ICD-10 Code L88: Pyoderma gangrenosum coding reference
L88 is the billable ICD-10-CM code for pyoderma gangrenosum. One Excludes1 note ...
Last Updated: August 4, 2026
ICD-10 Code N72 is the billable FY2026 diagnosis code for inflammatory disease of cervix uteri, covering cervicitis, endocervicitis, and exocervicitis with or without erosion or ectropion.
Pair N72 with a B95-B97 infectious agent code only when the organism lacks its own combination code — organisms like gonorrhea, herpes, and chlamydia have dedicated combination codes (A54.03, A60.03, A56.09) that take priority over N72 plus B95-B97.
N72 has Excludes1 conditions that prevent simultaneous assignment; verify the tabular list before coding any related cervical or pelvic condition.
Pabau’s claims management software and digital intake forms help gynecology practices document N72 encounters accurately and reduce claim errors.
ICD-10 Code N72 is the FY2026 billable diagnosis code for inflammatory disease of the cervix uteri, covering cervicitis, endocervicitis, and exocervicitis with or without erosion or ectropion. It carries a mandatory “use additional code” instruction: pair N72 with a B95-B97 code when the infectious agent is identified, unless that organism has its own combination code instead.
N72 sits within Chapter 14 of ICD-10-CM (Diseases of the Genitourinary System, N00-N99), specifically in the N70-N77 subsection covering inflammatory diseases of female pelvic organs. It is a single-code category with no further specificity subdivisions, which makes the infectious agent code pairing the primary complexity coders and clinicians need to manage.
This reference covers the official includes notes, Excludes1 restrictions, B95-B97 pairing rules, related codes, documentation requirements, and practical billing guidance for OB/GYN practice management and women’s health practices.
The official ICD-10-CM Includes note for N72 lists three distinct anatomical presentations, all of which map to this single code:
The parenthetical “with or without erosion or ectropion” is clinically significant. Cervical erosion or ectropion found incidentally alongside active inflammation does not require a separate code; the presence of the inflammatory process subsumes the structural finding under N72.
Accepted synonyms in the ICD-10-CM index that map to this code include acute cervicitis, acute endocervicitis, acute on chronic cervicitis, and chronic cervicitis. Coders searching by any of these terms should verify they land on N72 before assigning.
All three conditions fall under N72, but the clinical distinction matters for documentation. Cervicitis is a broad term for cervical inflammation. Endocervicitis specifically involves the endocervical canal and glandular epithelium; it is more commonly associated with ascending infections like chlamydia and gonorrhea. Exocervicitis involves the ectocervix and squamous epithelium, more often linked to HPV, herpes simplex, or contact irritation.
The clinical note should specify which presentation is present. This supports accurate infectious agent coding and strengthens medical necessity documentation for any associated treatment or testing.
The single most important coding instruction attached to N72 is this: use an additional code from B95-B97 to identify the infectious agent. This instruction is mandatory when the causative organism is documented or confirmed by laboratory testing.
The B95-B97 block covers bacterial, viral, and other infectious agents as the cause of diseases classified elsewhere. Relevant codes for cervicitis include:
When the organism is unknown or testing is pending, assign N72 alone and update the claim if lab results arrive before the claim submission window closes. Do not assign a B95-B97 code speculatively.
For sexual health clinics managing high volumes of STI-related cervicitis, building a structured laboratory results workflow into the patient record reduces the risk of submitting claims before infectious agent confirmation is available. According to CMS ICD-10-CM coding guidance, the “use additional code” instruction signals that the additional code should be sequenced after the primary condition code.
N72 carries an Excludes1 note, meaning certain conditions cannot be coded simultaneously with N72 under any circumstance. Excludes1 is a hard restriction: if the Excludes1 condition is what the patient actually has, assign that code instead of N72.
Conditions in the Excludes1 note for N72 include erosion and ectropion of the cervix without cervicitis. The critical distinction: cervical erosion or ectropion occurring as an incidental structural finding in the absence of active inflammation is not coded to N72.
Those presentations are coded to N86 instead of N72. The includes note for N72 makes clear that erosion and ectropion are included only with the inflammatory process, not as standalone findings.
Understanding where N72 ends and adjacent codes begin prevents upcoding and downcoding errors. Three codes are frequently confused with N72:
For charts documenting pelvic inflammatory disease (PID) that extends beyond the cervix, review whether N70-N77 codes for salpingitis or oophoritis are also warranted. Cervicitis documented as the portal of entry for ascending PID may be coded alongside the more specific PID code, depending on the clinical note and attending physician documentation.
Always verify against the CDC/NCHS ICD-10-CM web tool to confirm current tabular list instructions before assigning.
Before assigning N72, run a quick three-point check: (1) Is cervicitis, endocervicitis, or exocervicitis explicitly documented in the clinical note? (2) Is the infectious agent confirmed or identified? If yes, select the matching B95-B97 code. (3) Does the note describe erosion or ectropion without inflammation? If so, the correct code is N86, not N72. Building this check into your charge capture or EHR workflow takes two minutes and eliminates the most common N72 denial pattern.
Payers reviewing N72 claims look for three documentation elements: the clinical basis for the diagnosis, the site and acuity of inflammation, and the infectious agent or rationale for unknown etiology.
At minimum, the clinical note supporting an N72 claim should include the presenting symptoms, the physical or speculum examination findings confirming cervical inflammation, any laboratory or swab results documenting the infectious agent, and the treatment plan. For audit purposes, a diagnosis of cervicitis stated without examination findings is insufficient to support medical necessity.
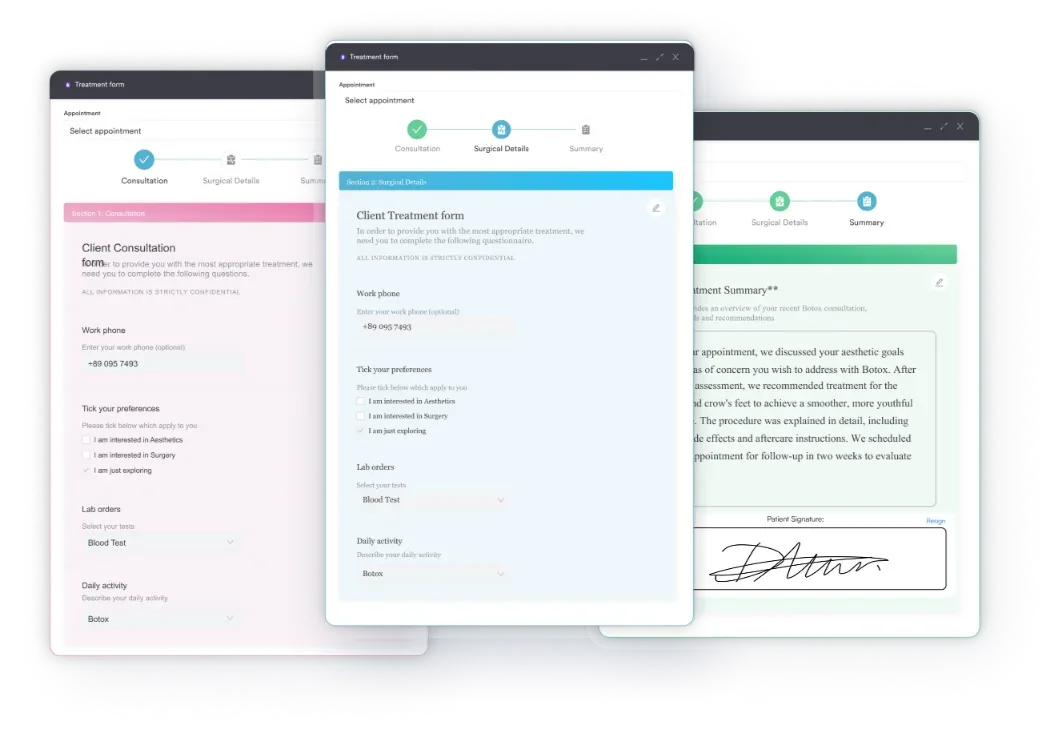
Practices using digital intake forms can capture structured symptom histories (vaginal discharge characteristics, pelvic pain, dyspareunia, contact bleeding) before the clinician encounter, reducing documentation time and ensuring completeness. Structured pre-visit data also makes it easier to demonstrate symptom onset and acuity in an audit response.
Both acute and chronic cervicitis map to N72. However, the clinical note should specify acuity because this affects treatment decision-making and any associated E/M complexity calculation. Acute on chronic cervicitis, one of the official synonyms for N72, should be documented when the patient has a history of chronic cervicitis with a new inflammatory episode superimposed.
Chronic cervicitis without an acute exacerbation may appear in a list of chronic conditions supporting a higher-complexity E/M code. In that scenario, confirm that N72 is sequenced appropriately relative to the primary reason for the encounter.
Pabau helps gynecology and women's health practices capture complete encounter documentation, pair diagnosis codes with infectious agent findings, and submit cleaner claims. See how it works.

N72 sits at a specific intersection in the ICD-10-CM hierarchy. Knowing the codes above and below it prevents misassignment and helps build more complete claim documentation for complex gynecological encounters.
The A54.03 row warrants specific attention. When gonococcal cervicitis is the confirmed diagnosis, A54.03 is the correct primary code: the ICD-10-CM Alphabetic Index entry for “cervicitis due to gonorrhea” directs coders to A54.03, not to N72 with B96.89.
Verify WHO ICD-10 sequencing guidance and your payer’s medical policy for STI diagnoses to confirm current requirements. Coders handling these charts should check the AAPC Codify ICD-10-CM lookup for current coding notes. The same specificity principle applies to other confirmed STIs, like A64, where the organism-specific code takes precedence over a symptom-based code.
When a patient presents with confirmed chlamydial cervicitis, check whether A56.09 (Other chlamydial infection of lower genitourinary tract) is more appropriate than N72 with B96.0. The ICD-10-CM Alphabetic Index entry for ‘cervicitis due to chlamydia’ directs coders to A56.09. Defaulting to N72 in this scenario is technically an error. Review the index, not just the tabular code, for organism-specific cervicitis.
Auditors reviewing N72 claims look for four recurrent patterns. Practices that address these in their charge capture workflow see measurably fewer post-payment recovery requests.
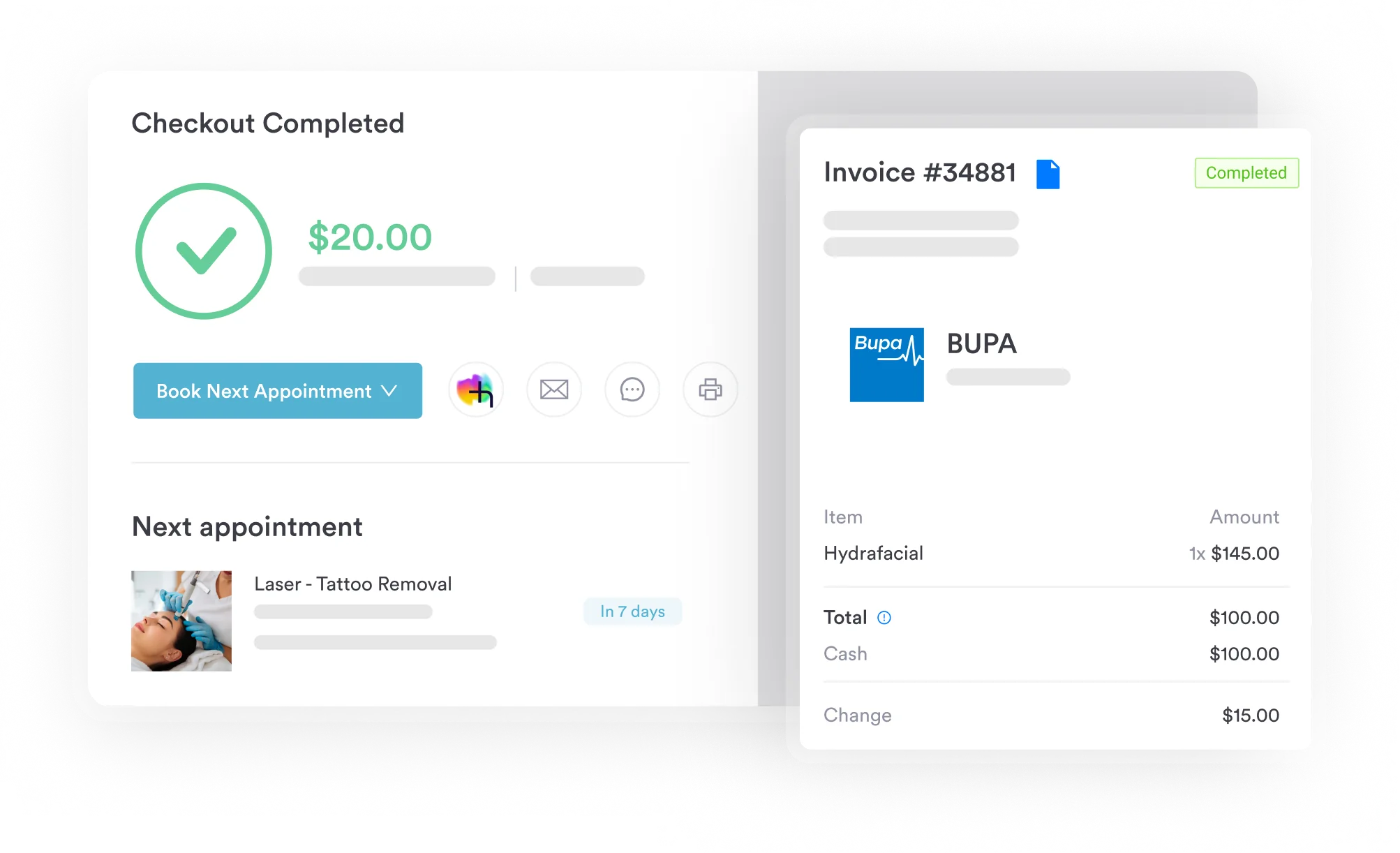
Using claims management software that surfaces coding edits at the point of charge capture can flag missing B95-B97 pairings before the claim is transmitted, reducing denial rates without adding manual review time.
For practices that handle large volumes of N72 claims, building a code-pair rule for N72 plus B95-B97 into the EHR’s clinical decision support layer is worth the configuration time. Well-structured HIPAA-compliant documentation practices also provide the audit trail needed if a payer requests medical records.
Accurate N72 coding starts at intake, not at charge capture. A structured documentation workflow that runs from the patient’s first symptom entry through the lab result review ensures the clinical note supports the code before the claim is built.
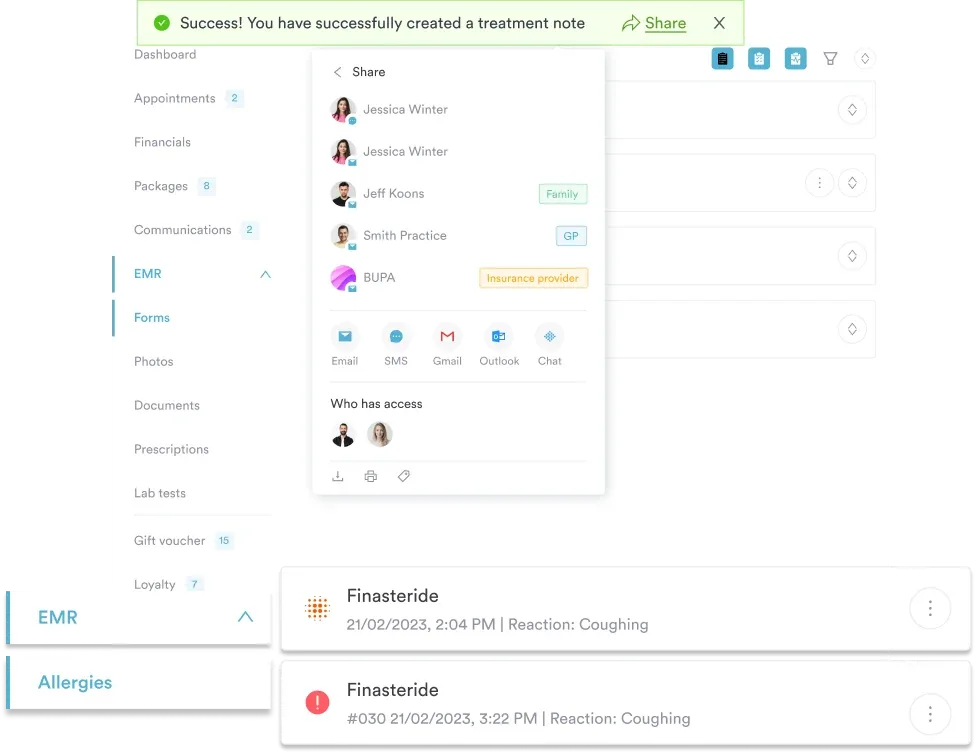
Practices building this workflow into their patient record management system benefit from a built-in link between the lab result entry and the diagnosis code field, keeping clinical documentation and coding in sync. Pabau’s AI-assisted clinical documentation can help clinicians structure encounter notes to include the examination findings and organism identification that support N72 claims.
N72 is confirmed as a valid, billable/specific ICD-10-CM diagnosis code for FY2026. It is not a header or non-billable parent code; it is the most specific available code for inflammatory disease of the cervix uteri within the current classification.
The ICD-10 diagnostic coding framework for N72 follows the same chapter-14 hierarchy used across all genitourinary diagnoses, making it navigable by any coder familiar with the N00-N99 block. Practices billing a pelvic exam alongside the N72 diagnosis can reference G0101 for the corresponding procedure code.
For practices new to the code range, CDC and NCHS provide free access to the current tabular list, index, and instructional notes. For related obstetric and gynecological code guidance, see O62.4.
Omitting the B95-B97 pairing when an organism is documented is the costliest N72 coding error. It creates an incomplete claim that invites denial, audit, and post-payment recovery. Every N72 encounter should end with a deliberate check: organism identified, code paired, Excludes1 conflict resolved.
Pabau’s compliance management tools and structured clinical documentation features help gynecology and women’s health practices build this check into the standard charge capture workflow, keeping clinical findings and billing accuracy aligned. To see how Pabau supports cleaner coding across your practice, book a demo.
Need to document a routine exam that turns up cervicitis findings? Pelvic exam documentation template gives your team a structured format for capturing speculum findings and discharge characteristics.
Coding a confirmed chlamydial infection outside the lower genitourinary tract? A55 covers lymphogranuloma venereum, a distinct STI diagnosis coders sometimes confuse with routine chlamydial cervicitis.
Billing a routine gynecological exam with no abnormal findings? Z01.419 is the code for a normal screening visit with no inflammation present, unlike N72.
ICD-10 Code N72 is used to document and bill for inflammatory disease of the cervix uteri, including cervicitis, endocervicitis, and exocervicitis with or without erosion or ectropion. It is a billable FY2026 code applicable to any encounter where cervical inflammation is the confirmed or working diagnosis.
Inflammatory disease of the cervix uteri is inflammation of the cervix, the lower portion of the uterus that opens into the vagina. It encompasses cervicitis, endocervicitis (affecting the inner canal), and exocervicitis (affecting the outer cervix), most commonly caused by sexually transmitted infections such as chlamydia, gonorrhea, or herpes simplex.
A B95-B97 code should be added after N72 only when the organism doesn’t have its own combination code — for example, B95.1 for Group B Streptococcus. Gonorrhea, herpes, and chlamydia have dedicated combination codes (A54.03, A60.03, and A56.09) that take priority over pairing N72 with B95-B97. If the organism is not identified, assign N72 alone without speculative coding.
Cervical erosion or ectropion without active cervicitis is excluded from N72 under its Excludes1 note; those presentations belong to N86. Additionally, confirmed organism-specific diagnoses (such as gonococcal cervicitis coded to A54.03, herpetic cervicitis coded to A60.03, or chlamydial infection coded to A56.09) may require the infectious disease chapter code instead of N72 as the primary diagnosis.
Yes. N72 is a valid, billable/specific ICD-10-CM diagnosis code for FY2026. It is not a non-billable header code; it is the most specific code available for inflammatory disease of the cervix uteri and can be submitted on claims for outpatient, inpatient, and professional fee encounters.
Cervicitis is a broad term for inflammation of the cervix. Endocervicitis specifically refers to inflammation of the endocervical canal and glandular cells, more commonly associated with ascending infections like chlamydia and gonorrhea. Exocervicitis involves the ectocervix and squamous cells. All three map to N72 in ICD-10-CM.