short clinician checklist (chief complaint, history, exam, assessment, plan) and tie EHR templates to it. Documentation drives the code, never the reverse.
Billers compile the patient’s demographic data, insurance details, and codes into a claim. Most practices use electronic health record (EHR) systems that generate claims automatically. Before submission, claims pass through scrubbing software that checks for common errors: missing modifiers, incorrect patient identifiers, invalid code combinations. Clean claims have a higher first-pass acceptance rate.
Claims go to a clearinghouse-an intermediary that validates the format and routes the claim to the correct payer. Clearinghouses flag errors before the claim reaches the insurance company, allowing practices to fix issues quickly. Direct submission to payers is possible but slower. Most US practices use clearinghouses for Medicare, Medicaid, and commercial claims. UK private healthcare practices submit private medical insurance claims primarily through Healthcode, the UK’s dominant medical billing platform that connects clinics to insurers including Bupa, AXA Health, Vitality, and Aviva, alongside direct submission via insurer-specific portals.
The payer reviews the claim to determine payment eligibility. They check whether the service is covered under the patient’s plan, the diagnosis supports medical necessity, and the provider is authorised. Adjudication can take 7-30 days. The payer then approves payment, requests more information, or denies the claim. Approved claims generate an Explanation of Benefits (EOB) detailing what the payer will pay and what the patient owes.
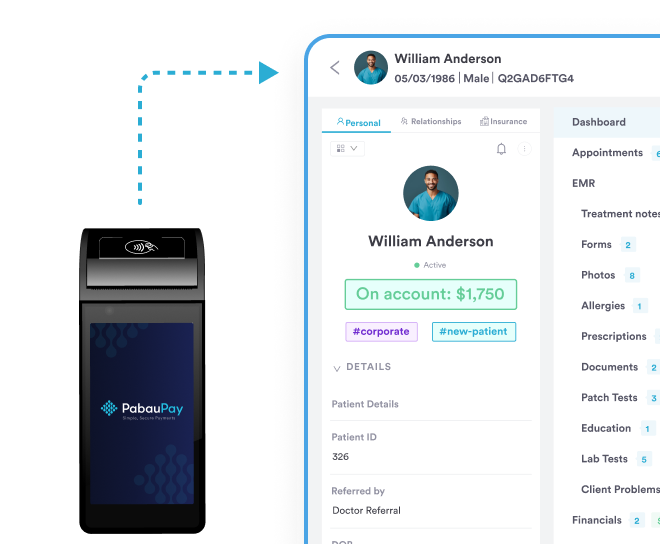
When payment arrives, staff post it to the patient’s account. They allocate the payment across billed services and update the account balance. If the patient has a remaining balance-due to deductibles, co-insurance, or non-covered services-the practice generates a patient statement. Integrated payment processing systems simplify collection by allowing patients to pay online or via mobile app.
Denied claims require investigation. Staff identify the denial reason, gather supporting documentation, and resubmit or appeal. Common denial causes include incorrect patient information, missing prior authorisation, or coding mismatches. Practices that track denial patterns can implement upstream fixes-training staff on frequent errors or updating EHR workflows to prevent repeat issues.
Track denial reasons by payer in a simple spreadsheet or RCM dashboard. Patterns emerge quickly: one payer may consistently reject claims for missing modifier 25, another for prior-authorization gaps on imaging. Fix the root cause once and you eliminate dozens of future denials, instead of chasing each one individually.
Automate claims management, track payments in real-time, and reduce administrative burden with an all-in-one practice management platform.

Billing and coding are distinct but interdependent. Coders work directly from clinical documentation. They assign diagnosis codes (ICD-10-CM), procedure codes (CPT, HCPCS), and modifiers that clarify circumstances. Their work requires clinical knowledge-understanding anatomy, disease processes, and treatment protocols. A coder must know the difference between excision and debridement, or how to classify a complex versus simple laceration repair.
Billers take the coded claim and manage the financial side. They verify insurance, submit claims, follow up with payers, post payments, and bill patients. Billing requires operational expertise: payer policies, reimbursement timelines, appeals processes, and patient communication. While coders need clinical literacy, billers need financial fluency.
In solo practices or small clinics, one person often handles both. Larger organisations separate the roles. Some outsource coding to specialists while keeping billing in-house, or vice versa. The rise of claims management software has blurred these lines-systems now auto-suggest codes based on clinical notes and submit claims with minimal manual intervention.
Medical billing has its own vocabulary. Misunderstanding these terms causes confusion during payer conversations or when troubleshooting claim issues.
Superbill: A detailed receipt of services provided during a patient visit, listing all procedures, diagnoses, and charges. Practices that bill patients directly often hand out superbills for insurance reimbursement.
Clean claim: A claim submitted with no errors or missing information, processed on first submission without rework.
Remittance advice: A document from the payer explaining how a claim was processed, including paid amounts, adjustments, and denial reasons.
Aging report: A financial report showing outstanding patient balances by age (30, 60, 90 days overdue). Practices use this to prioritise collection efforts.
Write-off: An amount the practice removes from a patient’s account, either as a contractual adjustment (difference between billed charge and payer-allowed amount) or bad debt (uncollectible balance).
Coordination of benefits: The process of determining which insurance plan pays first when a patient has multiple policies. The primary plan processes the claim, then the secondary plan covers remaining balances per its terms.
Track your clean claim rate monthly. Industry benchmarks suggest 90-95% of claims should be clean on first submission. If your rate falls below 90%, audit your coding and documentation workflows to identify recurring errors.
Medical billing software has evolved from standalone systems to integrated platforms. Modern solutions connect clinical documentation, coding, claim submission, and payment processing in a single workflow.
Key features include automated insurance verification, real-time eligibility checks, electronic claim submission, denial tracking, payment posting, and financial reporting. Advanced systems use artificial intelligence to suggest codes based on clinical notes, flag potential denials before submission, and predict patient payment likelihood.
Cloud-based platforms dominate because they allow multi-location access, automatic updates, and seamless integration with clearinghouses and payment processors. For clinics operating internationally, software that supports multiple coding systems (CPT in the US, CCSD in the UK, tarmed in Switzerland) prevents manual code translation.
Security is non-negotiable. Medical billing systems must comply with regional data protection regulations. In the US, HIPAA mandates encryption, access controls, and audit trails. In Europe, GDPR requires patient consent, data portability, and breach notification protocols. UK practices face CQC oversight for data handling. Reputable billing software builds these safeguards into the platform.
Medical billing sits within a larger framework called revenue cycle management (RCM). RCM tracks every financial touchpoint from patient scheduling to final payment collection. It encompasses pre-service activities (appointment scheduling, insurance verification), point-of-service activities (check-in, co-pay collection, clinical documentation), and post-service activities (coding, billing, payment posting, follow-up).
Effective RCM reduces the time between service delivery and payment receipt, known as days in accounts receivable. Industry data suggests private practices average 30-50 days. High-performing clinics bring this below 30 by addressing bottlenecks: slow coding turnaround, delayed claim submission, or inefficient denial resolution.
RCM also measures key performance indicators: claim acceptance rate, denial rate, collection rate (percentage of billed charges actually collected), and bad debt ratio. Practices compare their metrics against specialty benchmarks to identify improvement opportunities. For example, if your denial rate is 12% and the industry average is 6%, your coding or verification process needs attention.
Outsourced RCM services exist for practices that lack in-house billing expertise. These vendors handle end-to-end billing for a percentage of collections (typically 4-8%). The trade-off: less direct control over patient communication and financial reporting. Many private practices prefer in-house billing supported by robust software.
Billing mistakes delay payments and frustrate patients. The most frequent errors are predictable and preventable.
Incorrect patient information: Misspelled names, wrong birth dates, or outdated addresses cause immediate claim rejections. Front-desk staff must verify demographics at every visit, not just new patient registration.
Insurance verification gaps: Failing to confirm coverage before the appointment leads to uncompensated care. Patients assume they’re covered, then receive surprise bills when claims are denied. Real-time eligibility checks during scheduling prevent this.
Upcoding or undercoding: Billing a higher-level service than documented (upcoding) triggers audits and potential fraud accusations. Billing a lower-level service (undercoding) leaves money on the table. Coders must match documentation precisely.
Missing modifiers: Modifiers clarify circumstances like bilateral procedures, discontinued services, or assistant surgeons. Omitting them results in incorrect reimbursement or denials. Practices should maintain a reference guide of commonly used modifiers for their specialty.
Duplicate billing: Submitting the same claim twice-often due to software errors or impatient follow-up-flags the practice as high-risk. Clearinghouses catch most duplicates, but repeat offenders face payer scrutiny.
Late filing: Payers impose submission deadlines that vary widely. Commercial payers typically allow 90-180 days from service date, Medicare allows up to one year (365 days), and some commercial contracts require submission within 30-90 days. Missing the deadline forfeits payment entirely.
The clinics that hit 95% clean-claim rates and collect within 30 days did not get there by working harder. They moved from fragmented spreadsheets and standalone billers to integrated platforms that catch errors before submission, surface denial patterns early, and put payment options in front of patients without staff chasing balances. Automation handles the rote work so your team can focus on the cases that genuinely need a human touch: complex appeals, payer disputes, and patient questions about coverage.
Book a demo with Pabau to see how an integrated practice management platform replaces the patchwork of billing tools most clinics still rely on, and get a clearer picture of where your revenue is currently leaking.
Looking for integrated billing and clinical workflows? Claims Management Software connects patient records, coding, and payer submission in one system.
Need to streamline patient payment collection? Payment Processing supports online payments, deposit management, and automated reminders.
Managing multiple clinic locations? Multi-Location Management centralises billing, reporting, and patient data across sites.
Medical coding translates clinical documentation into standardised diagnosis and procedure codes. Medical billing uses those codes to prepare and submit claims to insurance payers or patients, then tracks payments and manages denials. Coders focus on clinical accuracy; billers focus on financial processing.
From service date to payment receipt, the billing cycle typically takes 30-50 days. Insurance claims require 7-30 days for adjudication. Denied claims can extend the timeline by weeks if appeals are necessary. Practices using automated workflows and clean claim protocols often reduce this to under 30 days.
Verifying insurance before appointments confirms the patient’s coverage is active, the provider is in-network, and the service is covered under their plan. Without verification, practices risk delivering uncompensated care when claims are denied for eligibility issues. Real-time checks during scheduling prevent surprise billing disputes.
The core stages are patient registration and insurance verification, clinical documentation and charge capture, medical coding, claim preparation and scrubbing, submission via clearinghouse, payer adjudication, payment posting, and denial management. Each step requires accuracy to avoid delays.
Medical billers verify insurance eligibility, prepare and submit claims electronically, track claim status with payers, post payments to patient accounts, generate patient statements for outstanding balances, investigate denied claims, and communicate with both payers and patients about billing inquiries. They use practice management software to manage these workflows.
Common challenges include high denial rates due to coding errors, slow reimbursement timelines from payers, patient confusion about billing statements, difficulty tracking prior authorisations, and managing changing payer policies. Practices address these through staff training, automated claim scrubbing, and integrated billing software.