Obesity nursing care plan: Current NANDA-I diagnoses
Download your free obesity nursing care plan template A ready-to-use plan coveri...
Last Updated: August 6, 2026
High cholesterol (LDL ≥ 130 mg/dL) raises cardiovascular disease risk and requires a structured dietary management strategy.
Foods rich in soluble fiber, omega-3 fatty acids, and plant sterols naturally reduce LDL — saturated and trans fats raise it. This evidence-based diet plan guides patient food selection.
The DASH and Mediterranean diets are the two most evidence-backed dietary protocols for lowering LDL while improving HDL and triglycerides.
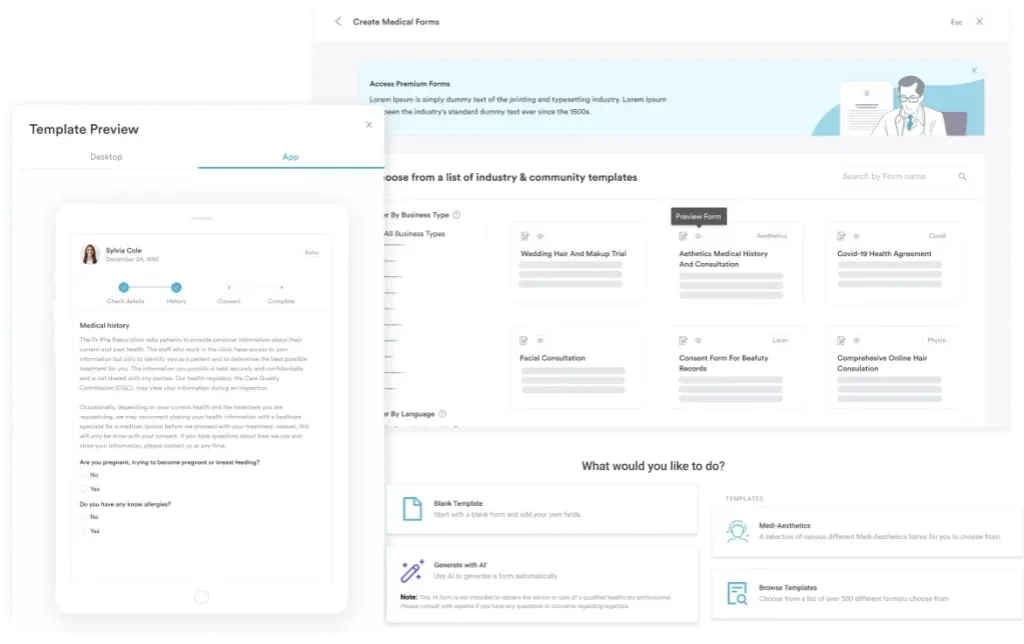
Practice management software like Pabau offers digital forms and an AI scribe that help clinicians distribute this diet plan and track patient adherence during follow-up visits.
A comprehensive nutritional guidance template covering recommended and avoided foods, a 7-day meal plan, and evidence-based dietary protocols (DASH, Mediterranean) for managing LDL, HDL, and triglycerides.
Download templateElevated cholesterol (LDL ≥ 130 mg/dL) is a silent risk factor for cardiovascular disease. Yet many patients struggle to translate “eat healthier” into actionable daily choices.
This clinician-ready digital forms template provides a structured high cholesterol diet plan you can hand to patients at the point of care — complete with a 7-day meal plan, foods to prioritize, items to avoid, and guidance on evidence-based dietary protocols (DASH and Mediterranean) that lower LDL naturally.
A high cholesterol diet plan is a structured nutritional intervention designed to lower LDL (low-density lipoprotein — the “bad” cholesterol) while maintaining or raising HDL (high-density lipoprotein — the “good” cholesterol) and reducing triglycerides.
Unlike a medication-first approach, dietary intervention targets the root cause: excessive saturated fat, trans fat, and refined carbohydrates that drive cholesterol synthesis in the liver.
That root-cause focus is why dietary intervention fits naturally into functional medicine practices, where lifestyle-first care is often the starting point before medication.
The clinical evidence is strong. The American Heart Association recommends limiting saturated fat to no more than 5-6% of total daily calories for patients with elevated LDL, alongside increasing soluble fiber intake.
For many patients with borderline or mild elevation, dietary changes alone may defer or eliminate the need for statin therapy — making this template an essential first-line counseling tool.
Evidence-based cholesterol-lowering foods fall into three categories: soluble fiber sources, omega-3 fatty acids, and plant-derived compounds that block cholesterol absorption.
Patients benefit from a downloadable visual checklist they can carry to the grocery store. Pabau’s AI scribe tool can help document which food categories each patient commits to prioritizing during their next appointment.
Limiting these items is essential for LDL reduction:
This practical 7-day framework balances fiber, omega-3, and plant sterol intake while keeping saturated fat under 5-6% of calories. Print and hand to patients at the end of the appointment.
Patients following a vegan or vegetarian pattern can adapt the same principles with a vegan diabetes meal plan as a starting template, swapping in plant-based proteins for the fish and dairy items below.
Three evidence-based protocols dominate the literature. All reduce LDL, but differ in emphasis, adherence, and secondary benefits.
DASH is the most evidence-backed for combined hypertension and cholesterol reduction. Mediterranean wins for long-term adherence and cardiovascular event prevention. Patient compliance tracking is critical — whichever protocol the patient chooses, follow-up visits should confirm adherence and adjust as needed.
Many patients present with elevated cholesterol alongside hypertriglyceridemia (triglycerides ≥150 mg/dL) or hypertension. Dietary adjustments accommodate all three targets:
Diabetes frequently coexists with high cholesterol as well. For these patients, a cardiac-diabetic diet food list layers glucose control on top of the same fiber- and fat-focused principles.
Patient care documentation should note baseline cholesterol, triglycerides, and blood pressure, then re-check at 6-8 weeks to assess dietary intervention efficacy before escalating to pharmacotherapy.
The downloadable template supports a structured patient education workflow:
Lifestyle vs. pharmacologic interventions frameworks guide when to escalate to statin therapy if diet alone is insufficient after 8-12 weeks. Track ongoing statin and supplement use alongside the diet plan with a daily medication chart.
Successful dietary intervention requires patient buy-in and accountability. Patient portals enable you to send follow-up check-ins, share educational resources, and request self-reported adherence data between appointments.
Store the completed diet plan template in the patient record alongside baseline lipid panel results and follow-up cholesterol values. This creates a clear narrative of dietary intervention outcomes.
Clinical documentation for dietary intervention should include:
HIPAA-compliant software keeps this record secure and audit-ready.
Store diet plans, lipid results, and follow-up notes in one integrated patient record. Use digital forms to distribute templates and AI scribe to document dietary discussions.

A structured high cholesterol diet plan is a powerful first-line intervention. This template gives you the evidence-based framework — foods to prioritize (soluble fiber, omega-3, plant sterols), foods to limit (saturated and trans fats), and three proven protocols (DASH, Mediterranean, low-fat).
Distribute the 7-day plan, set a follow-up lipid panel at 6-8 weeks, and track adherence in the patient record. For many patients, diet alone lowers LDL by 5-15% and defers or reduces medication — improving quality of life and long-term cardiovascular outcomes.
Practice management software like Pabau ties it together: digital forms distribute the template, an AI scribe documents dietary discussions, and patient portals keep follow-up on track between visits. Book a demo to see how Pabau closes the loop between your clinical decisions and patient accountability..
Looking to track long-term patient outcomes? Benefits of patient portals shows how consistent portal engagement supports better long-term dietary adherence.
Most patients see measurable LDL reductions (5-15%) within 6-8 weeks of consistent dietary adherence. Individual variation depends on baseline LDL, genetics, and diet compliance. Recheck labs at 8 weeks; if insufficient, consider statin therapy alongside continued dietary intervention.
Yes. One large egg contains 186 mg of dietary cholesterol but also provides high-quality protein and choline. The saturated fat content is modest (1.6g). Current AHA guidance allows up to one egg daily for most patients with high cholesterol; egg-white omelets are unlimited. Prioritize preparation method (poached or boiled over fried).
LDL (low-density lipoprotein) carries cholesterol from the liver to arteries, where it deposits and hardens into plaque-raising cardiovascular risk. HDL (high-density lipoprotein) removes excess cholesterol from arteries and returns it to the liver for excretion, protecting against heart disease. High cholesterol diet plans aim to lower LDL while maintaining or raising HDL.
Yes. The DASH diet (Dietary Approaches to Stop Hypertension), developed by NHLBI, reduces LDL by 5-11% and simultaneously lowers blood pressure. It emphasizes whole grains, legumes, vegetables, and low-fat dairy while limiting saturated fat and sodium. It is particularly effective for patients with concurrent hypertension.
Diet can defer or reduce statin therapy in patients with mild-to-moderate LDL elevation (130-189 mg/dL) without established cardiovascular disease. However, patients with severe elevation (≥190 mg/dL), prior cardiovascular events, or genetic hyperlipidemia typically require pharmacotherapy alongside diet. Always reassess after 8-12 weeks of dietary intervention before making medication decisions.