ICD-10 Code M32.9: Systemic lupus erythematosus, unspecified
M32.9 codes SLE when the notes name no organ involvement. Treat it as the fallba...
Last Updated: August 3, 2026
ICD-10 Code O74.7 captures a failed or difficult intubation when an anesthesiologist or CRNA administers general anesthesia during labor and delivery. It’s a billable, specific code that hospital coders and obstetric billing teams assign to the mother’s record to flag this complication separately from the delivery itself. Because it sits inside the O74 category of anesthesia complications, getting the documentation and sequencing right protects both the claim and quality reporting for the encounter.
ICD-10 Code O74.7 describes failed or difficult intubation for anesthesia during labor and delivery, a billable and specific ICD-10-CM diagnosis code
O74.7 falls under the parent category O74 (Complications of anesthesia during labor and delivery), within the O60-O77 range of the pregnancy and childbirth chapter
Code O74.7 applies specifically to intubation failure or difficulty during general anesthesia; separate subcodes cover spinal, epidural, and other anesthesia complications
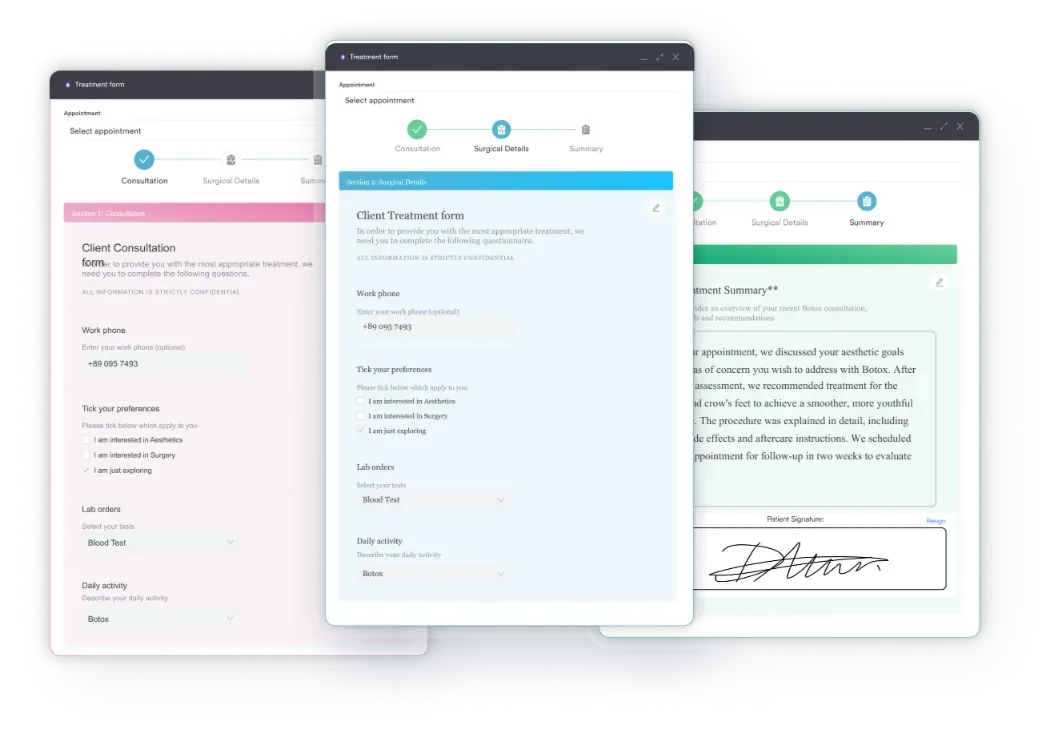
Pabau’s claims management software and digital documentation tools help obstetric and anesthesia billing teams capture complication codes accurately at the point of care
Difficult airway management during labor is one of the highest-stakes scenarios in obstetric anesthesia, and accurate ICD-10 coding starts with a clear understanding of what the code actually captures. OB/GYN practices and hospital billing teams use ICD-10 Code O74.7 to document a specific and serious anesthesia complication that requires its own distinct code rather than a catch-all unspecified entry.
Full code description: Failed or difficult intubation for anesthesia during labor and delivery.
ICD-10 Code O74.7 is a billable, specific ICD-10-CM diagnosis code. It is valid for use in the 2025 and 2026 ICD-10-CM code sets and has remained active across multiple fiscal year updates, confirmed by the CDC/NCHS ICD-10-CM web tool.
The code documents a complication that arises when the anesthesiologist or certified registered nurse anesthetist (CRNA) attempts, and fails or finds significant difficulty in, placing an endotracheal tube during the administration of general anesthesia for a patient in labor or during delivery.
Clinically, this scenario typically involves a patient with an unanticipated difficult airway. Physiological changes during pregnancy, including airway edema, increased breast tissue, and reduced functional residual capacity, make obstetric patients at higher risk for difficult or failed intubation than the general surgical population. The resulting documentation has direct coding, billing, and quality-reporting implications.
Most anesthesia complication codes in the O74 category are non-billable header codes, used only for organizational purposes in the ICD-10-CM tabular list. ICD-10 Code O74.7 is different: it is a fully billable, specific code with no further subdivision required. Coders should assign it directly, without appending a 7th character or any additional specificity digits.
Several ICD-10-CM official guidelines govern how this code is used. The CMS ICD-10 codes page and the NCHS ICD-10-CM Official Guidelines for Coding and Reporting outline the following principles for obstetric complication codes:
For facilities using claims management software, these sequencing rules should be embedded into claim scrubbing workflows so that O74.7 is never submitted as a principal diagnosis for an inpatient delivery encounter.
Review your anesthesia complication coding workflow quarterly. Failed intubation codes are frequently undercoded because anesthesiologists document the event in procedure notes rather than the discharge summary, meaning coders miss it entirely. Build a CDI query trigger for any case where general anesthesia was used during labor or delivery.
The O74 category covers every anesthesia complication that can arise during labor and delivery, from aspiration pneumonitis to epidural headache to cardiac arrest. Selecting the wrong subcode is among the most common obstetric coding errors, because the clinical scenarios can overlap in documentation. Understanding where O74.7 begins and ends helps coders avoid defaulting to unspecified codes.
The clearest distinction for coders is between O74.7 and O74.8. Use O74.7 specifically when the documented complication is failure or difficulty with endotracheal intubation, typically in the context of general anesthesia. O74.8 applies to anesthesia complications that do not fit any other named subcode. When documentation says “unanticipated difficult airway requiring video laryngoscopy” or “failed rapid sequence induction with conversion to mask ventilation,” O74.7 is the appropriate code.
O74.9 should be a last resort. The AAPC Codify ICD-10-CM lookup and official guidelines both reinforce that unspecified codes are appropriate only when documentation genuinely does not permit a more specific assignment. The same principle applies to other labor and delivery complications, such as O66.1: always code to the highest supported specificity.
Coding O74.7 correctly depends almost entirely on what the provider documents. Missing or ambiguous documentation is the primary reason obstetric anesthesia complications are either undercoded or coded to the unspecified O74.9.
For O74.7 to be coded, the anesthesia record or provider note must clearly document all three of the following elements:
Facilities with clinical documentation improvement (CDI) programs should flag labor and delivery cases where general anesthesia was administered, particularly for emergency cesarean deliveries. A CDI query asking the provider to clarify whether intubation was achieved without difficulty, required additional attempts, or required an alternative airway technique can unlock O74.7 in cases where the complication occurred but was not described with coding-ready language. Standardizing this with a structured intake assessment template gives anesthesiologists a consistent place to document airway findings before the CDI team ever needs to query the chart.
Coders who use digital intake forms in an integrated platform can prompt anesthesiologists to complete structured intraoperative complication fields, reducing the dependence on free-text note review. Practices coding other complex obstetric complications, such as O11.1, run into the same documentation problem: the clinical event occurred, the provider managed it, but the note lacks the specificity for accurate coding.
Build a CDI query template specifically for obstetric anesthesia cases. When a delivery record includes general anesthesia but no anesthesia complication code, trigger a query asking the provider to confirm whether intubation was uncomplicated. A two-minute query can capture O74.7 that would otherwise drop to O74.9 or disappear entirely.
For hospital outpatient departments and inpatient obstetric units, ICD-10 Code O74.7 flows into MS-DRG assignment through the delivery DRG grouper. Correctly capturing this code affects the facility’s case mix index and may influence the DRG weight for the delivery encounter, depending on whether the failed intubation qualifies as a major complication or comorbidity (MCC) or complication or comorbidity (CC) under the grouper logic.
Physician billing for the anesthesiologist or CRNA is a separate claim from the delivery itself, which is typically billed under a global obstetric care code such as CPT 59400. The anesthesia claim uses ASA procedure codes, not CPT procedure codes, for the delivery service. The O74.7 diagnosis code supports medical necessity on the anesthesia claim and may be required by certain payers to justify extended or complex anesthesia services billed with a higher base unit or time conversion.
There is no universal payer policy for O74.7. Medicare covers obstetric anesthesia through the inpatient prospective payment system for hospital claims and through the physician fee schedule for professional anesthesia claims. The ICD List and other lookup tools confirm that O74.7 carries no specific CMS-published payer edits that restrict its use as a secondary diagnosis. Commercial payers may have their own coverage policies, so it is worth confirming with individual payer contracts whether a failed intubation code on an anesthesia claim triggers additional documentation requirements or prior authorization review.
From a practice management perspective, obstetric units that track anesthesia complication rates for quality reporting (for example, under Joint Commission perinatal core measures) need this code documented consistently to support internal analytics. Practices using compliance management tools within their EHR workflows can set alerts for delivery encounters with general anesthesia but no documented anesthesia complication code, helping capture O74.7 before claims are submitted.
Before the ICD-10-CM transition in October 2015, coders used ICD-9-CM codes 668.81 and 668.82 (Other complications of anesthesia or other sedation in labor and delivery, delivered) as the closest available match, per the CMS General Equivalence Mappings. Neither code specifically identified failed or difficult intubation as a distinct obstetric complication.
The ICD-10-CM system resolved this with O74.7, giving coders a specific billable code for a clinical event that previously required a non-specific assignment.
For historical claims analysis, revenue cycle teams should be aware that pre-2015 data coded to 668.8x may represent a mix of complications now separable under ICD-10, including failed intubation (O74.7), toxic local anesthetic reactions (O74.4), and other unclassified anesthesia events (O74.8). The WHO ICD-10 browser provides international classification context for O74 codes, though US facilities should use the ICD-10-CM tabular list maintained by NCHS rather than the international ICD-10 edition.
Practices managing obstetric and reproductive health documentation can benefit from fertility practice management software designed with maternal care workflows in mind. Integrating complication code capture into standard delivery documentation templates reduces coding lag and denial rates on affected claims. Teams looking to understand how these coding lags affect the bigger picture can also track denial patterns with a revenue cycle management framework that spans departments.
Pabau's integrated claims management and digital documentation tools help OB/GYN and anesthesia billing teams capture complication codes like O74.7 accurately at the point of care, reducing denials and improving case mix documentation.

ICD-10 Code O74.7 exists within a broader framework of maternal complication codes that obstetric and anesthesia billing teams should understand together. The O74 category itself falls under the O60-O77 block, which covers complications arising specifically during the intrapartum period, not antepartum care or postpartum recovery.
For practices reviewing their obstetric documentation processes, structured medical forms in healthcare workflows directly influence how well complications like failed intubation are captured before billing. When anesthesiologists complete standardized intraoperative complication checklists rather than free-text notes alone, coders receive cleaner input and submit more accurate claims. Facilities that have integrated structured clinical records into their delivery workflows catch more anesthesia complication codes that would otherwise go unrecorded.
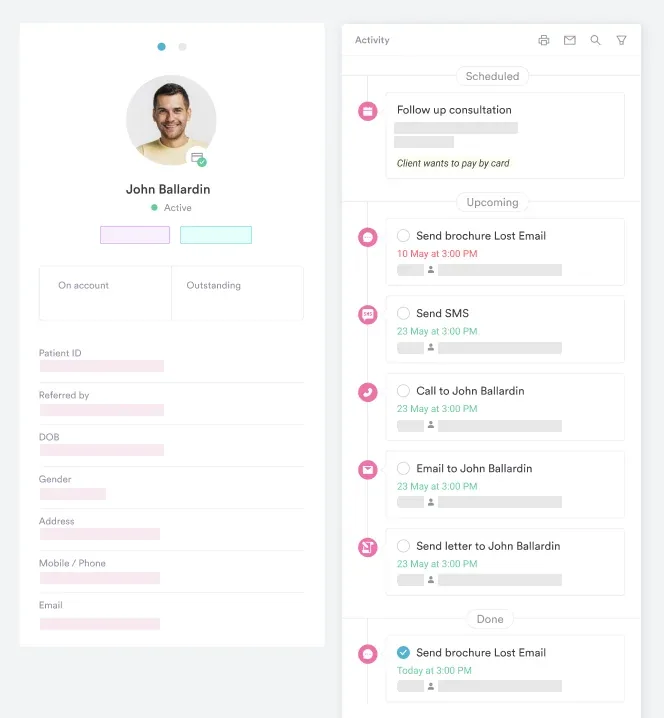
Revenue cycle managers overseeing obstetric units should also consider how their EHR integration strategy connects anesthesia records, delivery notes, and the coding team. When these data sources are siloed, O74.7 is among the codes most likely to be missed, because the clinical event appears in the anesthesia record but never surfaces in the discharge summary that coders primarily review. Practices exploring broader practice management solutions for obstetric and women’s health settings should evaluate whether the platform supports cross-departmental documentation workflows that surface anesthesia complication data to the coding team automatically.
Failed or difficult intubation during labor and delivery is a serious clinical event, and it deserves a specific, accurate code. ICD-10 Code O74.7 captures that event precisely, distinguishing it from every other anesthesia complication in the O74 category. The code is billable, specific, and valid through the current code set.
The most common barrier to accurate use is documentation, not coding knowledge. Facilities that build structured anesthesia complication capture into their delivery workflows, supported by CDI queries and integrated clinical record tools, will see O74.7 assigned when it belongs and dropped when it does not. To see how Pabau supports accurate diagnostic code workflows for obstetric and specialist practices, book a demo.
Need a framework for obstetric and women’s health documentation? OB/GYN practice management software covers how Pabau supports clinical workflows for obstetric and gynecology practices.
Need billing context for the delivery encounter itself? CPT 59510 covers routine obstetric care for cesarean delivery and the postpartum period that O74.7 explicitly excludes.
Want to reduce coding errors with structured clinical forms? Pabau’s digital forms feature explains how structured intake and intraoperative forms cut down on the missing documentation that causes coding errors.
ICD-10 Code O74.7 is a billable ICD-10-CM diagnosis code used to document failed or difficult intubation for anesthesia during labor and delivery. It applies when an anesthesiologist or CRNA encounters significant difficulty or failure in placing an endotracheal tube while administering general anesthesia during a labor or delivery encounter. The code is assigned as an additional (secondary) diagnosis, not as a principal diagnosis for the delivery encounter.
Yes, O74.7 is a fully billable and specific ICD-10-CM diagnosis code, valid across the 2025 and 2026 code sets. It requires no further subdivision or additional specificity characters. Coders assign it directly when documentation supports the complication.
O74.7 applies specifically to failed or difficult intubation during general anesthesia for labor and delivery. O74.8 covers other anesthesia complications during labor and delivery that do not fit any named subcode (such as certain equipment failures or anesthetic agent reactions). O74.9 is the unspecified anesthesia complication code, used only when documentation does not allow a more specific assignment. Coders should default to the most specific code the documentation supports and avoid O74.9 when the complication can be identified.
The parent code is O74 (Complications of anesthesia during labor and delivery), which covers maternal complications arising from the administration of general, regional, or local anesthetic, analgesic, or other sedation during labor. O74 itself is a non-billable header code; the billable specificity sits in the subcodes, including O74.7.
The provider’s anesthesia record or clinical note must document the nature of the intubation difficulty (e.g., “failed intubation,” “grade 3-4 laryngoscopy,” “unanticipated difficult airway”), its relationship to anesthesia administration, and that it occurred during a labor or delivery encounter. A CDI query can clarify ambiguous documentation before the code is assigned.
The closest ICD-9-CM codes were 668.81 and 668.82 (Other complications of anesthesia or other sedation in labor and delivery, delivered), per the CMS General Equivalence Mappings. Neither was specific to failed or difficult intubation. ICD-10-CM introduced O74.7 as a specific code for this complication, allowing coders to document it distinctly for the first time.
No. O74.7 is specific to labor and delivery. A failed or difficult intubation during pregnancy (the antepartum period) is coded to O29.6 instead, and one during the puerperium (the postpartum period) is coded to O89.6. A non-obstetric failed or difficult intubation uses a code outside the O-chapter entirely. Confirm the encounter is a labor or delivery episode before assigning O74.7.