CPT code 00103: Anesthesia for eyelid reconstruction billing guide
CPT code 00103 is the anesthesia code for reconstructive procedures on the eyeli...
July 23, 2026
ICD-10 code B86 is a billable, specific diagnosis code for scabies in FY2026 ICD-10-CM, used across outpatient and institutional settings.
B86 covers all scabies presentations including crusted (Norwegian) scabies and sarcoptic itch under a single code with no subcategory options.
Documentation must specify the clinical basis for diagnosis, including characteristic burrows, pruritic eruption, and any infection control measures taken.
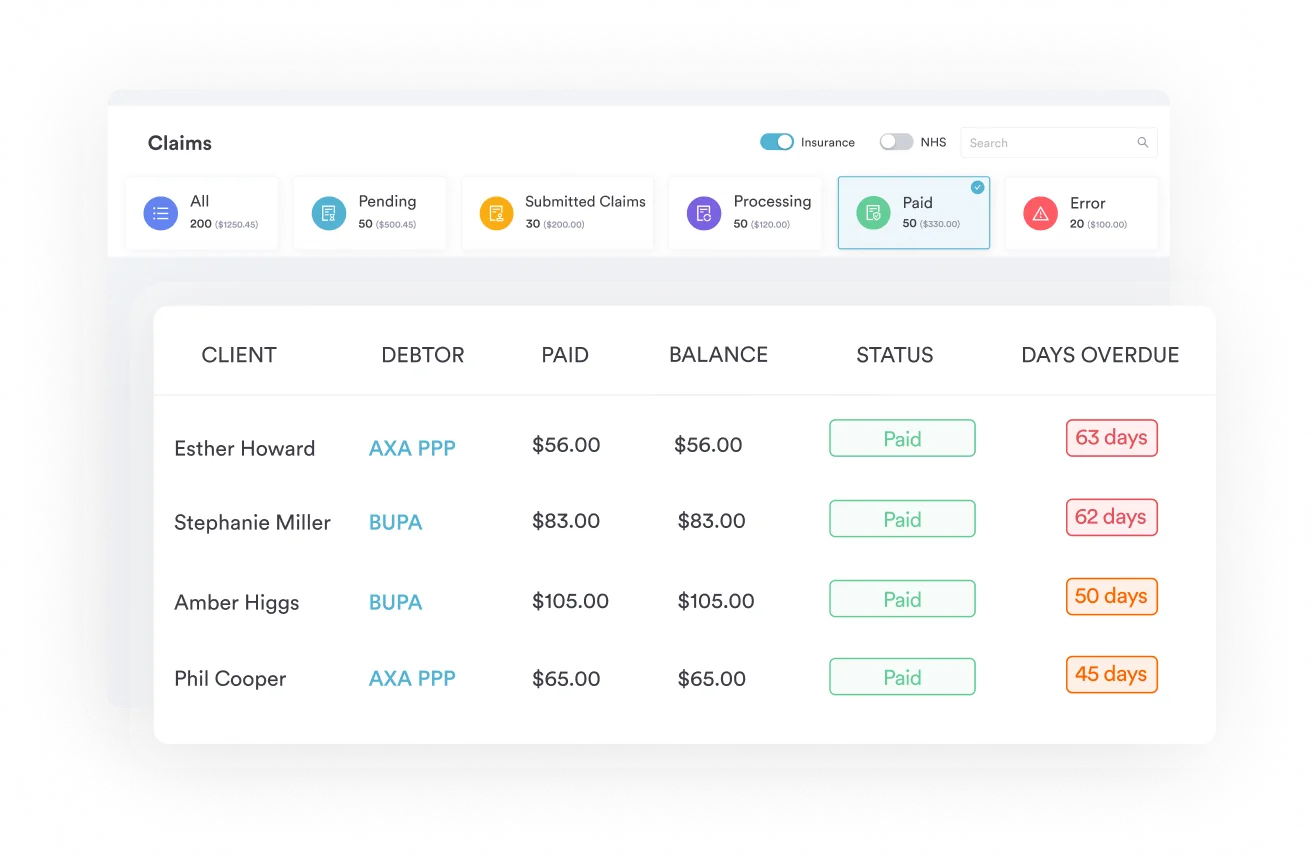
Pabau’s claims management workflows help dermatology and primary care teams submit B86 claims accurately and track reimbursement outcomes.
ICD-10 code B86 is the single billable, specific ICD-10-CM code for scabies, a contagious skin infestation caused by the mite Sarcoptes scabiei. It covers every presentation, including classic and crusted (Norwegian) scabies and sarcoptic itch, under one code with no subcategory options in the FY2026 release.
B86 is classified under Chapter 1 of ICD-10-CM: Certain infectious and parasitic diseases (A00-B99), within the block B85-B89 covering pediculosis, acariasis and other infestations. The CDC/NCHS ICD-10-CM web tool confirms B86 as a billable, specific code valid for FY2026.
Clinically, scabies is a contagious cutaneous inflammation caused by the bite of the mite Sarcoptes scabiei. It is characterized by pruritic papular eruptions and burrows affecting primarily the skin folds, interdigital spaces, wrists, and genitals. The itch is typically worse at night.
In immunocompromised patients, the presentation escalates to crusted (Norwegian) scabies, where mite counts are vastly higher and the risk of institutional spread is significant.
B86 is fully billable in the FY2026 ICD-10-CM release. There are no subcategory options: one code covers all variants of scabies. Specificity modifiers do not apply here.
| Field | Value |
|---|---|
| Code | B86 |
| Full description | Scabies |
| Billable/specific | Yes (FY2026) |
| Chapter | Chapter 1: Certain infectious and parasitic diseases (A00-B99) |
| Block | B85-B89: Pediculosis, acariasis and other infestations |
| ICD-9-CM crosswalk | 133.0 (Scabies) |
| MS-DRG grouping | MS-DRG v43.0 (v43.1 from April 2026) |
The CMS ICD-10 codes page provides annual update files where coders can confirm effective dates and any tabular changes for B86 in each fiscal year. Validate against the current FY file rather than legacy coding references, since other codes in the B85-B89 block can change between fiscal years even when B86 itself does not.
The ICD-10-CM tabular list includes one official “Applicable To” note under B86. It is an accepted alternative diagnosis that maps to this single code, not a separate condition requiring a different code.
Coders and clinicians also use other terms for scabies in day-to-day practice. These are general clinical terminology rather than official tabular synonyms, but they still map to B86:
None of these terms changes the code: whether the note uses the official tabular synonym or general clinical terminology, it all maps to B86. The distinction matters for clinical documentation, especially when institutional infection control is involved, but the code itself does not differentiate between classic and crusted presentations.
Coders who see “Norwegian scabies” on a clinical note should still report B86.
Document the presenting term exactly as the clinician recorded it, then map it to the correct code in the tabular. This creates a clear, audit-ready chain between the clinical note and the submitted code.
Payers routinely request clinical documentation to support a B86 diagnosis. Vague documentation (“possible scabies” or “rule out scabies”) is not sufficient. The diagnosis must be confirmed in the clinical note before B86 is reported.
Crusted scabies carries a higher infection control burden than classic scabies, but the ICD-10-CM code remains B86. Documentation for these cases should explicitly identify the presentation as crusted or Norwegian scabies to justify the intensity of management documented in the encounter.
This does not change the reported code, but it does protect the practice if the visit level or additional services are reviewed. Immunocompromised patients with recurring or hard-to-clear infestations may also need ongoing case coordination; practices billing chronic care management alongside B86 should review the requirements under CPT code 99490 before submitting both on the same claim.
Practices using clinical documentation workflows benefit from structured note templates that prompt providers to capture all exam findings, not just the diagnosis label. This is particularly valuable in high-volume dermatology and primary care settings where scabies is a common urgent presentation. For a closer look at how these systems work, see our guide to clinical documentation software.
Maintaining HIPAA-compliant medical records for infectious disease diagnoses like scabies also requires that infection control communications with patients are documented in the record. Verbal counseling alone is not auditable.
Dermatology practices can standardize this intake-to-documentation process with a dermatology intake form template, paired with a dermatology consent template to keep exposure history, exam findings, and treatment consent in one place before the encounter closes.
Flag all scabies encounters for infection control documentation before claim submission. If the note lacks explicit mention of patient education about laundering, decontamination, or treatment of household contacts, return it to the provider for addendum before coding. Missing this detail is a leading audit vulnerability for B86 claims.
B86 carries no Type 1 Excludes note, so it can be reported alongside other codes on the same claim. Coders should still understand the distinction between B86 and adjacent codes in the B85-B89 block to avoid miscoding.
| Code | Description | Relationship to B86 |
|---|---|---|
| B86 | Scabies | Primary code for all scabies presentations |
| B88.0 | Other acariasis | Use for acariasis not caused by Sarcoptes scabiei (e.g. Demodex infestation, other mites) |
| B85.0-B85.4 | Pediculosis | Lice infestations – separate condition, different code block |
| B87.x | Myiasis | Fly larva infestation – distinct from mite infestation |
| Z20.7 | Contact with/(suspected) exposure to pediculosis, acariasis and other infestations | Report for a documented exposure to scabies before infestation is confirmed; it lists “exposure to scabies” as an applicable synonym. Not a substitute for B86 once scabies is diagnosed |
| L30.9 | Dermatitis, unspecified | Do not use when scabies is confirmed – specificity requires B86 |
The most common miscoding error is reporting B88.0 (Other acariasis) when the provider has documented confirmed scabies. B88.0 covers Demodex infestation, acariasis from other mite species, and unspecified mite infestations. Once the clinician identifies Sarcoptes scabiei as the causative agent or documents a clinical diagnosis of scabies, B86 is the correct and only appropriate code.
A related but distinct scenario is documented exposure to scabies without a confirmed infestation, such as an asymptomatic household or care-home contact. In that case report Z20.7 (Contact with and suspected exposure to pediculosis, acariasis and other infestations), which lists “exposure to scabies” among its applicable synonyms. Switch to B86 only once the infestation itself is confirmed.
The same specificity principle applies across dermatology coding generally: a diagnosis such as psoriasis (L40.0) requires its own distinct code rather than a generic skin-condition placeholder.
The AAPC Codify ICD-10-CM lookup provides cross-reference context for B86 within the full B85-B89 block, useful when coders are distinguishing between infestation types during chart review.
Practices managing skin condition coding can benefit from pairing B86 with appropriate secondary codes where relevant. For example, if a secondary bacterial skin infection, such as impetigo or cellulitis, has developed due to scratching, that secondary diagnosis should be coded in addition to B86 using the correct L or A/B series code.
Code the primary reason for the encounter first; secondary complications follow. Practices documenting cellulitis as a secondary diagnosis can use a cellulitis nursing care plan template to standardize the follow-up plan.
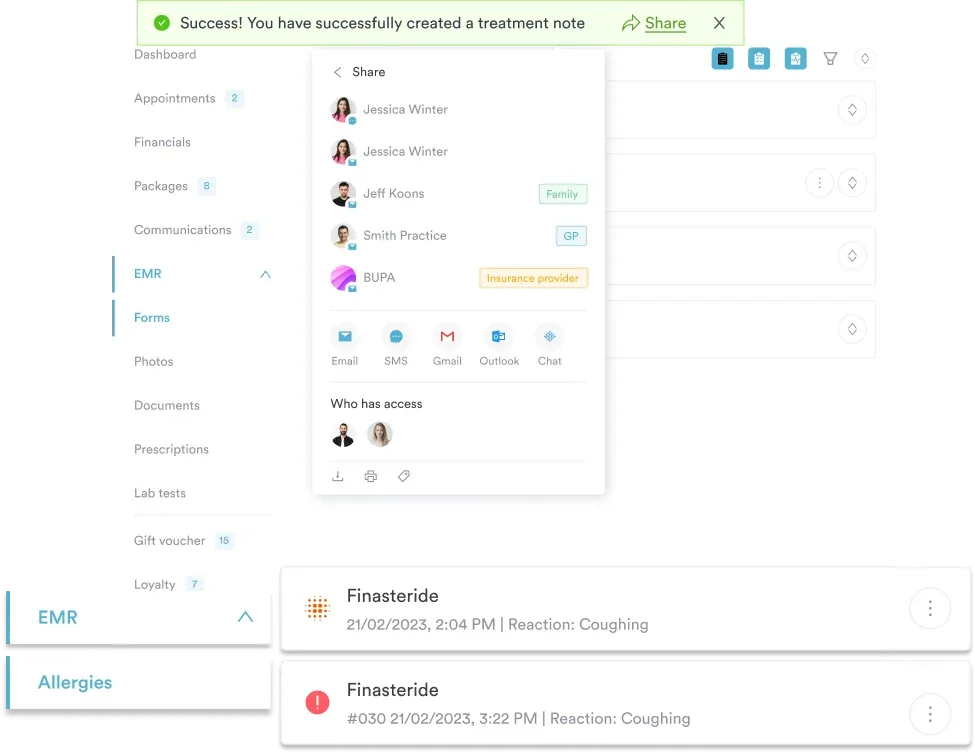
Pabau helps dermatology and primary care teams document encounters accurately, manage claims, and reduce denial rates for codes like ICD-10 B86. See how structured records and integrated billing tools work together.

B86 is a diagnosis code only. It must be paired with a procedure or evaluation and management (E/M) CPT code on the claim. The pairing depends on the type of encounter and services rendered.
Payers expect the CPT code level to reflect the documented complexity of the encounter. A crusted scabies case in an immunocompromised patient requiring infection control coordination and prescription management will typically support a higher-level E/M than a straightforward classic presentation in a healthy adult. Medical decision making documentation drives CPT level selection, not the diagnosis code.
Practices with robust claims management workflows can link the documented MDM complexity directly to the submitted CPT level, creating an audit-ready chain from clinical note to claim. This is especially valuable for dermatology teams handling high volumes of infectious skin conditions.
Scabies is primarily an outpatient diagnosis. Claims for B86 route through standard CMS and commercial payer adjudication without special prior authorization in most cases. However, several workflow steps reduce denial risk.
In outpatient settings, B86 is the principal or first-listed diagnosis when scabies is the primary reason for the encounter.
In inpatient settings, the code may appear as a secondary diagnosis if the patient was admitted for another condition and scabies was identified incidentally or as a complication.
Coders reporting the inpatient stay itself alongside B86 should reference the applicable hospital E/M code, such as CPT code 99236 for observation or inpatient care completed on the same day, or CPT code 99232 for subsequent hospital care.
In institutional settings such as care homes or rehabilitation facilities, a scabies diagnosis may also trigger infection control reporting obligations under state public health regulations, which should be flagged to the clinical lead, not just the coding team.
Facility visits in these settings are commonly billed under a dedicated code such as HCPCS code S9124, so confirm the correct visit code applies before submitting the claim alongside B86.
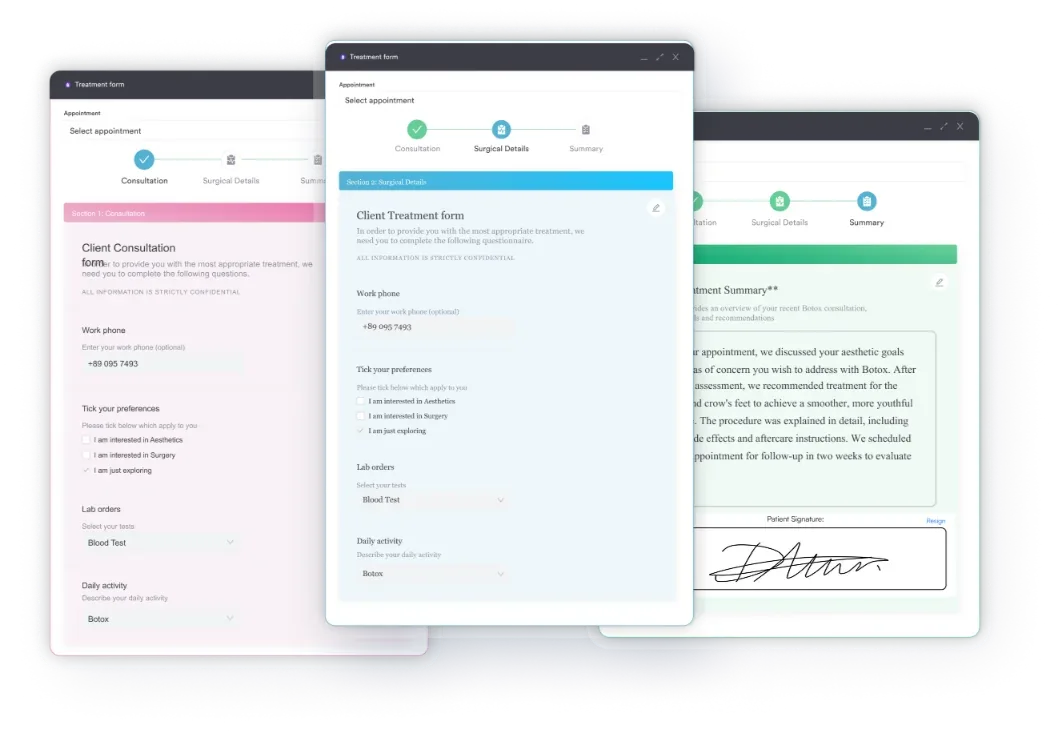
Dermatology and primary care practices can reduce these denials by building structured encounter templates that prompt for the diagnosis criteria relevant to B86. Pabau’s digital intake forms and clinical note tools allow teams to create condition-specific templates that capture the required documentation fields at the point of care rather than chasing addenda after the patient leaves.
The same condition-specific approach applies across specialties: a dedicated adolescent intake questionnaire, built for a different population, follows the same principle of capturing the exact fields a diagnosis requires before the visit ends.
The WHO ICD-10 browser provides the international classification context for B86, useful when coding for patients presenting from regions with high scabies prevalence or when cross-referencing with international coding standards for multi-site practices.
Teams working across dermatology practice workflows benefit from having claims review integrated directly into the practice management platform, so that coding accuracy checks happen before claims are submitted.
Build a B86 encounter template with checkboxes for: confirmed diagnosis wording, physical exam findings (burrows, papules, excoriations), treatment prescribed, infection control counseling documented, and household contacts discussed. Staff complete the checklist before signing. This single workflow change addresses the most common documentation deficiencies behind B86 denials.
For practices still managing legacy data or working with older claims, B86 maps from ICD-9-CM code 133.0 (Scabies). The transition to ICD-10-CM introduced no clinical scope change for this diagnosis; the condition maps one-to-one. There are no dual coding requirements for claims submitted under the current system.
B86 has been a terminal, billable code since ICD-10-CM was first implemented in 2015, with no subcategory options below it. Despite this, some legacy coding reference tools display incomplete tabular information, which can cause confusion for teams that have not validated their references against the current fiscal year file. The FY2026 tabular confirms B86 remains a terminal, billable code.
Practices managing historical encounter data should confirm that legacy B86 claims used the code descriptor and format valid at the time of service, since fiscal-year tabular updates elsewhere in the B85-B89 block can affect adjacent codes even when B86 itself stays unchanged. Using outdated code tables is a common audit finding.
Accurate historical records are foundational to structured patient records management. When a code’s descriptor or reporting requirements change between fiscal years, the practice’s documentation system needs to reflect the version in effect at the date of service, not the current year’s table.
Maintaining patient data security practices around diagnostic coding records also matters here: legacy ICD-9 crosswalk files may contain patient data and should be handled under the same access controls as active records.
Practices that routinely diagnose and treat skin infestations, including scabies, benefit from a platform that integrates clinical documentation with billing in a single workflow. When the clinical note and the claim are handled in separate systems, documentation deficiencies that cause B86 denials are harder to catch before submission.
Pabau’s compliance management tools help practices build structured clinical note templates, track which encounter records are complete before claims submission, and maintain audit-ready documentation across their patient population. For dermatology and primary care teams handling infectious skin diagnoses at volume, this reduces the manual review burden significantly.
Teams evaluating platforms as part of this decision can compare options in our roundup of dermatology EHR software.
The platform also supports condition-specific intake templates that can be configured to capture scabies-specific intake data, including exposure history, symptom onset, and prior treatment attempts. This information feeds directly into the clinical record, giving providers the documentation foundation they need to support a confirmed B86 diagnosis from the first patient touchpoint.
ICD-10 code B86 is a single, billable, specific code covering all scabies presentations in FY2026 ICD-10-CM. Accurate coding starts with confirmed clinical documentation, not just a diagnosis label: providers need to record physical findings, treatment, and infection control counseling before the coder submits B86 on a claim.
Pabau’s integrated clinical documentation and claims management tools give dermatology and primary care teams the structured workflows to capture that detail at the point of care. To see how Pabau handles diagnostic coding documentation, book a demo with the team.
Coding another dermatology diagnosis? The ICD-10 code L40.0 (psoriasis) guide shows how the same specificity rules apply when a distinct skin condition needs its own code rather than a generic placeholder.
Need infection control counseling in the record? HIPAA compliance for medical offices covers the documentation standards that make patient education and infection control notes audit-ready for B86 claims.
Choosing a platform for a dermatology practice? Our roundup of the best dermatology EHR software compares tools that combine clinical documentation and claims management in one workflow.
ICD-10 Code B86 is the billable, specific ICD-10-CM diagnosis code for scabies, a contagious skin infestation caused by the mite Sarcoptes scabiei. It is classified under Chapter 1 (Certain infectious and parasitic diseases) within the B85-B89 block covering pediculosis, acariasis and other infestations. B86 covers all scabies presentations including crusted (Norwegian) scabies and sarcoptic itch under a single code with no subcategory options.
Yes. B86 is a fully billable, specific ICD-10-CM code and has been billable since ICD-10-CM was implemented in 2015. There are no subcategory codes beneath it. Teams should always verify they are referencing the current fiscal year tabular list when coding scabies encounters to ensure no updates have been made.
Crusted scabies (also called Norwegian scabies) is a severe hyperinfestation seen primarily in immunocompromised patients, characterized by thick crusted plaques and very high mite burdens. It is still coded as B86 in ICD-10-CM; there is no separate subcategory for crusted versus classic scabies. Providers should document the presentation explicitly in the clinical note to support the level of management provided.
B86 is paired with E/M CPT codes appropriate to the setting and complexity of the encounter. Common pairings include 99202-99215 for outpatient office visits and 99281-99285 for emergency department presentations. The CPT level is determined by documented medical decision making or time, not by the diagnosis code itself.
B86 (Scabies) is specific to infestations caused by Sarcoptes scabiei, while B88.0 (Other acariasis) covers acariasis from other mite species such as Demodex and unspecified mite infestations. If the provider documents confirmed scabies or sarcoptic itch, use B86. B88.0 applies only when the causative mite is confirmed to be a species other than Sarcoptes scabiei or when the mite species is unspecified.
Sarcoptic itch is the official “Applicable To” synonym listed in the ICD-10-CM tabular under B86. It describes the intense pruritic reaction caused by Sarcoptes scabiei infestation and maps directly to B86 with no separate code required. When a provider documents “sarcoptic itch” as the diagnosis, report B86.