Healthcare content marketing: A strategy guide for practices
Healthcare content marketing works when clinical records and appointment data be...
Last Updated: August 6, 2026
Asthma is a chronic inflammatory disease with reversible airway obstruction that requires systematic NANDA-based nursing assessment and intervention.
The six primary NANDA nursing diagnoses for asthma are Ineffective Airway Clearance, Impaired Gas Exchange, Ineffective Breathing Pattern, Activity Intolerance, Deficient Knowledge, and Anxiety.
Each nursing diagnosis requires specific measurable expected outcomes, evidence-based interventions with clinical rationale, and documented evaluation of goal achievement.
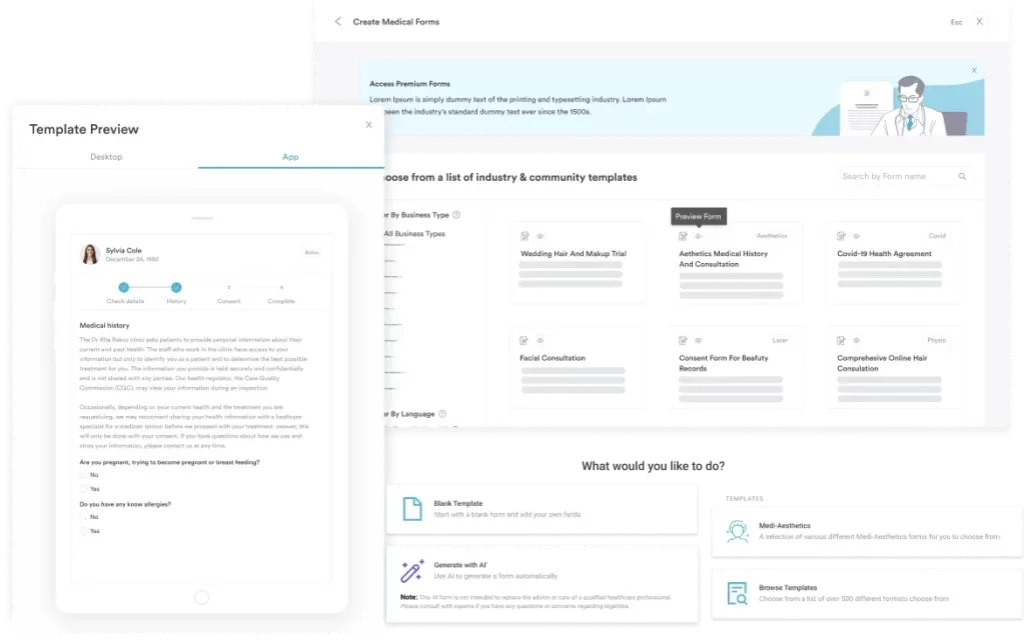
Practice management software like Pabau offers digital forms and clinical documentation features that help nurses structure assessment data, track intervention outcomes, and maintain audit-ready compliance records for asthma care plans.
A ready-to-use clinical framework covering patient assessment, NANDA diagnosis selection, measurable goals, evidence-based nursing interventions with rationale, and structured evaluation for asthma management across adult and pediatric populations.
Download templateAn asthma nursing care plan is a systematic clinical document that guides nurses through evidence-based assessment, accurate NANDA-approved nursing diagnoses, measurable goals, specific interventions with scientific rationale, and documented outcomes evaluation.
This framework ensures consistent, high-quality care for patients across the full spectrum of asthma severity-from stable chronic management to acute exacerbation.
Asthma is a chronic inflammatory airway disease characterized by reversible airway obstruction, bronchial hyperresponsiveness, and inflammation. Nursing care plans respond to this pathophysiology by providing a structured template for assessment and intervention.
A care plan documents the patient’s current respiratory status, identifies actionable nursing diagnoses, establishes measurable outcomes, implements targeted interventions, and evaluates progress toward goals.
The care plan bridges clinical assessment and patient safety by creating an audit trail of decision-making, ensuring compliance with professional nursing standards, and supporting continuity of care across shifts and settings.
For healthcare teams using structured patient records, the care plan becomes the centerpiece of documentation-a legally defensible record that demonstrates evidence-based nursing judgment.
Assessment is the foundation of the care plan. Nurses collect subjective data (patient-reported symptoms, trigger history, medication adherence, anxiety level, knowledge deficits) and objective data (respiratory rate, oxygen saturation, peak flow measurements, breath sound auscultation, accessory muscle use, ability to speak full sentences, presence of cough or wheeze).
This assessment data directly informs nursing diagnosis selection and justifies the interventions that follow. Mental health assessment frameworks also inform anxiety screening, which commonly co-occurs with asthma exacerbation, and an anxiety triggers worksheet can help structure that part of the assessment.
NANDA-I (North American Nursing Diagnosis Association International) provides standardized diagnostic labels that transform assessment findings into actionable nursing problems.
These diagnoses reflect actual or potential health issues that nurses are uniquely qualified to address through independent and collaborative interventions.
Selection of diagnoses depends on assessment findings. Not every asthma patient receives every diagnosis-the nurse prioritizes based on the presenting clinical picture. A comprehensive biopsychosocial assessment can help structure this diagnostic reasoning when anxiety or psychosocial factors complicate the clinical picture.
Each care plan follows a standard table format with columns for nursing diagnosis, related factors and defining characteristics (AEB), expected outcomes (short- and long-term goals), specific nursing interventions with measurable actions, scientific rationale explaining why the intervention works, and evaluation notes documenting goal achievement.
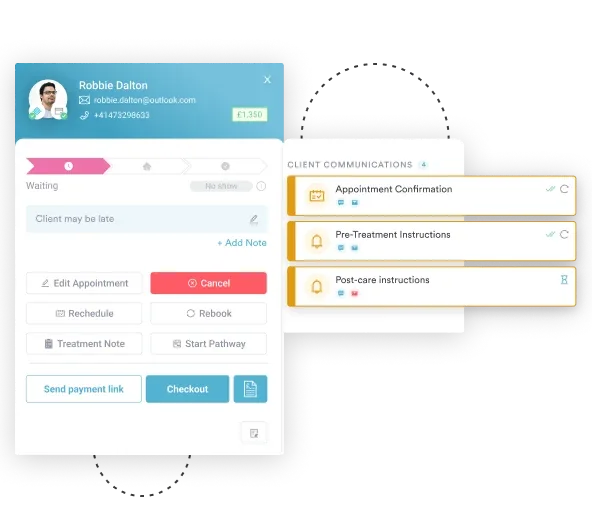
Documentation of each intervention step-including the time, outcome, and patient response-creates the evidence trail that supports clinical decisions and regulatory compliance. Structured digital forms can be configured to prompt for required assessment elements and document interventions in real time.
An acute asthma exacerbation demands immediate prioritization of Ineffective Airway Clearance and Impaired Gas Exchange.
Nursing interventions shift to crisis-level protocols: continuous pulse oximetry monitoring, frequent reassessment (every 15-30 minutes), rapid medication administration, oxygen titration to maintain SpO2 94-98%, positioning to maximize breathing mechanics, and preparation for emergency escalation if respiratory distress worsens.
The exacerbation care plan differs from a maintenance plan by compressing the timeline for goal achievement (hours, not days), increasing monitoring frequency, and including contingency interventions if first-line actions fail. Automated alert workflows can flag critical oxygen saturation thresholds or missing reassessment timestamps, reducing response delays.
Pediatric asthma care plans adapt assessment parameters and interventions for developmental stage. Infants and toddlers cannot report dyspnea verbally, so nurses rely on behavioral cues (irritability, inability to feed, grunting, retractions) and vital signs. School-age children and adolescents participate in self-management education and can learn inhaler technique and trigger avoidance strategies.
Pediatric care plans emphasize caregiver education and family involvement. Goals include teaching parents to:
School nurses benefit from receiving a copy of the care plan to provide consistent monitoring during school hours.
Begin by completing a thorough respiratory and general assessment, documenting all findings in the assessment section. Next, review the NANDA diagnosis list and select the diagnoses that match your patient’s clinical presentation. For each selected diagnosis, complete the “related factors” and “evidenced by” sections with specific assessment data from your patient record.
The template is most effective when completed collaboratively with the interdisciplinary team-physicians for medication adjustment, respiratory therapists for breathing technique coaching, and social workers for discharge planning and community resource referral.
Core nursing interventions fall into three categories: airway management and oxygenation, medication administration and education, and patient teaching for self-management and exacerbation prevention.
Airway and breathing interventions include:
Medication interventions involve administering rescue inhalers (short-acting beta-agonists for acute bronchoconstriction) and controller medications (inhaled corticosteroids for long-term inflammation suppression). Nurses:
A daily medication chart can help patients track adherence to controller medications after discharge.
Patient education covers:
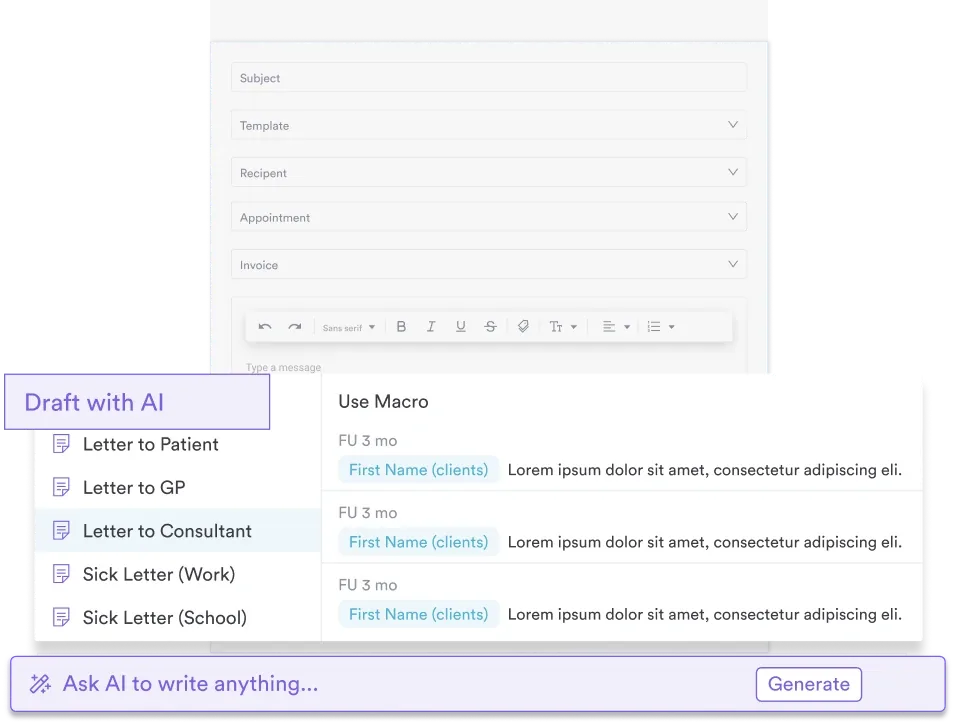
AI-assisted clinical documentation can help nurses capture teaching moments and document patient understanding in real time during consultations.
An asthma nursing care plan culminates in patient and family education that empowers self-management and prevents exacerbations. Nurses teach patients to:
Written discharge instructions should specify:
Lifestyle coaching frameworks complement this education by reinforcing trigger avoidance and physical activity guidelines within the patient’s capacity.
Templates save time while ensuring consistency and regulatory compliance. A pre-formatted asthma nursing care plan provides standard NANDA diagnoses, reduces transcription errors, prompts inclusion of all required assessment components, and generates audit-ready documentation that demonstrates evidence-based care delivery.
Busy clinical units benefit from templates that are customizable yet structured enough to guide decision-making.
Pabau's structured digital forms and automated care plan tracking help teams deliver consistent, compliant asthma care across multiple locations. Book a demo to see how practices organize assessment data, track outcomes, and meet regulatory audits.

Care plan documentation serves multiple purposes. It:
Compliance management features in practice management systems ensure required documentation elements are completed and accessible for review during regulatory inspections, accreditation surveys, or adverse event investigations.
A well-constructed asthma nursing care plan transforms assessment data into actionable clinical decisions, ensures consistent care delivery, and documents the nursing judgments that improve respiratory outcomes. By systematically addressing NANDA diagnoses through evidence-based interventions and measurable goals, nurses optimize asthma control and reduce preventable exacerbations.
Using a structured template accelerates care planning while maintaining clinical rigor and regulatory compliance. Documentation of care plans supports both patient safety and organizational accountability.
Download the asthma nursing care plan template above and customize it for your clinical setting to ensure every patient receives systematic, evidence-based asthma care.
Need a structured assessment framework? Psychiatric evaluation template provides a parallel model for systematic clinical assessment and documentation across mental and respiratory health intersections, including anxiety screening relevant to asthma exacerbation.
Managing a coexisting anxiety diagnosis? Anxiety nursing care plan offers a matching NANDA-based framework for patients whose breathing difficulty triggers or worsens anxiety symptoms.
Treating a pediatric patient? Consent to treat minor covers the documentation nurses need before starting assessment or treatment for a child.
The six primary diagnoses are Ineffective Airway Clearance, Impaired Gas Exchange, Ineffective Breathing Pattern, Activity Intolerance, Deficient Knowledge, and Anxiety. Selection depends on assessment findings; not all patients receive every diagnosis.
A nursing care plan is a clinician-authored document structured around NANDA diagnoses, goals, interventions, and rationale-used in hospital and clinical settings. An asthma action plan is a patient-facing written guide specifying which medications to take daily, when to use rescue inhalers, and what symptoms require emergency care.
Expected outcomes must be SMART: specific, measurable, achievable, relevant to the nursing diagnosis, and time-bound. Example: “Patient will maintain oxygen saturation ≥95% on room air within 24 hours” is measurable; “Patient will feel better” is not.
Evaluation frequency depends on the clinical setting and patient acuity. Acute exacerbations warrant reassessment every 2-4 hours; stable chronic management may be evaluated daily or at each visit. Plans should be revised if goals are not met or patient status changes.
Yes, but pediatric plans require adaptations: assessment parameters differ (behavioral cues in infants, self-reporting in older children), expected outcomes reflect developmental capacity, and interventions emphasize caregiver/family education alongside child-focused teaching.
Patient education is central to preventing exacerbations. Nurses teach trigger recognition and avoidance, correct inhaler technique, when to use rescue vs. controller medications, and red flags requiring emergency care. Documented patient understanding supports goal achievement and discharge readiness.