CPT code 00103: Anesthesia for eyelid reconstruction billing guide
CPT code 00103 is the anesthesia code for reconstructive procedures on the eyeli...
July 23, 2026
CPT code 99283 is the Level 3 emergency department E/M code. Under the 2023 AMA descriptor, it applies when an ED visit requires a medically appropriate history and/or examination and low medical decision making (MDM). It is billed with Place of Service 23 and selected by MDM, not time.
CPT Code 99283 covers emergency department visits requiring a medically appropriate history and/or examination plus low medical decision making (MDM), per 2023 AMA guidelines.
The 2023 AMA revision changed the MDM requirement from moderate to low complexity, making 99283 the Level 3 ED code for conditions with a low risk of morbidity.
CPT 99283 is restricted to Place of Service 23 (emergency department); urgent care centers using POS-20 or POS-22 must use outpatient E/M codes such as 99214 instead.
Pabau’s claims management software helps ED billing teams document 99283 encounters accurately, reducing claim denials caused by incomplete MDM documentation.
Most ED claim denials at Level 3 trace back to one misunderstanding: coders still apply the pre-2023 MDM threshold to CPT Code 99283. Since January 2023, the American Medical Association’s CPT code set defines 99283 as requiring low medical decision making, not the moderate complexity that older resources still cite.
The official 2023 AMA descriptor reads: “Emergency department visit for the evaluation and management of a patient, which requires a medically appropriate history and/or examination and low medical decision making.” This article covers the documentation requirements, reimbursement rates, modifier rules, and the facility-versus-professional billing distinctions that affect 99283 claims in 2026.
Before 2023, selecting between ED E/M codes relied on three key components: history, examination, and MDM. The American College of Emergency Physicians (ACEP) confirmed that the 2023 AMA revision eliminated history and physical as stand-alone determinants for code selection. They are now documented only when “medically appropriate,” not to justify the code level.
For CPT Code 99283 specifically, this created two important shifts. Code selection now rests on the level of MDM alone: unlike office visit codes, the ED E/M codes (99281-99285) are not reported by time, so total time cannot be used to pick the level. The history and physical still need to be documented, but they no longer drive code selection.
| Criterion | Pre-2023 rule | Post-2023 rule |
|---|---|---|
| Code selection basis | History + Exam + MDM (all three) | MDM alone (time not used for ED codes) |
| MDM complexity | Moderate | Low |
| History/Exam role | Required key component | Medically appropriate (documented but not determinative) |
| New vs. established patient | Not differentiated | Not differentiated (no change) |
One point worth flagging: some older payer contracts and legacy EHR templates were built around the three-component framework. Billing teams should verify their EHR integration and charge-capture workflows reflect the post-2023 rules before submitting 99283 claims.
Low MDM is the clinical threshold that separates 99283 from 99282 (straightforward MDM) below it and 99284 (moderate MDM) above it. The AMA defines low MDM across three elements: the number and complexity of problems addressed, the amount and/or complexity of data reviewed, and the risk of complications and/or morbidity or mortality.
At the low MDM level, 99283 applies when the clinician addresses one or more self-limited or minor problems, or one stable chronic illness. Typical presentations include a laceration requiring closure, an uncomplicated UTI, a mild asthma exacerbation responding to a single bronchodilator treatment, or a closed extremity fracture without neurovascular compromise.
Low MDM requires limited data review. This could mean reviewing a limited number of tests ordered during the encounter, reviewing external records relevant to the presenting problem, or ordering and reviewing the result of one or two ancillary tests. Extensive multi-system data review, specialist consultation, or independent interpretation of imaging pushes the encounter toward moderate or high MDM.
For 99283, the risk level is low. The presenting problem carries a low risk of morbidity without treatment and a low probability of complications from the management plan. Prescription drug management, minor surgical procedures with no identified risk factors, and over-the-counter medications are consistent with this risk tier.
Document the specific risk level explicitly in the clinical note. Stating ‘low risk of morbidity, treated with prescription antibiotic and discharge instructions’ gives coders and auditors a clear MDM anchor. Vague phrases like ‘patient doing well’ leave the MDM tier open to interpretation and increase denial risk.
Accurate documentation is the front line of defense against 99283 denials. The HIPAA-compliant documentation requirements for 99283 break into three areas: clinical content, MDM substantiation, and time (when time-based billing is used).
The note must clearly support low MDM. Reviewers look for the number of problems addressed, the data reviewed (labs ordered, imaging interpreted, records reviewed), and the management risk. Notes that list a diagnosis without explaining the thought process behind it fail MDM documentation standards. Structured clinical documentation tools, including clinical documentation workflows built into practice management systems, reduce this risk significantly.
Unlike office and other outpatient E/M codes, the emergency department codes 99281-99285 are not selected on time. The AMA and the American College of Emergency Physicians (ACEP) confirm that time is not a descriptive component for ED E/M services, so 99283 must be chosen on the level of medical decision making. You may still document total encounter time for productivity or medico-legal reasons, but base the code itself on MDM. Because time is not a factor, the prolonged-service add-ons used with time-based office visits — such as CPT code 99358 (prolonged service) — cannot be appended to 99283.
Reimbursement for CPT Code 99283 varies by payer, geography, and facility type. The CMS Physician Fee Schedule is the reference point for Medicare rates, which then form the baseline for most commercial payer negotiations.
Under the 2026 Medicare Physician Fee Schedule, CPT Code 99283 carries roughly 2.11 total RVUs (1.60 work RVUs), which works out to a national professional payment of approximately $70 before geographic adjustment. Locality adjustments move this figure up or down, so verify the exact amount for your locality with the CMS Physician Fee Schedule lookup tool. Because emergency services are hospital-based, the facility and non-facility professional values are effectively the same, while hospitals bill the institutional rate separately through the hospital outpatient prospective payment system (OPPS).
| Billing scenario | Who bills | Payment basis | Approximate Medicare rate (2026) |
|---|---|---|---|
| Professional (physician) | ED physician or group | MPFS national rate | ~$70 (locality-adjusted) |
| Facility (hospital ED) | Hospital | OPPS APC payment | Separate APC rate (varies) |
| Commercial payer | Physician or facility | Negotiated contract rate | Varies by contract |
Always verify current rates directly through the CMS fee schedule lookup tool, as rates change annually. Commercial payer rates for 99283 may differ substantially from Medicare, and major payers including Blue Cross Blue Shield entities and Molina Healthcare maintain their own coverage and reimbursement policies. Using claims management software to track payer-specific rates prevents undercoding and overcoding errors.
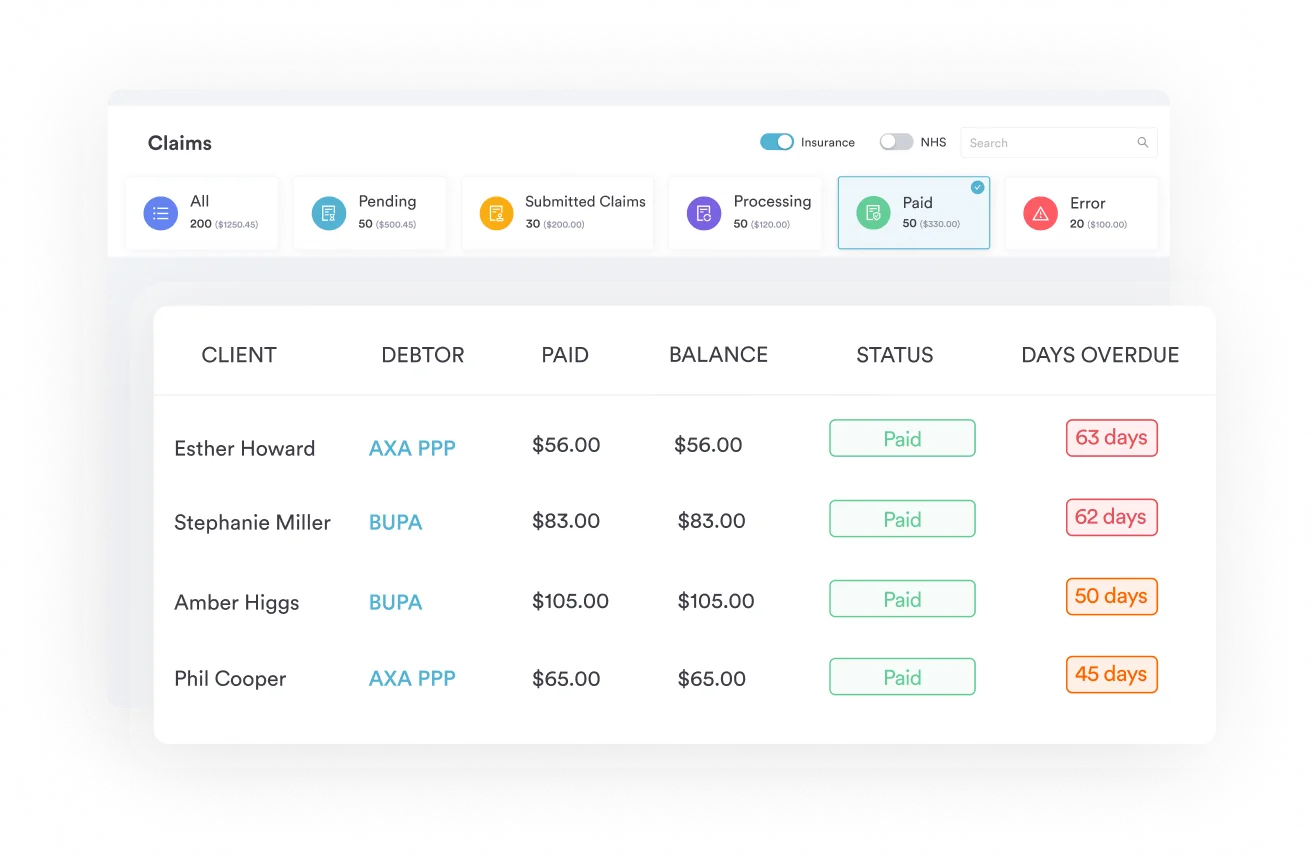
Pabau's claims management tools help emergency and urgent care billing teams build accurate, auditable records for every E/M level. See how structured documentation reduces denials.

This distinction causes more confusion than almost any other aspect of ED billing. The same patient encounter generates two separate claims: one from the physician (professional bill) and one from the hospital (facility bill). They follow different rules and different payment systems.
The ED physician or physician group submits the professional claim using CPT Code 99283 with Place of Service 23. Payment comes from the Medicare Physician Fee Schedule or the applicable commercial contract. The physician’s note drives MDM-based code selection. Revenue cycle teams managing professional billing should integrate charge capture into their practice management software to flag documentation gaps before submission.
The hospital submits a UB-04 claim. For Medicare patients, the ED visit is paid through the OPPS under an Ambulatory Payment Classification (APC) group, not the MPFS. Facility E/M level selection may follow different internal criteria (often nursing-based criteria or facility-specific tools) rather than physician MDM alone. An AAPC forum discussion confirmed that Modifier 25 is generally not required on facility claims when procedures like X-rays are billed alongside 99283, because X-rays are not classified as significant procedures in that context.
Modifier usage with 99283 depends on the clinical circumstance and the billing environment (professional vs. facility). The most common modifiers are listed below, along with their appropriate use cases. Refer to documentation features that save billing teams time when verifying modifier requirements across payer-specific rules.
Modifier 25 carries the highest audit risk. CMS and most commercial payers scrutinize it closely when it appears with procedure codes on the same claim. The supporting documentation must clearly show that the E/M service was performed above and beyond what the procedure itself required.
ED coders who mis-level between 99282, CPT Code 99283, and 99284 are leaving money on the table or creating audit exposure. The MDM tier is the primary differentiator after the 2023 AMA guideline changes.
| Code | MDM level | Typical presentation | Risk tier |
|---|---|---|---|
| 99281 | May not require physician presence | Simple injury, minor laceration (nurse-only evaluation) | Minimal |
| 99282 | Straightforward | Simple complaint, single problem, OTC medication management | Minimal-Low |
| 99283 | Low | UTI, closed fracture, mild asthma exacerbation, laceration repair | Low |
| 99284 | Moderate | Chest pain requiring workup, abdominal pain with imaging, CVA evaluation | Moderate |
| 99285 | High | Sepsis, acute MI, multi-system trauma, altered mental status | High |
The most common mis-leveling error is coding 99283 when the encounter warrants 99284. Chest pain presentations, for example, often involve multiple diagnoses considered, imaging interpretation, and IV drug management, all of which push MDM toward moderate. Coders reviewing ED charts should use a structured MDM scorecard rather than relying on chief complaint alone. Building this into medical practice management software workflows catches the error before submission.
When a patient presents with chest pain and the physician orders a troponin, EKG, and chest X-ray, and then considers multiple diagnoses, the data complexity alone may support moderate MDM, pushing the encounter to 99284. Do not default to 99283 for chest pain without reviewing the data and risk elements first.
CPT Code 99283 is restricted to Place of Service 23 (emergency department). This is not a technicality. Molina Healthcare’s provider policy explicitly states that ED E/M codes require POS-23, and the Journal of Urgent Care Medicine has confirmed that urgent care centers using POS-20 (urgent care facility) or POS-22 (outpatient hospital) must use outpatient E/M codes such as 99214, not 99283.
Freestanding emergency departments that bill with POS-23 can use 99283 for qualifying encounters. The setting is what controls the code family, not the acuity or the name on the door. Practices managing hybrid urgent-care-and-ED settings should build payer-specific POS rules into their automated billing workflows to prevent POS mismatches at claim submission.
Claim denials for 99283 cluster around a predictable set of documentation and coding errors. Addressing these proactively, before submission, is far less costly than working a denial queue. Consider improving patient scheduling and workflow documentation as a foundation for cleaner claims.
Revenue cycle teams using integrated practice management platforms that connect clinical documentation to billing charge capture see fewer of these errors because the note and the claim draw from the same structured data source. Manual transcription between systems is where most 99283 errors originate.
Emergency department billing teams deal with high volume, time pressure, and documentation requirements that change with every AMA guideline revision. Pabau’s claims management software connects clinical note-taking directly to billing workflows, reducing the manual handoff where most 99283 errors occur.
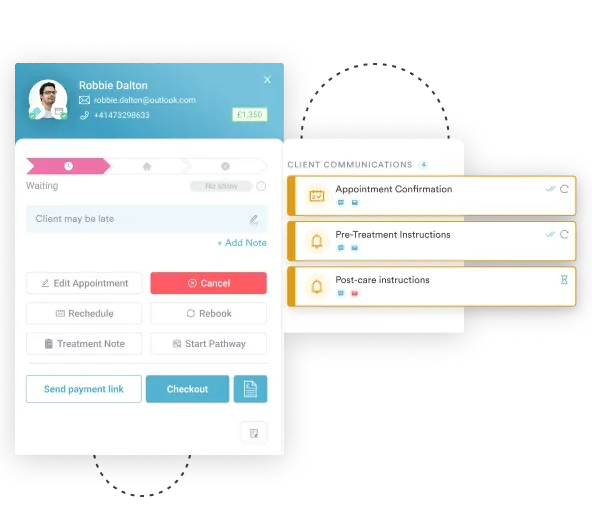
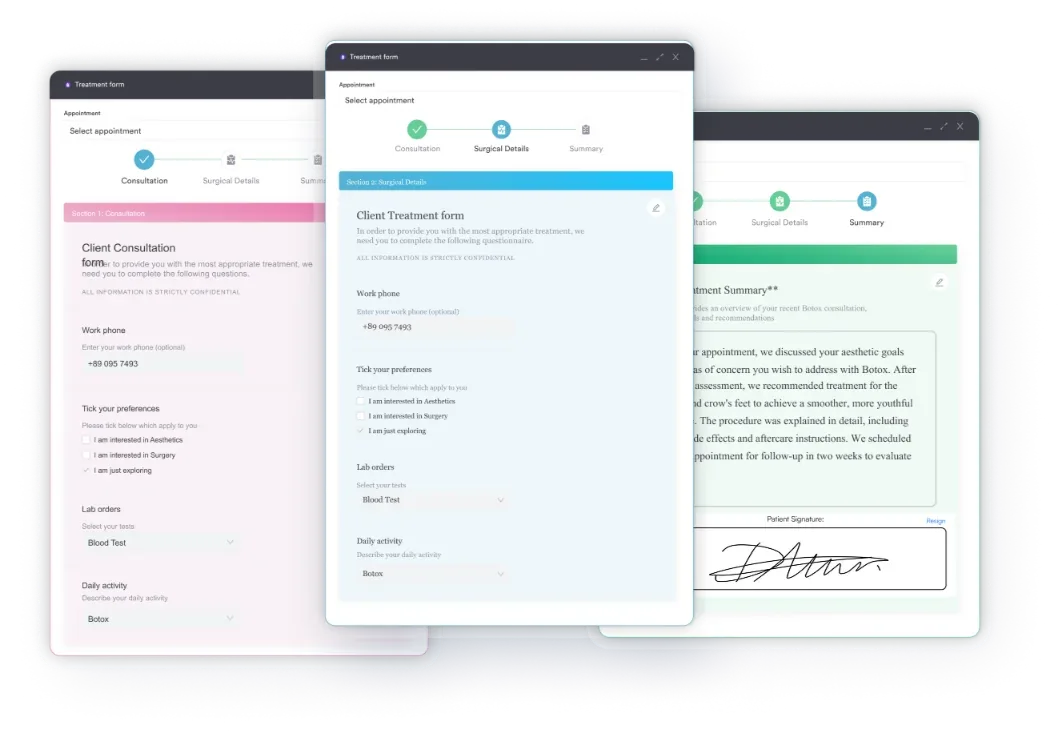
Practices using Pabau can build structured encounter templates that prompt physicians to document MDM elements explicitly, including the number of problems addressed, the data reviewed, and the risk level. The platform also supports digital intake forms that capture structured clinical data at the point of care, reducing the back-and-forth between providers and coders during charge reconciliation. For teams managing clinical documentation burden, structured templates also reduce cognitive load on physicians at end-of-shift documentation time.
CPT Code 99283 is one of the most commonly billed ED codes, and also one of the most frequently denied due to documentation gaps. The 2023 AMA guideline changes shifted the MDM requirement to low complexity and eliminated history and physical as stand-alone code determinants, but many billing workflows have not fully caught up.
Getting 99283 right consistently requires structured MDM documentation, accurate place of service assignment, and modifier discipline around Modifier 25. Pabau’s claims management and structured documentation tools give billing teams the workflow infrastructure to build these checks into every encounter, reducing denials before they happen. To see how Pabau supports accurate E/M coding at scale, book a demo.
Need to understand how practice management software handles billing workflows? How practice management software streamlines billing walks through the core functions that connect clinical documentation to claim submission.
Looking to reduce admin burden on your clinical team? Features that save private practices time on documentation covers the tools that cut manual data entry in billing and scheduling workflows.
Want to explore related CPT coding references? CPT coding guides for related specialties covers other commonly billed procedure codes alongside clinical documentation best practices.
CPT Code 99283 is an emergency department evaluation and management code used when a patient visit requires a medically appropriate history and/or examination along with low medical decision making (MDM), per the 2023 AMA descriptor. It applies regardless of whether the patient is new or established, since ED E/M codes do not differentiate by patient status.
The difference is MDM complexity. CPT 99283 requires low MDM, while CPT 99284 requires moderate MDM. Encounters with multiple diagnoses considered, imaging interpretation, or IV drug management typically support moderate MDM and should be billed as 99284, not 99283. Undercoding to 99283 when the chart supports 99284 leaves reimbursement on the table.
Not routinely. CPT 99283 does not require a modifier for standard ED encounters. Modifier 25 is added only when a significant, separately identifiable procedure is billed on the same claim and a separate E/M service is documented. Verify payer-specific modifier requirements before applying Modifier 25, as incorrect use is a common audit trigger.
No. CPT Code 99283 is restricted to Place of Service 23 (emergency department). Urgent care centers using POS-20 or POS-22 must use outpatient office E/M codes such as 99214 for equivalent complexity encounters. Only facilities designated as emergency departments and billing under POS-23 can use the 99281-99285 code family.
The 2026 Medicare national professional rate for CPT Code 99283 is approximately $70 (about 2.11 total RVUs), subject to geographic locality adjustments. Facility rates are paid separately under the OPPS system and differ from professional rates. Commercial payer rates vary by contract and can be significantly higher or lower than Medicare.
Low MDM is required, per the 2023 AMA revision. This means the encounter involves a limited number of diagnoses or management options, limited data review, and a low risk of complications or morbidity. Encounters warranting prescription drug management for a single acute problem, or interpretation of a single ancillary test, often meet the low MDM threshold for 99283.