ICD-10 Code K25.0: Gastric ulcer, acute with hemorrhage
ICD-10 Code K25.0 is a billable, specific ICD-10-CM code describing a gastric ul...
July 23, 2026
ICD-10 Code D73.5 is a billable, specific diagnosis code for infarction of spleen, valid for FY2026 under the D50-D89 chapter.
Inclusion terms cover splenic rupture (nontraumatic) and torsion of spleen, but NOT traumatic splenic injuries, which use the S36.0x series.
Always sequence the underlying etiology (atrial fibrillation, sickle cell disease, hypercoagulable state) as the principal diagnosis when it drives the encounter.
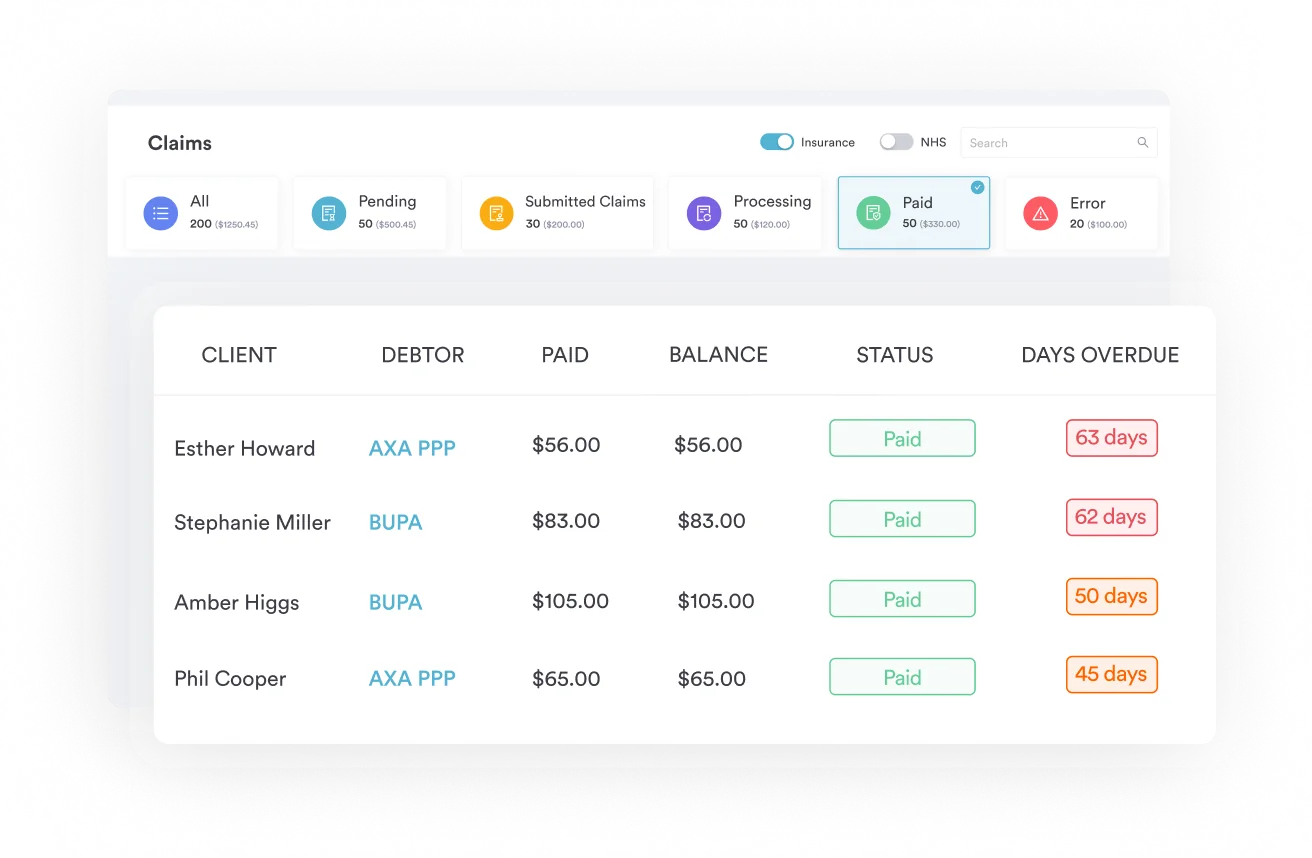
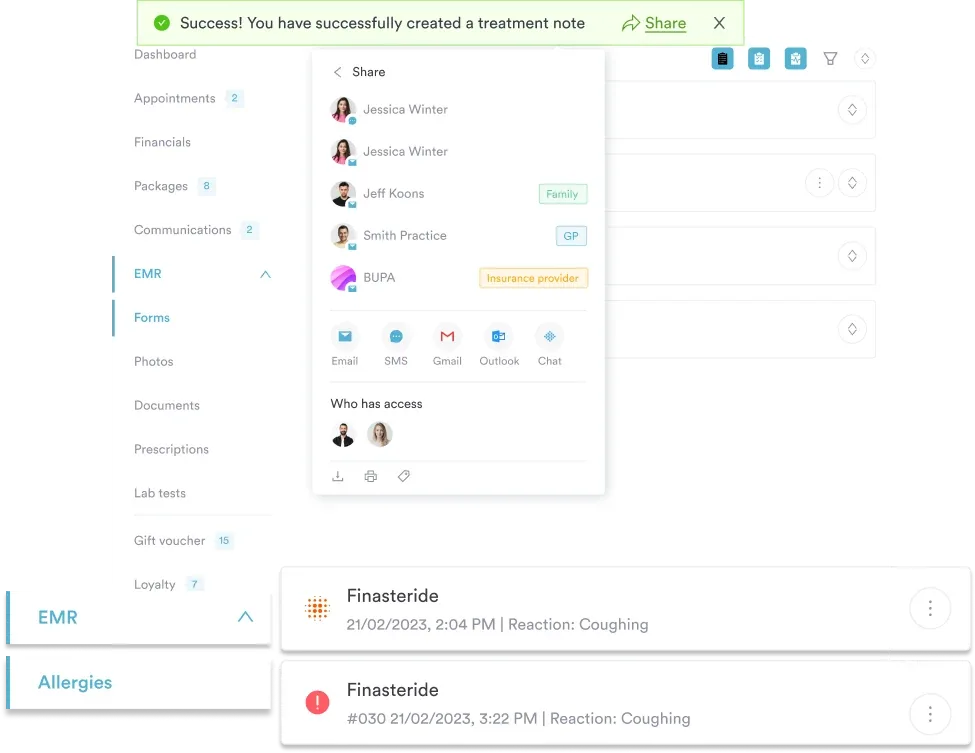
Pabau’s claims management software and AI-assisted documentation help practices capture D73.5 accurately and reduce claim errors at submission.
ICD-10 Code D73.5 is the billable, specific ICD-10-CM code for infarction of spleen, covering nontraumatic splenic rupture and torsion of spleen as inclusion terms. It is valid for FY2026 and is usually sequenced as a secondary code, following the underlying etiology that drove the encounter. Pabau’s claims management software keeps ICD-10 codes tied directly to patient records, reducing errors at submission.
D73.5 sits within Chapter 3 (Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism, D50-D89), under the block D70-D77 (Other disorders of blood and blood-forming organs), and within the parent category D73 (Diseases of spleen). The code has been valid and billable every fiscal year from 2016 through FY2026, as confirmed by the CDC/NCHS ICD-10-CM web tool.
Splenic infarction, also called splenic infarct, occurs when blood supply to the spleen is interrupted, causing tissue death in the affected region. Clinically, it presents as acute left upper quadrant pain, sometimes radiating to the left shoulder, and is associated with fever, nausea, and elevated inflammatory markers.
The condition is typically discovered on CT imaging and most commonly arises as a complication of hematologic disease, thromboembolic events, or structural cardiac conditions.
Two additional conditions are captured under D73.5 as inclusion terms in the official tabular list. Both are nontraumatic splenic conditions and must not be confused with injury codes.
Coders and clinicians should verify these inclusion terms against the official tabular list maintained by the Centers for Medicare and Medicaid Services (CMS). The inclusion terms do not expand the code’s scope; they clarify equivalent conditions that map to the same code. Accurate clinical documentation distinguishing among these presentations is essential before the code is assigned.
Traumatic splenic injuries are explicitly outside the scope of D73.5. Blunt abdominal trauma causing splenic laceration, rupture, or contusion is coded using the S36.0x series under Chapter 19 (Injury, poisoning, and certain other consequences of external causes). Applying D73.5 to a traumatic rupture is a coding error that may trigger a claim audit.
Similarly, other diseases of the spleen listed under D73 have their own specific codes and should not default to D73.5. For instance, splenic abscess maps to D73.3, and cyst of spleen maps to D73.4.
Understanding where D73.5 sits within the ICD-10-CM hierarchy helps coders navigate the full D73 category and select the most specific code available. The WHO ICD-10 browser provides the authoritative classification structure.
Coders handling other hematologic disorders can reference our guide to ICD-10 Code D69.3 (immune thrombocytopenic purpura) for parallel sequencing logic. When D73.9 (unspecified) is tempting because documentation is incomplete, the better path is to query the provider before assigning a non-specific code.
D73.5 marks one point in a splenic condition’s coding lifecycle, so the right code depends on the spleen’s current status. An active infarction is D73.5. Once the tissue loss leaves the spleen underfunctioning, it becomes D73.0 (hyposplenism, which covers functional asplenia). A surgically removed spleen becomes Z90.81 (acquired absence of spleen), and a fully resolved event with no current treatment moves to a personal history code, Z86.2.
Practices transitioning legacy data, supporting audits on historical claims, or working with older EHR records will encounter ICD-9-CM codes. The crosswalk for splenic infarction maps as follows:
The ICD-10-CM system introduced substantially more granularity for splenic conditions. D73.5 replaced a broader ICD-9 bucket code that grouped multiple splenic conditions together. For consistent mapping, coders should verify legacy crosswalks against the official General Equivalence Mappings (GEMs) rather than relying on memory.
When querying historical claims data or running an audit against pre-2015 records, always document both the ICD-9 legacy code and the ICD-10-CM equivalent in your reconciliation notes. A one-to-one crosswalk rarely exists for splenic conditions, and payers may require explicit mapping documentation during audits.
Insufficient documentation is the primary reason D73.5 claims face payer scrutiny. Coders cannot assign a code that the clinical record does not support, and “splenic infarction” must appear as a confirmed diagnosis, not a rule-out or differential.
The clinical record must include all of the following to support D73.5:
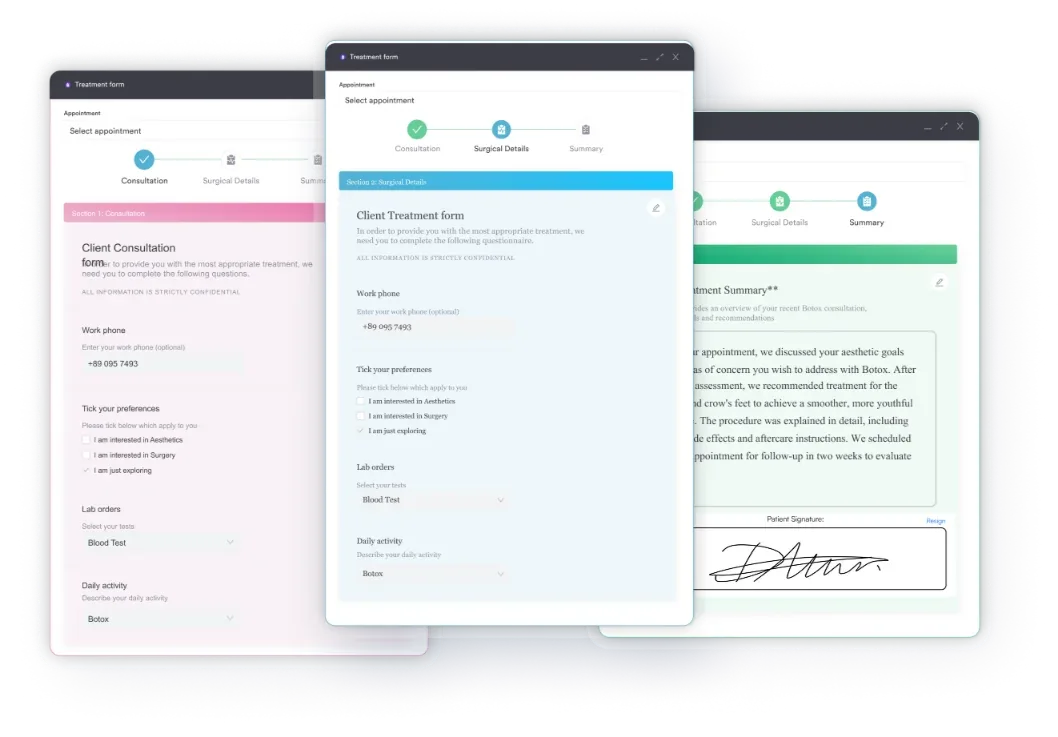
Practices using digital intake forms to capture presenting symptoms systematically reduce the risk of incomplete documentation at the point of first contact. When the ICD-10 coding workflow is embedded in the EHR, coders work from structured notes rather than hunting through unorganized free text.
Dedicated clinical documentation software makes that structure routine, which matters when a payer requests medical records to support a D73.5 claim.
D73.5 is almost always a secondary code. The principal diagnosis should reflect the underlying condition driving the encounter. ICD-10-CM Official Guidelines from the National Center for Health Statistics (NCHS) direct coders to sequence the etiology first when it is known and documented.
Common principal diagnoses coded alongside D73.5 include:
When the etiology is not yet identified and the encounter is specifically for splenic infarction, D73.5 may serve as the principal diagnosis. However, the documentation must clearly state that no underlying cause was identified at the time of the encounter. Understanding accurate ICD-10-CM sequencing principles for primary versus secondary positioning helps avoid errors across all diagnostic categories, not just splenic conditions.
Pabau links diagnosis codes directly to patient records and clinical notes, so your billing team works from structured, verified data rather than decoding handwritten charts. See how it works for your practice.

Three errors account for the majority of D73.5 claim problems. Each is preventable with tighter documentation workflows and coder education.
Traumatic splenic rupture following motor vehicle accidents, falls, or sports injuries does not belong under D73.5. The correct codes are in the S36.0x series (injury to spleen). Applying D73.5 to a trauma encounter will typically be flagged by claims editing software because the principal diagnosis codes (trauma, injury) do not logically associate with a non-traumatic splenic code.
Payer systems look for clinical coherence across the claim. Practices concerned about HIPAA-compliant documentation workflows should ensure their coding audit trails clearly distinguish traumatic from non-traumatic presentations.
A CT report that reads “findings consistent with splenic infarction” is not a physician-confirmed diagnosis. ICD-10-CM guidelines require the attending or treating physician to document the diagnosis. If only the radiologist’s report exists, the coder should query the physician before assigning D73.5. Failure to do this creates exposure during retrospective audits.
Coding D73.5 alone on a claim where the underlying cause is documented and known is an incomplete code set. Payers expect to see the etiological chain. Missing the principal diagnosis can trigger a request for additional documentation or outright denial. The sequencing rules are clear: etiology first, manifestation (splenic infarction) second.
Build a D73.5 coding checklist into your EHR workflow: confirm confirmed diagnosis (not rule-out), verify no traumatic mechanism, identify and code the underlying etiology, and check that imaging documentation is signed by the treating physician. Reviewing this at claim creation prevents the most common denial triggers.
Accurate code capture starts at the clinical encounter, not the billing queue. When clinicians document in structured fields rather than free text, coders spend less time interpreting ambiguous notes and more time on quality review. Practices using practice management software features that integrate diagnosis code selection directly with the clinical note see fewer incomplete records at claim creation.
Specific workflow improvements that support D73.5 accuracy:
For practices managing multiple specialty workflows, functional medicine practices dealing with autoimmune or hematologic presentations encounter D73.5 in the context of broader multisystem workups. Having a consistent coding protocol for secondary diagnosis codes across these complex encounters reduces variability in claim accuracy.
Splenic infarction presents a specific coding challenge: a condition that almost always has an underlying cause, that must be distinguished from traumatic injury, and that requires explicit physician documentation before the code can be assigned. ICD-10 Code D73.5 covers infarction of spleen, nontraumatic splenic rupture, and torsion of spleen. It is a secondary code in most encounters, following the principal diagnosis of the underlying etiology.
Pabau supports accurate ICD-10 Code D73.5 capture through structured clinical records, integrated diagnosis code workflows, and AI-assisted documentation that ensures key details are never lost between the clinical encounter and claim submission. To see how practice management software works to streamline diagnostic coding workflows, book a demo.
Need a structured approach to clinical documentation for complex diagnoses? Safer clinical notes provides a step-by-step framework for producing defensible, audit-ready records across specialty encounters.
Coding other blood and spleen disorders? ICD-10 Code D50.0 (iron deficiency anemia) walks through documentation and sequencing for a related hematologic diagnosis.
Looking to reduce billing errors across your practice? Claims management software from Pabau links diagnosis codes directly to patient records, supporting accurate submission from the first draft.
ICD-10 Code D73.5 is used to document infarction of spleen, a condition in which blood supply to the spleen is blocked, causing tissue death. It also covers nontraumatic splenic rupture and torsion of spleen as inclusion terms. The code applies to non-traumatic presentations only; traumatic splenic injuries use the S36.0x injury codes.
Yes, D73.5 is a billable and specific ICD-10-CM diagnosis code valid for FY2026. It can be submitted on a claim as a principal or secondary diagnosis, depending on the clinical context and whether an underlying etiology is identified and documented.
The inclusion terms for D73.5 are splenic rupture (nontraumatic) and torsion of spleen. These are not separate codes; they map to D73.5 as equivalent conditions listed in the official ICD-10-CM tabular list.
The closest ICD-9-CM equivalent for splenic infarction under D73.5 is 289.59 (Other diseases of spleen), which was a broader, less specific code that grouped multiple splenic conditions together before the ICD-10-CM transition increased granularity.
The D73 category includes hyposplenism (D73.0), hypersplenism (D73.1), chronic congestive splenomegaly (D73.2), abscess of spleen (D73.3), cyst of spleen (D73.4), infarction of spleen (D73.5), neutropenic splenomegaly (D73.81), other diseases of spleen (D73.89), and disease of spleen unspecified (D73.9). Each has its own billable code.
Once a splenic infarction has resolved and no longer needs active treatment, it is no longer reported with D73.5. A documented history of splenic infarct is captured with a personal history code, Z86.2 (personal history of diseases of the blood and blood-forming organs). D73.5 stays on the claim only while the infarction is an active, physician-confirmed diagnosis.
Functional asplenia, where the spleen is present but no longer works, is coded D73.0 (hyposplenism), which also covers atrophy of the spleen. This differs from D73.5, since a splenic infarction can eventually cause hyposplenism once enough tissue is lost. Confirm the spleen’s current status against the tabular list before assigning either code.
After the spleen has been surgically removed, use Z90.81 (acquired absence of spleen) rather than a disease code. This status code signals that the organ is gone, which affects vaccination, infection risk, and later encounters, so it belongs on the problem list once a splenectomy has been performed.