ICD-10 Code S42.009B: Open clavicle fracture, initial encounter
ICD-10 Code S42.009B identifies a fracture of an unspecified part of an unspecif...
Last Updated: July 31, 2026
ICD-10 Code M17.9 is the billable diagnosis code for osteoarthritis of the knee when laterality is not documented or cannot be determined
M17.9 is valid and billable for FY 2026. Use M17.11, M17.12, or M17.0 when the affected side is documented in the clinical record
Using M17.9 when laterality is known can trigger payer audits. Always document clinical rationale when applying the unspecified code
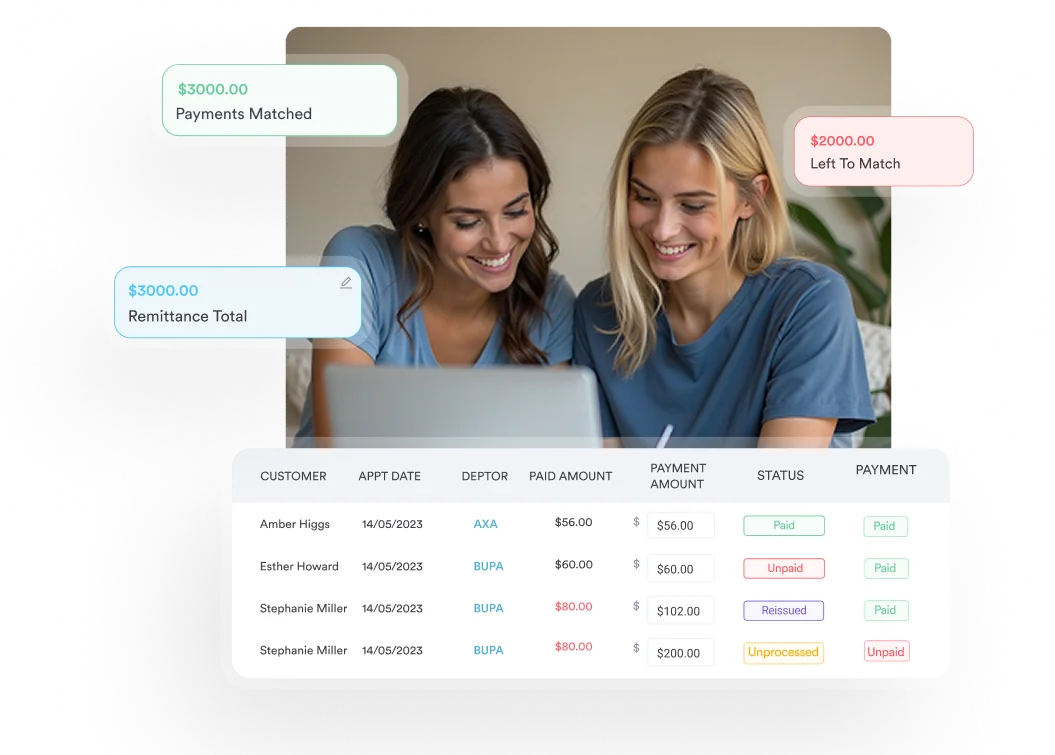
Practice management software like Pabau provides claims management and client record tools that support accurate M17.9 documentation and streamlined billing workflows for orthopedic and physical therapy practices
ICD-10 Code M17.9 is the diagnosis code for osteoarthritis of the knee, unspecified. It applies when the clinical documentation doesn’t identify which knee is affected, or when the presentation doesn’t meet the bilateral primary criteria for M17.0.
Clinicians also chart this presentation as gonarthrosis or degenerative joint disease (DJD) of the knee — different terms for the condition M17.9 classifies.
This reference covers where M17.9 sits in the M17 hierarchy, when to use it instead of M17.11 or M17.12, documentation requirements, and the CPT codes billed alongside it.
Understanding where M17.9 sits in the ICD-10-CM hierarchy, and when payers expect a more specific code, keeps claims clean and helps practices avoid post-payment recovery audits. Accurate client record documentation is the first line of defense when a payer questions unspecified coding.
M17.9 is the ICD-10-CM diagnosis code for osteoarthritis of the knee, unspecified. It falls under Chapter 13 (Diseases of the Musculoskeletal System and Connective Tissue, M00-M99), subcategory M15-M19 (Osteoarthritis), and specifically under M17 (Osteoarthritis of the knee).
M17 sits inside the broader set of ICD-10 codes for osteoarthritis, which cover nearly every major joint and each carry their own laterality rules. Coders searching for the ICD-10 code for knee osteoarthritis land on M17.9 by default whenever the chart doesn’t document a side.
Clinically, the code describes a noninflammatory degenerative disease of the knee joint. The degeneration falls into three broad categories.
“Unspecified” in this context means the documentation doesn’t clearly identify which knee is affected, or both knees are involved in a pattern that doesn’t meet the criteria for M17.0.
According to the CDC/NCHS ICD-10-CM coding tool, M17.9 is confirmed billable and valid for FY 2026. The code has no Type 1 Excludes or Type 2 Excludes notes that restrict its use in the M17 subcategory.
M17.9 is one of 11 billable codes within the M17 subcategory. Knowing the full hierarchy prevents miscoding when laterality or etiology is documented.
The CMS ICD-10-CM coding guidelines emphasize that coders should assign the most specific code supported by the documentation. M17.9 is correct only when the clinical record genuinely does not specify laterality.
The most common coding error with knee OA is applying M17.9 when a laterality-specific code is clearly supported by the documentation. Here is the practical decision framework.
A practical tip for physiotherapy clinic compliance workflows: If the therapist’s SOAP note documents “left knee strengthening protocol,” the coder should assign M17.12, not M17.9. The treatment site is sufficient documentation of laterality.
The same logic explains why a search for the ICD-10 code for left knee osteoarthritis should lead a coder to M17.12, not M17.9 — once a side is on the record, the unspecified code no longer applies.
When the provider’s assessment says ‘bilateral knee OA’ but treatment targets only one side, assign both M17.0 (bilateral primary) and the laterality-specific code for the treated knee as needed. Never default to M17.9 when the bilateral nature is explicitly documented.
Payers increasingly apply clinical documentation integrity (CDI) edits to unspecified codes. For M17.9, auditors look for evidence that laterality was genuinely unknown at the time of the encounter. Strong documentation includes three elements.
The note should indicate why laterality isn’t specified. Acceptable rationale includes:
Document this explicitly in the assessment or plan.
Record joint-specific findings: range of motion measurements, crepitus, effusion, and tenderness. Bilateral exam findings without a dominant side support M17.9. A unilateral finding without documented explanation for the unspecified code creates audit exposure. Practices tracking functional outcomes can layer in a validated instrument like the WOMAC index to document symptom severity alongside the exam.
When X-rays or MRI are ordered, reference them in the assessment. If imaging confirms bilateral OA with no dominant affected side, note this. Practices using digital intake forms can capture laterality data at registration, giving coders a documented source before the clinical note is finalized.
The AAPC ICD-10-CM code reference notes that unspecified codes are acceptable only when they represent the highest degree of certainty for the encounter. Documentation should support that standard.
Pabau's claims management and client record tools help orthopedic and physical therapy practices document ICD-10 diagnoses accurately, reduce coding errors, and submit cleaner claims.

Several ICD-10-CM Official Guidelines directly affect how M17.9 is coded and sequenced. Review these with your coding team before submission.
When the knee OA is the reason for the encounter, M17.9 is sequenced as the principal diagnosis. If the visit addresses pain management for a chronic condition, M17.9 leads and any pain code (such as M25.561 or M25.562 for knee pain) is sequenced as an additional code only when it adds clinically relevant information beyond what M17.9 captures.
M17.9 is commonly paired with codes that document functional status or comorbidities. Consider adding:
For practices transitioning older records or working with legacy claims data, M17.9 maps approximately to two ICD-9-CM codes: 715.36 (Osteoarthrosis, localized, not specified whether primary or secondary, lower leg) and 715.96 (Osteoarthrosis, unspecified whether generalized or localized, lower leg).
Neither ICD-9 code carries the laterality specificity of the M17 subcategory, which is one reason ICD-10-CM introduced the expanded code set. Practices running physiotherapy clinic management software with integrated billing modules can automate crosswalk lookups during claims preparation.
Run a quarterly coding audit on all claims submitted with M17.9. Pull 20-30 charts at random and verify that the clinical documentation does not specify laterality. If more than 15% of audited charts contain laterality documentation, your query protocols need tightening.
M17.9 pairs with a wide range of CPT codes depending on the treating specialty. The table below lists the most frequently associated procedures. Medical necessity must always be supported by the clinical documentation, not assumed from the diagnosis code alone.
For practices focused on conservative knee OA management, the current physical therapy evaluation codes are 97161, 97162, and 97163 for low, moderate, and high complexity evaluations. These replaced CPT 97001, which was deleted effective January 1, 2017, and is no longer billable. The claims management software Pabau uses helps practices flag mismatches between diagnosis codes and procedure codes before submission.
Orthopedic practices billing CPT 27447 for total knee arthroplasty with M17.9 should expect additional payer scrutiny. Major surgical procedures are more likely to require laterality-specific codes, and pairing M17.9 with a knee replacement claim creates an inconsistency that auditors flag.
Practice management software built for physical therapy can flag this kind of mismatch automatically, before the claim ever reaches the payer.
Unspecified codes are not inherently wrong, but they draw attention when payers compare the code to the documented clinical findings. For M17.9 specifically, the audit risk is concentrated in two scenarios.
This is the most common denial trigger. The physical exam documents “right knee swelling.” The imaging report references the right knee. But the coder assigns M17.9 anyway.
Payers running automated code-to-documentation edits flag this pattern. Recovery auditors (RACs and MACs) specifically target unspecified codes on claims where other documentation elements suggest a specific site. The fix is a coder query workflow that prompts providers to confirm laterality before claim submission.
Medicare and commercial payers expect laterality specificity when approving high-cost orthopedic procedures. A total knee replacement (CPT 27447) or a hyaluronic acid injection series billed with M17.9 instead of M17.11 or M17.12 may trigger a pre-payment review or post-payment audit.
Practices handling a high volume of orthopedic procedures benefit from physical therapy EMR software that builds laterality verification into the pre-visit intake workflow.
On the physical therapy side, physical therapy EMR platforms that embed laterality fields directly into evaluation templates reduce the chance of a therapist submitting an unspecified code when the treatment side is clearly documented in the functional assessment.
Bilateral knee injections (a hyaluronic acid series or a corticosteroid injection) are a frequent denial trigger. When the procedure note documents each knee separately, the claim needs two line items, each tied to its own laterality-specific code: M17.11 for the right knee and M17.12 for the left, with the injection code split by modifier 50 or reported as separate lines per payer convention. Submitting a single M17.9 line for an encounter the note already splits by side is what draws the review, not the injection itself.
Etiology can trip up coding the same way laterality does. Knee osteoarthritis that develops after an ACL reconstruction or another documented injury belongs under the post-traumatic M17.2/M17.3x codes, not M17.9, once the operative note ties the degeneration to that earlier trauma. The chart has to support both the side and the cause before a laterality-specific or etiology-specific code replaces the unspecified one.
The WHO ICD-10 classification browser confirms that the M17 subcategory was designed to support laterality-specific coding as the default. M17.9 exists for genuine clinical ambiguity, not as a convenience shortcut.
Accurate ICD-10 Code M17.9 coding depends on documentation captured before the claim is ever assembled. Pabau supports this upstream by enabling digital intake forms that collect the affected body region and laterality during patient registration. When that information flows into the clinical record, coders have a documented source to confirm laterality rather than defaulting to an unspecified code.
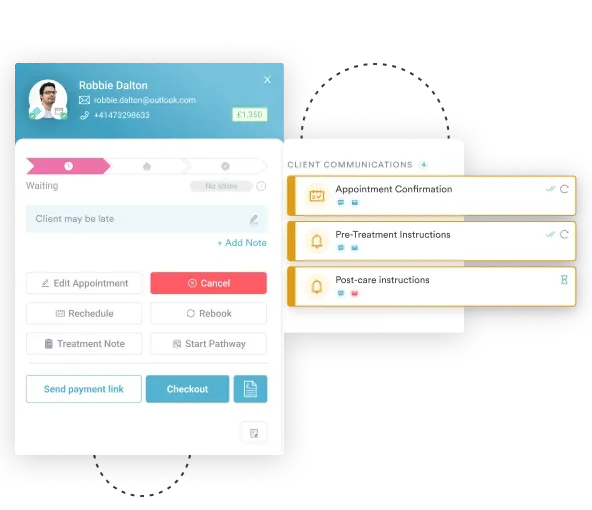
Practices running physical therapy, sports medicine, or orthopedic practices use Pabau’s claims management tools to catch code-to-documentation mismatches before submission. The platform’s sports medicine software workflows support structured SOAP notes that prompt clinicians to document laterality, etiology, and functional status at each visit.
For practices managing high claim volumes across musculoskeletal diagnoses, Pabau’s automated workflow tools can flag encounters where an unspecified code is applied against a high-cost procedure code, triggering a coder review before the claim reaches the clearinghouse. This is the kind of pre-submission audit that prevents the more expensive post-payment recovery audits that follow denial patterns.
Practices opening a physiotherapy clinic or expanding into orthopedic services should build laterality verification into their intake and documentation templates from day one. Retrofitting those workflows after the first audit is far more disruptive than building them correctly upfront.
The same principle applies for occupational therapy software users managing knee OA patients alongside functional rehabilitation goals: The diagnosis code must reflect what the clinical note says, not an assumption about what the provider probably meant.
Coders managing multi-specialty billing may also want to check other recently published references, including CPT code 11641 for facial lesion excision, CPT code 69210 for impacted cerumen removal, and CCSD code 0011G for FAP genetic analysis billing.
ICD-10 Code M17.9 is a valid, billable code for knee osteoarthritis when laterality is genuinely undetermined. Using it after the record already identifies the affected knee is what draws audit attention.
Practices that build laterality verification into their intake and documentation workflows reduce unspecified coding errors before they reach the payer. Pabau’s digital forms and structured clinical note tools make that verification part of the standard visit workflow rather than an afterthought at billing. To see how Pabau supports orthopedic and physical therapy documentation, book a demo.
Need structured tools for musculoskeletal documentation? Physical therapy EMR built for orthopedic and rehabilitation clinics, supporting laterality-specific ICD-10 coding workflows.
Want to reduce claim denials across your practice? Claims management software from Pabau helps practices flag code-to-documentation mismatches before submission.
Looking for sports medicine-specific workflows? Sports medicine software from Pabau supports structured SOAP notes with built-in laterality fields for musculoskeletal diagnoses.
ICD-10 Code M17.9 is the diagnosis code for osteoarthritis of the knee, unspecified. It is used when the clinical documentation does not identify which knee is affected, or when the degenerative joint disease cannot be clearly classified as bilateral primary (M17.0) or laterality-specific (M17.11 for right, M17.12 for left).
Use M17.9 only when the clinical record genuinely does not specify which knee is affected. If the provider’s note, physical exam, or imaging report identifies the right or left knee, assign M17.11 or M17.12 respectively. Using M17.9 when laterality is documented creates audit exposure and is inconsistent with ICD-10-CM specificity guidelines.
Yes. M17.9 is confirmed billable and valid for FY 2026 by the CDC/NCHS ICD-10-CM coding tool. It has no Type 1 or Type 2 Excludes notes that restrict its use within the M17 subcategory.
M17.9 maps approximately to ICD-9-CM 715.36 (osteoarthrosis, localized, not specified whether primary or secondary, lower leg) and 715.96 (osteoarthrosis, unspecified whether generalized or localized, lower leg). These are approximate crosswalk equivalents. Neither ICD-9 code captures the laterality specificity available in the ICD-10-CM M17 subcategory.
It can, particularly when paired with high-cost procedures like total knee arthroplasty (CPT 27447) or when other documentation in the claim suggests a specific laterality. Recovery auditors (RACs and MACs) flag unspecified codes on claims where the supporting documentation implies a specific site. Documenting clinical rationale for unspecified coding and running pre-submission chart reviews reduces this risk.
The clinical record should include a provider’s statement indicating why laterality is undetermined, bilateral or non-lateralized physical exam findings, and any imaging references that do not confirm a dominant affected side. When using M17.9 for a high-cost procedure, adding a brief clinical rationale note in the assessment section significantly reduces denial and audit risk.
Yes. Gonarthrosis is the clinical term for degenerative joint disease of the knee, and M17.9 is the ICD-10-CM code assigned when that diagnosis doesn’t specify which knee is affected.
Degenerative joint disease (DJD) of the knee is another name for osteoarthritis of the knee, and it’s coded the same way: M17.9 when laterality isn’t documented, M17.11 for the right knee, and M17.12 for the left.