Apathy evaluation scale (AES): Scoring guide and free template
Download your free apathy evaluation scale Apathy evaluation scale A ready-to-us...
July 21, 2026
A bipolar disorder nursing care plan is a structured clinical document that guides psychiatric nurses through assessment, diagnosis selection, intervention planning, and outcome evaluation for patients in manic, depressive, or mixed mood states.
NANDA diagnoses for bipolar disorder include Risk for Injury, Ineffective Coping, Disturbed Sleep Pattern, and Impaired Social Interaction, each requiring specific interventions and outcome measures.
Medication monitoring is central to nursing care – lithium requires serum level checks (therapeutic range 0.6-1.2 mEq/L maintenance), and antipsychotics need metabolic syndrome screening.
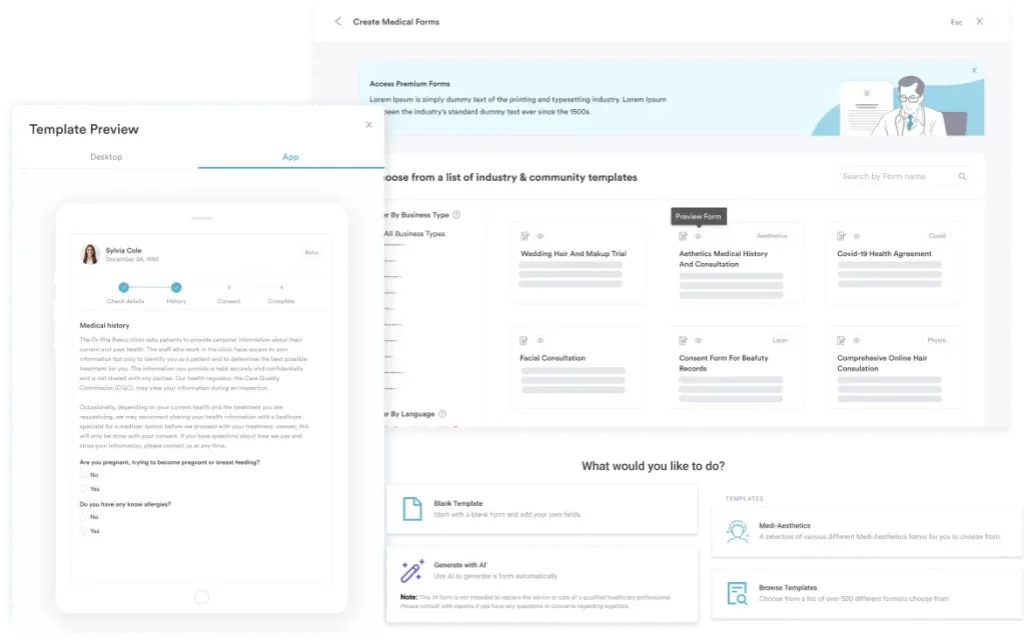
Practice management software like Pabau brings digital forms and structured client records together, so psychiatric teams can track mood episodes, medication responses, and safety assessments in one place.
A ready-to-use template covering psychiatric history assessment, NANDA diagnoses, nursing interventions for mood episodes, medication monitoring protocols, expected patient outcomes, and family education frameworks.
Download templateA comprehensive bipolar disorder nursing care plan provides the structured framework psychiatric nurses need to manage complex mood episodes and guide patient care across acute, maintenance, and relapse-prevention phases. This template equips clinicians with evidence-based tools to assess manic and depressive presentations, select appropriate NANDA diagnoses, deliver targeted interventions, and measure meaningful patient outcomes.
A bipolar disorder nursing care plan is a clinical document that translates the nursing process (ADPIE: Assessment, Diagnosis, Planning, Implementation, Evaluation) into actionable care guidance for patients diagnosed with Bipolar I Disorder, Bipolar II Disorder, or Cyclothymic Disorder. The plan addresses the patient’s immediate safety needs, mood stabilization goals, medication adherence, sleep hygiene, psychosocial stressors, and family involvement in recovery.
Care planning in psychiatry must account for the episodic nature of bipolar disorder. A single manic episode can escalate to dangerous impulsivity and risk-taking; untreated depression can drive suicidal ideation. The nursing care plan serves as the clinical bridge between psychiatric assessment and day-to-day interventions, ensuring consistent monitoring and rapid response to symptom changes.
Under DSM-5-TR and ICD-10 diagnostic criteria, nurses document the specific presentation—manic, hypomanic, depressive, mixed, or unspecified—and adjust the care plan accordingly. Legal and regulatory bodies including the American Psychiatric Nurses Association (APNA) and the American Nurses Association (ANA) mandate that psychiatric care plans meet documentation standards for patient safety, informed consent, and continuity of care.
A structured care plan template guides clinicians through a five-step workflow designed to capture critical assessment data, select evidence-based diagnoses, and track outcomes over time.
Digital clinical forms and structured templates streamline this workflow by auto-populating fields, enforcing compliance with documentation standards, and enabling real-time care team collaboration.
Psychiatric nurses and mental health nurse practitioners working in inpatient units, partial hospitalization programs, intensive outpatient programs (IOPs), community mental health centers, and private psychiatric practices all rely on standardized care plans to ensure safe, evidence-based care. The template is equally essential for registered nurses (RNs) transitioning into mental health specialties and for experienced psychiatric nurses managing complex cases with multiple comorbidities.
Facility-based teams benefit from the consistency a template provides: it reduces care fragmentation during shift changes, ensures all clinicians assess the same safety risks, and creates a legal record that meets Joint Commission inpatient psychiatric standards. Private practice clinicians and therapists use simplified versions to track mood patterns and medication responses between psychiatric appointments.
Safety and risk management. A structured care plan ensures systematic assessment of suicidal ideation, self-harm risk, and dangerous impulsivity. Nurses document safety interventions (e.g. 1:1 observation, restricted access to harmful items) with clear rationales tied to patient risk factors.
Medication monitoring compliance. Templates enforce documentation of lithium serum levels (maintained at 0.6-1.2 mEq/L), renal and thyroid function tests, and metabolic syndrome screening for antipsychotics. This prevents dangerous drug interactions and toxicity.
Continuity across episodes. Because bipolar disorder spans manic, depressive, and maintenance phases, a longitudinal care plan template documents the patient’s baseline mood, triggers, medication responses, and relapse patterns. This historical data speeds diagnosis and intervention when episodes recur.
Regulatory compliance. Documentation standards set by CMS, Joint Commission, and state nursing boards require that psychiatric care plans address specific domains: psychiatric history, assessment findings, nursing diagnoses, interventions, and measurable outcomes. A template ensures compliance.
Nursing care plans that leverage automated workflows and care coordination tools reduce manual documentation time, allowing clinicians to focus on direct patient care.
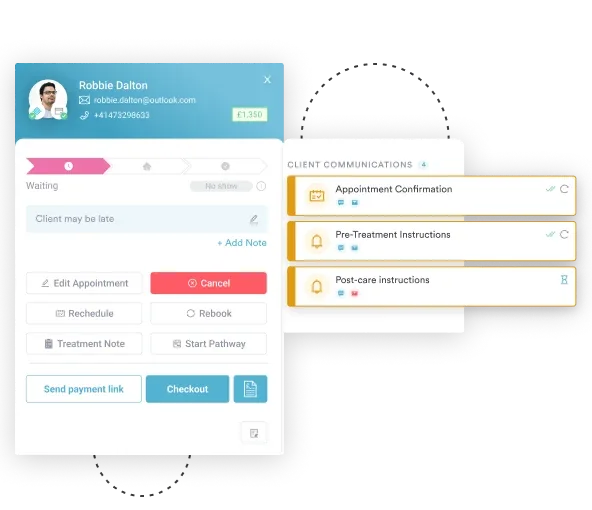
From intake assessment through medication tracking and family education, Pabau's digital forms and client records keep psychiatric care plans organized, accessible, and compliant.

A thorough psychiatric assessment forms the foundation of the nursing care plan. Nurses gather data across multiple domains: present mood and affect, recent mood episodes (onset, triggers, severity, duration), medications and adherence history, substance use, medical comorbidities, suicide and harm risk, cognitive and functional status, family psychiatric history, and psychosocial stressors (job loss, relationship conflict, financial strain).
Risk assessment tools such as the Columbia Suicide Severity Rating Scale (C-SSRS) and the Beck Scale for Suicide Ideation quantify suicidal risk and guide safety interventions, while standardized scales like the Beck Depression Inventory track depressive symptom severity over time. Clinicians also assess past coping mechanisms, social support, and previous responses to treatment.
Documentation using structured psychiatric evaluation frameworks ensures that no critical domain is missed and that assessment data directly informs diagnosis selection and intervention planning.
Once assessment data is in front of you, the next step is matching each finding to a bipolar disorder nursing diagnosis and the interventions that address it. The table below turns the most common NANDA-I diagnoses into a lift-ready care plan. Each row pairs the diagnosis with the assessment cue behind it, a measurable goal, and the nursing interventions for bipolar disorder that follow, with the rationale spelled out.
| NANDA nursing diagnosis | Assessment cue (related to) | Goal / expected outcome | Key nursing interventions and rationale |
|---|---|---|---|
| Risk for injury | Manic hyperactivity, impulsivity, poor judgment | Patient stays free from injury throughout admission | Lower stimulation with a quiet, low-lit room, remove hazardous items, and set consistent limits. Fewer triggers give escalating energy less to act on. |
| Risk for self-directed violence | Depressive hopelessness, suicidal ideation | Patient reports no suicidal intent and agrees to a safety plan | Screen with the Columbia Suicide Severity Rating Scale each shift and move to 1:1 observation when risk climbs. Frequent contact catches intent before it becomes action. |
| Disturbed sleep pattern | Manic agitation and reduced need for sleep | Patient sleeps at least six hours a night within one week | Cluster care to protect rest and cut caffeine and evening stimulation. Sleep loss both signals and fuels mania, so restoring it stabilizes mood. |
| Ineffective coping | Mood dysregulation and low frustration tolerance | Patient uses two healthy coping strategies by discharge | Keep communication calm and brief, and teach grounding and trigger identification. Predictable interactions lower reactivity. |
| Imbalanced nutrition: less than body requirements | Too distracted to eat in mania, appetite loss in depression | Patient maintains weight and takes adequate fluids | Offer portable, high-calorie finger foods during mania and track intake alongside lithium and sodium balance, since dehydration raises lithium toxicity risk. |
| Impaired social interaction | Intrusive grandiosity in mania or withdrawal in depression | Patient joins one structured group activity appropriately | Start with brief one-to-one contact and grade up to structured groups. Matching social demands to the current mood prevents both overstimulation and isolation. |
This is the same NANDA nursing diagnosis for bipolar disorder framework the downloadable template expands on, with space to record patient-specific cues and evaluation dates. Whether the documentation calls it a bipolar mood disorder nursing diagnosis or a bipolar affective disorder diagnosis, the assessment-to-outcome logic stays the same.
An acute manic episode reorders these priorities around safety and physical stability. The nursing interventions for bipolar disorder mania focus on reducing stimulation, protecting sleep, and keeping the patient nourished and hydrated while mood stabilizers take effect. Redirect excess energy into low-stimulation activities rather than confronting grandiose behavior, and document the response to each dose so the team can adjust quickly if agitation persists.
Medication management is inseparable from bipolar disorder nursing care. Mood stabilizers (lithium, valproate, lamotrigine) and atypical antipsychotics (aripiprazole, quetiapine, lurasidone) form the backbone of treatment, but each carries specific monitoring requirements that the nursing care plan must document.
Lithium requires serum level monitoring (therapeutic range 0.6-1.2 mEq/L maintenance), baseline and periodic renal and thyroid function tests, and patient education on sodium and fluid balance. Antipsychotics demand metabolic monitoring including weight, lipid panel, fasting glucose, and prolactin levels due to metabolic syndrome risk.
The care plan documents medication administration schedules, side effect monitoring (akathisia, tardive dyskinesia, weight gain), and contraindications. Antidepressants require caution in bipolar disorder because monotherapy can trigger mood switching, so distinguishing bipolar depression from unipolar major depression is essential; nursing notes must track any mood destabilization.
Safety is the highest-priority nursing domain in bipolar care. During manic episodes, patients may engage in reckless spending, unsafe sexual behavior, substance abuse, or dangerous driving. During depression, suicidal ideation and self-harm intent escalate risk. The care plan documents specific safety measures: 1:1 observation levels, access restrictions, physical environment modifications, and de-escalation techniques.
Proactive crisis intervention planning empowers patients to recognize their own prodromal symptoms (sleep loss, racing thoughts, sudden mood shifts) and contact their care team before hospitalization becomes necessary. The care plan includes a written crisis plan with emergency contact numbers, hospitalization triggers, and patient-identified coping strategies.
Psychoeducation is a cornerstone of relapse prevention. Patients and families benefit from clear, accessible information about bipolar disorder biology, medication side effects, sleep hygiene importance, stress management, substance avoidance, and early warning signs of mood episodes. The care plan dedicates specific interventions to education delivery and comprehension checks.
Family sessions foster understanding of bipolar disorder as a medical illness (not a character flaw), clarify boundaries during episodes, and strengthen communication. The nursing care plan documents informed consent and family engagement frameworks to support long-term stability.
Once acute symptoms stabilize, the nursing care plan transitions to maintenance-phase focus: preventing relapse, supporting medication adherence, managing triggers, and building psychosocial resilience. Nurses track mood patterns using mood diaries or digital tracking tools, identify situational triggers (seasonal changes, sleep disruption, relationship stress), and reinforce self-care routines.
Long-term care coordination with psychiatrists, therapists, primary care providers, and outpatient teams ensures continuity. A written relapse prevention plan given to the patient includes warning signs, coping strategies, and clear steps for reaching emergency services.
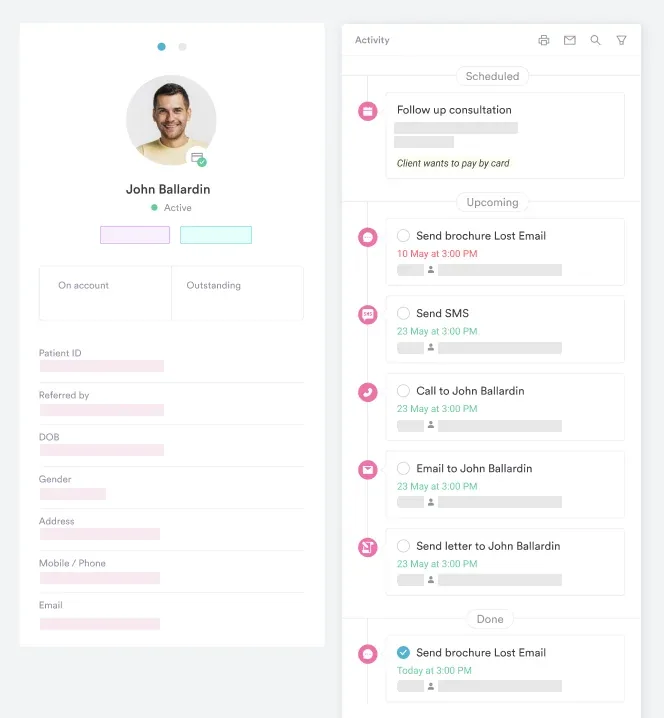
Using digital client records enables psychiatric teams to quickly access a patient’s full mood history, past episodes, medication trials, and response patterns, accelerating diagnosis and intervention when early warning signs emerge.
Qualitative research identifies barriers to effective bipolar disorder nursing care: inadequate time, understaffing, lack of specialized training, inconsistent documentation, and burnout. Standardized care plan templates mitigate these obstacles by reducing time spent on documentation structure, enforcing consistency across clinicians, and providing decision support.
A well-designed template serves as both a clinical guide and a teaching tool, enabling newer psychiatric nurses to deliver evidence-based interventions while more experienced clinicians can rapidly customize plans for complex cases. Practice management systems that integrate care planning workflows further reduce administrative burden.
The nursing care plan does not stand alone. It is one component of integrated care that includes psychiatric evaluation, psychotherapy (CBT, DBT, family therapy), vocational rehabilitation, substance abuse treatment if needed, and medical management of comorbidities. Nursing care coordinates across all modalities, ensuring the patient receives cohesive, team-based treatment.
Psychiatric practice management systems that support integrated care planning allow nurses, psychiatrists, therapists, and care coordinators to document within a shared record, reducing silos and accelerating response to clinical changes.
A comprehensive bipolar disorder nursing care plan is essential infrastructure for psychiatric practice. Whether delivered in hospital units, outpatient clinics, or community mental health settings, a well-constructed template ensures safety, guides clinicians through the nursing process, supports medication compliance, and empowers patients and families in long-term mood management. Organizations that prioritize structured care planning with integrated telehealth and documentation tools see measurable improvements in treatment adherence and relapse prevention outcomes.
Bipolar disorder demands vigilant, consistent nursing care across acute episodes and maintenance phases. A structured nursing care plan template provides the framework—assessment domains, NANDA diagnoses, measurable outcomes, and evidence-based interventions—that turns clinical knowledge into actionable care. Download the template above to establish this critical foundation for your psychiatric nursing practice.
Need a way to manage and track care plans across your team? Book a demo with Pabau to see how digital care coordination and automated workflows can reduce documentation time and improve patient outcomes.
Looking for a broader mental health template? Psychiatric Evaluation Template provides the foundational assessment framework that precedes nursing care planning.
Need to document crisis protocols? Crisis intervention strategies for clinicians outlines evidence-based de-escalation and safety responses.
Supporting family involvement? Healthcare provider burnout prevention strategies help psychiatric teams sustain the compassion required for long-term patient relationships.
A psychiatric evaluation is the initial assessment and diagnosis document completed by a psychiatrist or psychiatric nurse practitioner. A nursing care plan is the operational document that follows, outlining specific nursing diagnoses, patient-centered goals, and day-to-day interventions based on that evaluation.
Care plans are reviewed and updated weekly during acute hospitalization or intensive outpatient care, and at each outpatient appointment (typically monthly or quarterly in stable maintenance phase). Any significant change in mood, medication, or safety status triggers immediate plan revision.
The most frequently used diagnoses are Risk for Injury (manic impulsivity), Ineffective Coping (mood dysregulation), Disturbed Sleep Pattern (manic agitation or depressive lethargy), Impaired Social Interaction (withdrawn or hypersocial behavior), and Risk for Self-Directed Violence (depressive suicidal ideation).
Core domains are similar (assessment, diagnosis, goals, interventions, outcomes), but acuity level differs. Inpatient plans emphasize safety and acute symptom management; outpatient plans prioritize maintenance, relapse prevention, and functional recovery. Templates can be adapted to each setting.
Yes. Most treatment settings share a simplified, patient-friendly summary of goals and interventions with the patient and, with consent, family members. Full clinical documentation remains in the medical record under HIPAA privacy protections.
Care plans integrate findings from psychiatric nursing research, APNA clinical guidelines, and DSM-5-TR diagnostic standards. Regular review of current literature ensures interventions reflect best practice, medication monitoring aligns with pharmacology evidence, and safety protocols match current risk assessment science.
Core actions include keeping the patient safe through observation and a low-stimulation environment, monitoring mood-stabilizer levels and side effects, protecting sleep, supporting nutrition and hydration, and using calm, consistent therapeutic communication. The emphasis shifts between manic and depressive presentations.
The free template at the top of this page downloads as a ready-to-use document covering psychiatric assessment, NANDA diagnoses, goals, interventions, and family education, so you can build a plan for a specific patient instead of starting from a blank page.