Elimination Diet Plan Guide
Download your free elimination diet plan template A ready-to-use elimination die...
Last Updated: July 17, 2026
An acupuncture SOAP note is a structured four-section documentation format: Subjective (patient symptoms), Objective (clinical findings including pulse and tongue), Assessment (TCM diagnosis), and Plan (specific acupoints and treatment details).
The Objective section must include pulse quality, tongue observation, palpation findings, and range of motion — these clinical markers directly inform acupoint selection.
Insurance reimbursement for acupuncture (CPT codes 97810, 97811, 97813, and 97814) requires thorough SOAP documentation that demonstrates medical necessity and tracks patient progress.
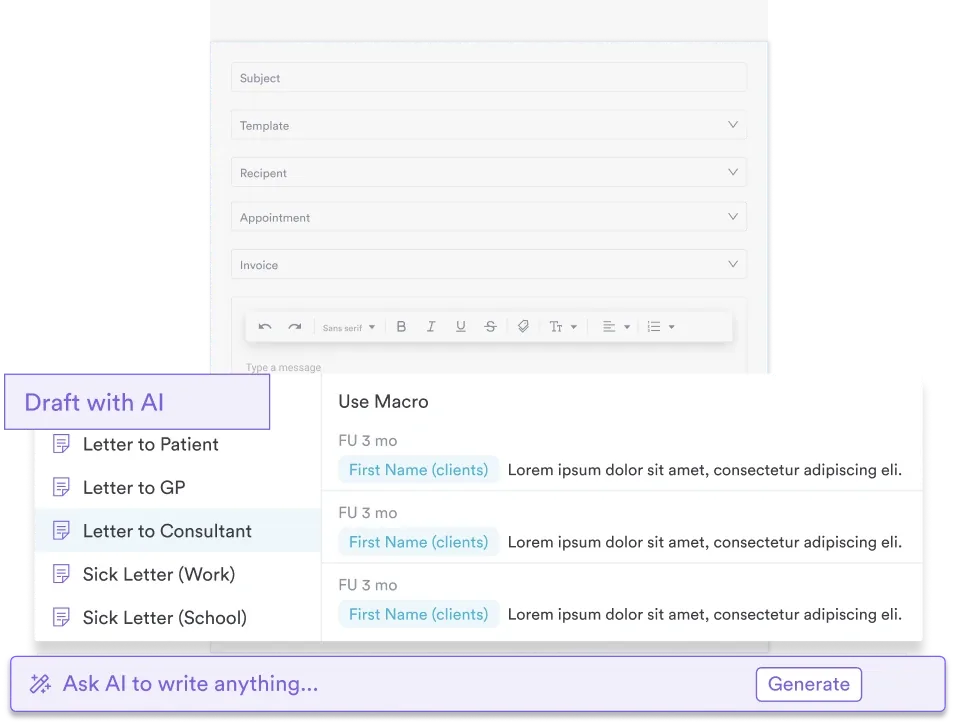
Pabau’s digital forms and client records features enable acupuncturists to create standardized SOAP templates and auto-populate fields, reducing documentation time and ensuring compliance.
A ready-to-use PDF template covering patient details, subjective symptoms, objective clinical findings (pulse, tongue diagnosis, palpation), assessment with TCM patterns, treatment plan with specific acupoints, and accessory modalities like cupping and e-stim.
Download templateAn acupuncture SOAP note is a structured clinical documentation system that helps practitioners record patient visits systematically. Whether you’re running a busy acupuncture practice or integrating acupuncture into a multidisciplinary practice, proper SOAP documentation ensures compliance, supports insurance billing, and creates a clear clinical record of treatment outcomes.
An acupuncture SOAP note is a four-section format for documenting patient encounters: Subjective (patient-reported symptoms and chief complaint), Objective (physical examination findings including pulse diagnosis, tongue observation, and palpation), Assessment (clinical diagnosis in both Western and Traditional Chinese Medicine terms), and Plan (treatment protocol with specific acupoints, needling technique, and accessory modalities).
A standardized structure does several jobs at once:
For acupuncturists treating chronic pain, anxiety, or musculoskeletal dysfunction, SOAP notes form the foundation of evidence-based, compliant practice. For a section-by-section breakdown, see these SOAP note examples, and how AI clinical documentation tools can auto-populate each field.
Using an acupuncture SOAP note template involves completing each section in a logical workflow during or immediately after the patient visit. Pair each plan with an acupuncture aftercare guide so patients know what to expect between sessions.
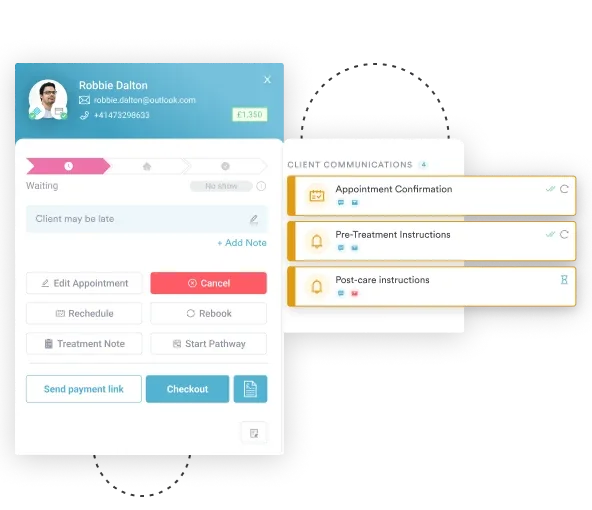
Practice management software like Pabau lets you standardize this workflow, auto-populate repeat information, and keep a historical record that shows patient progress. That history matters for both clinical care and billing justification.
Acupuncture SOAP notes are essential for licensed acupuncturists, acupuncture physicians (in regulated US states), and healthcare practitioners who integrate acupuncture into multidisciplinary practices: naturopathic doctors, chiropractors, integrative medicine physicians, physical therapists, and nurses with acupuncture credentials.
Related documentation templates include the chiropractic SOAP note template, the speech therapy SOAP note template, and the mental health SOAP note template.
SOAP notes are equally valuable in solo private practices and larger multi-location groups. They are required if you bill insurance under CPT codes 97810, 97811, 97813, and 97814 (acupuncture codes), as payers require documented clinical justification for payment.
In the UK, practitioners registered with the British Acupuncture Council (BAcC) or CNHC use SOAP notes to meet professional standards and patient safety requirements.
Clinical clarity: The four-section structure forces you to organize clinical thinking, ensuring no key findings are overlooked. This reduces diagnostic error and improves treatment outcomes.
Insurance billing compliance: Payers reviewing claims for CPT codes 97810, 97811, 97813, and 97814 expect SOAP notes demonstrating medical necessity, diagnosis, and measurable treatment response. Complete notes reduce claim denials and speed reimbursement.
Audit readiness: Regulatory bodies (CQC in England, CNHC in the UK, state licensing boards in the US) inspect clinical records during compliance audits. Properly formatted SOAP notes demonstrate professional standards and patient-centered care.
Patient continuity: If you work with staff or refer patients to colleagues, SOAP notes create a handoff document that another practitioner can understand immediately, ensuring care continuity and team safety.
Time savings: Using a standardized template, or an AI scribe such as Pabau Scribe, our AI scribe, cuts the time spent writing notes after each session, so you can focus on patients. See how AI SOAP notes cut documentation time further.
Traditional Chinese Medicine diagnostics — pulse reading and tongue assessment — are core to acupuncture practice, but they need clear documentation to stay useful for future visits and billing review.
Pulse documentation: Record the location (radial artery at three depths: superficial, middle, deep), quality (wiry, slippery, thready, tight, slow, rapid), and rate. Example: “Radial pulse at left middle position: wiry, rapid (95 bpm).” This specificity allows you to compare pulse changes across visits and track treatment response.
Tongue documentation: Note the color (pale, red, crimson), coating (white, yellow, thin, thick), moisture (dry, normal, wet), and any unusual markings (cracks, teeth marks). Example: “Pale tongue, white coating, slightly moist, with teeth marks along edges — consistent with Spleen Qi Deficiency.” Link findings to diagnosis.
Acupoint specificity: Never document treatment as “needled back area.” Instead, name the exact acupoints using standard abbreviations: LI4 (Large Intestine 4), LV3 (Liver 3), BL23 (Bladder 23), ST36 (Stomach 36), DU4 (Governing Vessel 4). Include ashi points (patient-identified tender sites) and note depth of insertion, needle retention time (e.g. “15 minutes”), and any manual stimulation (rotation, lifting-thrusting, or no manipulation).
Modality notation: If you used accessory techniques, document them clearly: “Cupping applied to BL13, BL17, BL20 for 5 minutes” or “E-stim (electroacupuncture) applied to LI4 bilaterally, 10 Hz, 10 minutes.” This creates a treatment map that shows your clinical reasoning and supports insurance billing.
Here’s how a completed follow-up note might read for a patient treated for chronic neck pain and work-related stress.
In practice management software like Pabau, the previous visit’s note pre-fills the baseline, so you only chart what changed: the pulse rate, the pain score, and the points you adjusted.
Insurance reimbursement for acupuncture requires specific documentation elements. CPT codes 97810, 97811, 97813, and 97814 cover acupuncture with and without electric stimulation, and payers require your SOAP notes to justify medical necessity and demonstrate measurable patient benefit.
Medicare sets an even narrower bar. It covers acupuncture only for chronic low back pain, defined as pain lasting 12 weeks or more with no specific cause, and pays for up to 12 visits in 90 days. Eight more visits are allowed only if your notes show the patient is improving, so progress tracking is what keeps the later visits payable.
Using automated workflows to flag when to re-evaluate patient progress or when a treatment course is complete reduces manual oversight and supports billing accuracy.
Pabau's digital forms and client records let you create standardized SOAP templates, auto-populate patient data, and maintain insurance-ready clinical records, all in one secure system.

The format changes slightly depending on the note type, so practitioners often maintain separate templates to ensure completeness. A concise format such as the ADIME note template suits nutrition-focused visits.
In an integrative medicine practice, having distinct re-evaluation workflows ensures accountability and regulatory compliance.
Write legibly or digitally: Handwritten notes risk illegibility, especially during insurance audits. Using digital forms and client portals ensures all notes are searchable and compliant with HIPAA and GDPR standards. Dedicated clinical documentation software keeps every note audit-ready.
Avoid vague terminology: Never write “treated generically” or “addressed imbalance.” Instead: “Treated LI4 and LV3 with manual rotation x 1 minute for Qi Stagnation” or “Applied moxibustion to DU4 and BL23 for 10 minutes to warm Kidney Yang.”
Be objective, not subjective: Separate your clinical observations (objective) from the patient’s experience (subjective). Objective = what you measure (pulse, tongue, ROM). Subjective = what the patient reports (pain level, emotional state).
Use consistent abbreviations: Pick a standard for acupoint naming (LI4 vs LI-4 vs Large Intestine 4) and stick with it. Consistency aids your own record-keeping and helps staff or colleagues understand your notes.
Document treatment duration and response: Always record time spent (e.g. “30-minute acupuncture session”) and any immediate feedback (“patient reported relief after needle placement; some tenderness at BL17 resolved”). This gives payers confidence in clinical efficacy.
Acupuncture regulation varies by jurisdiction, and your SOAP note format should align with local requirements.
United Kingdom: The British Acupuncture Council (BAcC) and Complementary and Natural Healthcare Council (CNHC) require registered practitioners to maintain patient records that demonstrate informed consent, clinical assessment, and safe practice.
SOAP notes meet these standards. The BAcC Code of Ethics and Safe Practice requires records to be legible and dated. In line with NHS retention guidance, keep adult records for at least eight years after treatment ends, and records for minors until the patient turns 25.
United States: In states where acupuncture is licensed (most US states plus DC), state boards require SOAP notes or equivalent records. For Medicare claims under CPT codes 97810, 97811, 97813, and 97814, documentation must demonstrate medical necessity, including treatment time and measurable progress. Check your state’s acupuncture regulatory board website for specific record-keeping requirements.
HIPAA and GDPR compliance: Whether you store notes on paper or digitally, they are protected health information (PHI) under HIPAA (US) or personal health data under GDPR (EU/UK). Use HIPAA-compliant practice management software to ensure notes are encrypted, access-controlled, and backed up securely.
Use the template provided, tailor it to your patient population, and keep your documentation habits consistent across visits.
A consistent acupuncture SOAP note documents your diagnostic reasoning, justifies your treatment decisions, and creates a record that supports patient safety, regulatory compliance, and insurance reimbursement. Whether you’re a solo practitioner or part of a multidisciplinary practice, that consistency reflects professional standards and builds patient trust.
Download the template provided above and begin using it at your next patient session. If you’re managing multiple practitioners or complex patient populations, book a demo with Pabau to see how digital forms and client records speed up SOAP note creation, keep you compliant, and free your time for patient care.
Setting up your clinical records system? Medical records management explains how to organize, store, and retrieve patient documentation securely.
Streamlining new patient onboarding? Patient intake software shows how to collect history and consent before the first visit.
Designing the intake forms themselves? Adapt this chiropractic intake form template for your own acupuncture practice.
Automating data capture? AI patient intake covers how automation reduces manual data entry at check-in.
An acupuncture SOAP note includes four sections: Subjective (patient-reported symptoms, pain level, onset, chief complaint), Objective (pulse quality, tongue assessment, palpation findings, range of motion), Assessment (clinical diagnosis in TCM and Western terms), and Plan (specific acupoints treated, needling technique, accessory modalities like cupping or e-stim, treatment frequency, and goals). The Plan section should name acupoints by standard abbreviation (e.g. LI4, LV3) rather than vague body regions.
Start with the Subjective section during or immediately after greeting the patient: record their chief complaint in their own words and establish a baseline pain or symptom score. Document your physical examination (pulse, tongue, palpation) in the Objective section. Synthesize these findings into a diagnostic statement in the Assessment section linking clinical data to TCM and Western diagnoses. Finally, in the Plan section, list the exact acupoints treated, needle retention time, any manual stimulation or e-stim, and your intended treatment frequency and outcome goals. Complete the note before the patient leaves to ensure accuracy.
The Objective section documents clinical findings from your physical examination: pulse quality and location (superficial, middle, deep at the radial artery), tongue appearance (color, coating, moisture, shape), palpation of relevant body areas (spine, joints, tender points), range of motion testing if applicable, and any other measurable clinical signs. Unlike the Subjective section (what the patient tells you), the Objective section contains only your direct observations and measurements — findings that another practitioner could independently verify.
Acupuncture SOAP notes emphasize TCM diagnostic methods (pulse, tongue, meridian palpation) in addition to standard Western clinical assessment. The Objective section always includes pulse quality and tongue diagnosis rather than conventional vitals and laboratory values. The Plan section names specific acupoints and TCM treatment principles rather than pharmaceutical interventions. Otherwise, the four-part SOAP structure and clinical logic remain the same: record what the patient reports, what you observe, your clinical conclusion, and your intended intervention.
Yes. Insurance payers reviewing acupuncture claims under CPT codes 97810, 97811, 97813, and 97814 require SOAP notes demonstrating medical necessity, baseline symptom severity, clinical diagnosis, and measurable patient progress. Without complete SOAP documentation showing clinical justification and treatment response, claims are routinely denied. Complete notes reduce denial rates and accelerate reimbursement.