ICD-10 code S62.163P: Displaced pisiform fracture, malunion
ICD-10 code S62.163P is a billable diagnosis code for a displaced fracture of th...
Last Updated: August 7, 2026
ICD-10 Code M83.4 is a long-standing, billable diagnosis code for aluminum bone disease, also documented as dialysis osteomalacia, currently in force under the FY2026 edition (effective October 1, 2025 – September 30, 2026)
M83.4 applies exclusively to aluminum-related bone disease in dialysis patients; it does not cover other forms of adult osteomalacia coded under M83.0-M83.9
Excludes1 conditions include infantile and juvenile osteomalacia (E55.0), renal osteodystrophy (N25.0), sequelae of rickets (E64.3), and vitamin D-resistant osteomalacia/rickets (E83.31), meaning these cannot be coded with M83.4 under any circumstance
Practice management software like Pabau, together with clinical documentation tools, helps nephrology and dialysis practices submit M83.4 claims accurately with the correct supporting documentation
ICD-10 Code M83.4 is the billable diagnosis code for aluminum bone disease, also documented as dialysis osteomalacia. It applies to the metabolic bone disorder that develops in patients on long-term dialysis, sitting within the M83 adult osteomalacia block alongside eight sibling codes for other causes of adult bone softening.
Coders often default to a generic M83 sibling code when a chart doesn’t spell out the cause. M83.4 requires the physician to document aluminum accumulation specifically, along with the excludes notes that separate it from renal osteodystrophy and the other bone disorders seen in dialysis patients.
M83.4 has been part of ICD-10-CM since October 1, 2015 (FY2016) and hasn’t changed in any fiscal year since, including the current FY2026 edition, in force October 1, 2025 through September 30, 2026.
Coders can use it for claim submission and diagnosis documentation without selecting a more granular child code, since M83.4 is itself the specific, terminal code in this branch.
The code sits within Chapter 13 of ICD-10-CM (Diseases of the musculoskeletal system and connective tissue), under block M80-M85 (Disorders of bone density and structure), within category M83 (Adult osteomalacia).
Unlike many M83 subcodes, M83.4 carries no laterality or site specification. Aluminum bone disease affects systemic bone metabolism rather than a localized anatomical site.
Aluminum bone disease is a metabolic bone disorder caused by the accumulation of aluminum in bone tissue. It occurs almost exclusively in patients on long-term dialysis, particularly those exposed to aluminum-containing phosphate binders or aluminum-contaminated dialysate before modern low-aluminum protocols became standard.
Physicians practicing in metabolic health, nephrology, and primary care will encounter this condition most often in patients with a long dialysis history.
At the cellular level, aluminum displaces calcium at bone mineralization fronts, blocking normal osteoid calcification. The result is defective bone matrix that fractures under normal mechanical load. Clinically, patients present with bone pain, proximal muscle weakness, and pathological fractures, particularly in weight-bearing bones.
Serum aluminum levels, deferoxamine challenge testing, and bone biopsy with aluminum staining are the primary diagnostic tools used to confirm the condition before coding M83.4.
ICD-10-CM includes an “Applicable To” note under M83.4 that coders must recognize when mapping physician documentation to this code. If a physician writes “dialysis osteomalacia” in the chart, M83.4 is the correct code, not a more generic M83 subcode.
Coders should flag any chart documentation using “dialysis osteomalacia” and map it directly to M83.4 without querying the physician for further specificity, since the applicable-to note confirms this synonym explicitly. HIPAA mandates ICD-10-CM for all covered transactions, so payer-specific variances don’t affect M83.4’s submittability. The same holds for dialysis procedure codes like CPT 90935.
Understanding where ICD-10 Code M83.4 sits within the full M83 block prevents coders from selecting a less-specific sibling code when M83.4 is the correct choice. The table below shows the complete M83 subcategory set:
The most common coding error in this block is assigning M83.9 (unspecified) when the chart clearly documents dialysis as the context. Whenever aluminum accumulation or dialysis history supports M83.4, the unspecified code should never be used.
The same specificity principle applies elsewhere in ICD-10-CM. M65.4 is a comparable example: a precise code that’s frequently downgraded to an unspecified one when documentation doesn’t clearly support it.
Excludes notes at the M83 parent level apply to all M83 subcodes, including M83.4. Understanding the distinction between Excludes1 and Excludes2 is critical: an Excludes1 note means the excluded condition cannot be coded with M83.4 under any clinical circumstances.
M83.5 covers other drug-induced osteomalacia. Coders sometimes confuse M83.4 with M83.5 when aluminum-containing medications, rather than dialysate contamination, are implicated. The deciding factor is whether dialysis is the confirmed route of aluminum exposure.
If the patient is on dialysis and aluminum overload is documented, M83.4 is correct. If aluminum toxicity stems from long-term antacid use in a non-dialysis patient, M83.5 may apply instead, and coding guidance should be queried from the physician.
Dialysis patients often carry multiple bone and mineral metabolism diagnoses simultaneously. The codes below appear frequently alongside M83.4 as secondary codes, or as alternatives when aluminum-specific bone disease is not confirmed:
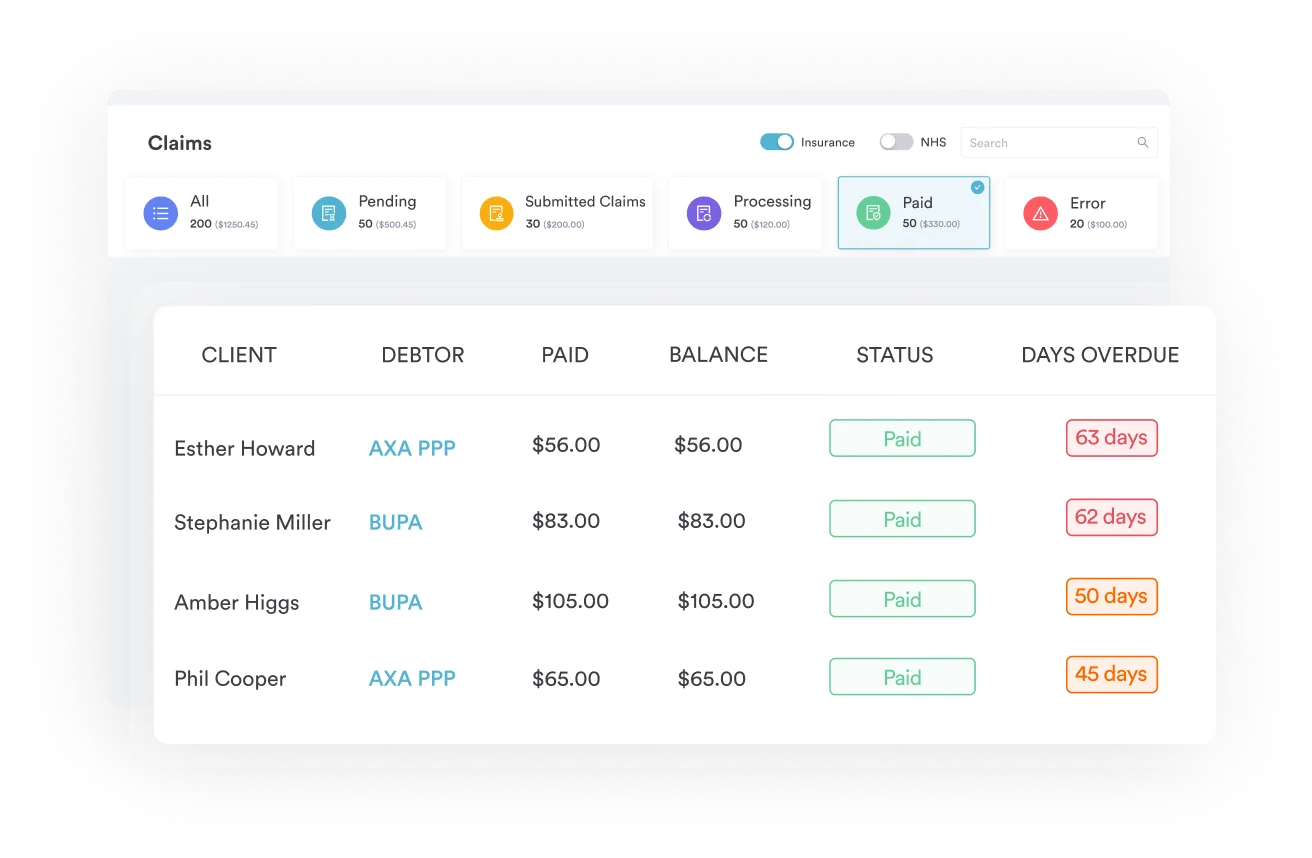
For dialysis practices coding complex multi-diagnosis claims, claims management software that supports multiple simultaneous diagnosis codes per encounter reduces the risk of dropping secondary codes from the claim.
Denied M83.4 claims almost always trace back to incomplete physician documentation. The chart must support each element of the diagnosis independently. Pre-structured clinical documentation forms can capture these data points consistently at every nephrology encounter.
Practices using structured clinical documentation tools can build nephrology-specific templates that prompt clinicians to capture each of these fields before the note is finalized. Missing even one element, particularly the aluminum exposure source, is enough for a payer to question the M83.4 coding.
Run a deferoxamine challenge test result as your primary clinical anchor for M83.4. A serum aluminum rise above 50 mcg/L post-DFO infusion, combined with a dialysis history and compatible bone symptoms, gives coders and auditors a clean, defensible record without relying solely on biopsy data.
The ICD-10-CM Official Guidelines for Coding and Reporting, maintained jointly by CMS and NCHS, govern sequencing and code selection for M83.4.
The WHO ICD-10 browser provides the international parent classification context, while the AAPC Codify ICD-10-CM lookup supports rapid code verification for US coders.
ICD-10-CM is the mandated code set for all covered-entity transactions under HIPAA compliance rules for medical offices.
Nephrology and dialysis practices managing complex metabolic bone cases need documentation workflows that capture the right clinical detail before the claim is submitted. Pabau’s claims management software supports multi-diagnosis claim submission, reducing the risk of dropping secondary codes like Z99.2 from an M83.4 encounter.
Pre-built nephrology consultation forms, created through digital intake forms, can prompt clinicians to document aluminum exposure history, deferoxamine test results, and dialysis duration at the point of care, rather than after a denial arrives.
Structured EHR integration workflow connects clinical documentation to billing, so coders work from complete records instead of chasing down missing data before the claim window closes. Practices that also need audit-ready records can rely on compliance management software to keep documentation standards consistent across every provider.
Pabau helps nephrology and specialist practices capture the clinical documentation needed to support complex diagnostic codes like M83.4 at the point of care. See how our claims management and digital forms tools reduce denial rates.

Miscoding aluminum bone disease costs dialysis practices claim denials that are entirely preventable. The chart note needs to confirm aluminum as the causative agent, establish the dialysis history, and include the laboratory markers that support the diagnosis before a coder assigns M83.4 with confidence.
Pabau’s digital forms and claims management tools help practices build this documentation into the clinical workflow rather than chasing it after a denial. To see how Pabau handles nephrology and metabolic bone disease coding documentation, compare specialist EHR options or book a demo with the team.
Billing hemodialysis sessions alongside M83.4? CPT 90945 covers dialysis procedures other than hemodialysis, with the same specificity requirements that apply to aluminum bone disease claims.
Confirming an osteomalacia diagnosis with imaging? CPT 77080 is the DXA bone density scan code used to support a bone-disease diagnosis alongside M83.4.
Coding weight loss in chronic dialysis patients? ICD-10 Code R64 covers cachexia, a frequent comorbidity that needs the same explicit physician documentation as M83.4.
Want another example of specificity preventing a denial? ICD-10 Code K12.2 walks through a commonly downgraded oral diagnosis code.
ICD-10 Code M83.4 is the billable diagnosis code for aluminum bone disease, a metabolic bone disorder caused by aluminum accumulation in bone tissue that occurs primarily in patients on long-term dialysis. It is used for claim submission, diagnosis documentation, and insurance reimbursement when the physician has confirmed that aluminum overload is the cause of the patient’s bone disease.
Yes. M83.4 is a long-standing, billable/specific ICD-10-CM code, valid for claim submission and currently in force under the FY2026 edition (effective October 1, 2025 \u2013 September 30, 2026). It requires no further subdivision and can be used directly on insurance claims without selecting a more granular child code.
Dialysis osteomalacia is the clinical term for bone softening caused by aluminum accumulation in dialysis patients. It is listed as an Applicable To synonym under M83.4, meaning that whenever a physician documents “dialysis osteomalacia” in the patient record, M83.4 is the correct ICD-10 code to assign without further query.
The M83 parent code carries Excludes1 notes for infantile and juvenile osteomalacia (E55.0), renal osteodystrophy (N25.0), sequelae of rickets (E64.3), and vitamin D-resistant osteomalacia/rickets (E83.31). These conditions cannot be coded simultaneously with M83.4. Vitamin D deficiency (E55.9) may be coded separately as a comorbidity if independently documented, since it is not subject to an Excludes1 restriction against M83.4.
M83.4 is a long-standing, billable ICD-10-CM code that has been in place since October 1, 2015 (FY2016) and has not been revised in any fiscal year since. October 1, 2025 simply marks the start of the current FY2026 annual cycle, under which M83.4 remains unchanged and fully billable through September 30, 2026.
The most relevant codes are M83.4 (aluminum bone disease/dialysis osteomalacia), N25.0 (renal osteodystrophy, for broader CKD-MBD when aluminum etiology is not confirmed), E21.3 (hyperparathyroidism as a common comorbidity), and Z99.2 (dependence on renal dialysis, coded alongside M83.4 to establish clinical context for payers).