








Blood pressure monitoring: A complete clinical guide
A clinical guide to blood pressure monitoring: home technique, reading categorie...
July 23, 2026
Medical records management covers how clinics collect, store, secure, and dispose of patient health information across its full lifecycle.
HIPAA requires a minimum 6-year retention period in the US; UK NHS guidelines extend this to up to 20 years after the last patient interaction.
Incomplete or disorganized records increase the risk of medical errors and expose clinics to audit failures and legal liability.
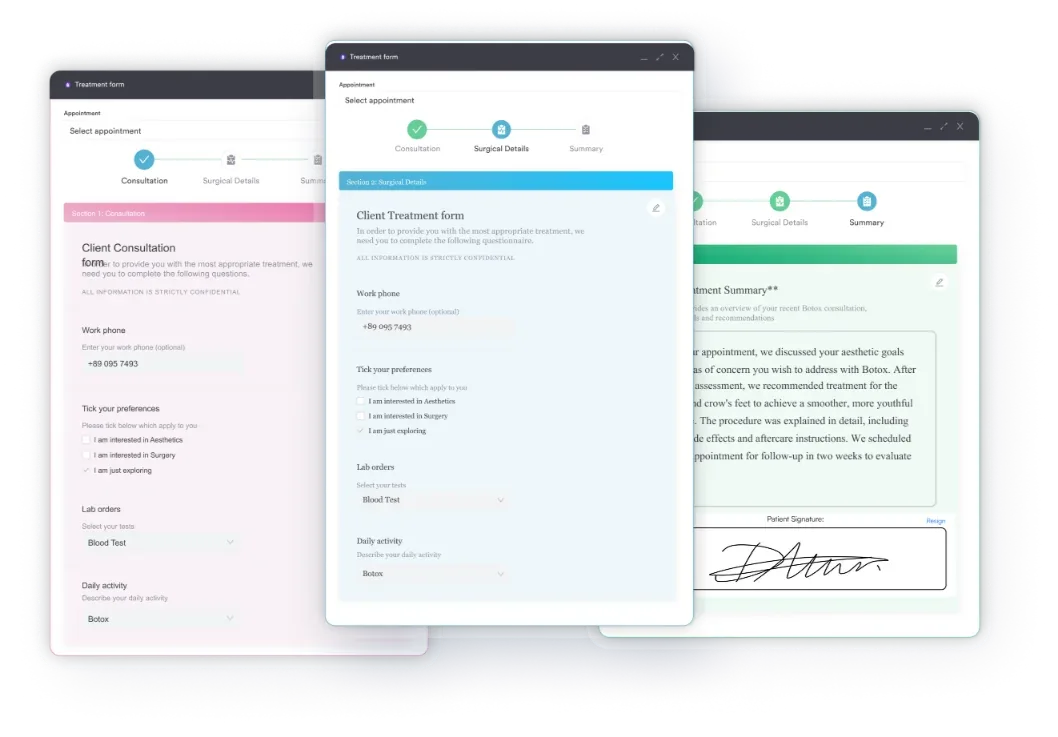
Pabau’s client record management and digital forms replace paper-based workflows with structured, searchable, compliance-ready documentation.
Most clinic owners don’t lose sleep over scheduling or payments. They lose sleep over documentation. A missing consent form before a procedure, a patient record that can’t be located during an audit, a breach notification triggered by a misfiled email. These are the scenarios that medical records management is designed to prevent.
Strong medical records management isn’t just a compliance requirement. It’s what makes continuity of care possible, protects practitioners legally, and gives clinic operators a clear operational picture of every patient journey. This guide covers the core principles, retention rules across key jurisdictions, the shift from paper to digital, and how practice management software makes records workflows faster and safer.
Medical records management is the organized process of creating, maintaining, securing, retaining, and disposing of patient health information throughout its full lifecycle. It spans everything from the moment a patient fills in an intake form to the point where their records are lawfully destroyed decades later.
In practice, the management of medical records covers five stages across the record lifecycle:
The American Medical Association (AMA) describes this obligation as encompassing not only current patients but also retaining older records against possible future need and transferring records to authorized parties on request. In practice, this creates ongoing operational demands for every clinic, regardless of size.
What’s actually at stake when records management breaks down? Three categories of risk:
For small and private practices especially, these risks compound quickly. A solo practitioner managing records in a shared folder has the same compliance exposure as a 50-room hospital. The case for keeping client records up to date is partly clinical, partly legal, and entirely operational.
Retention rules vary significantly by jurisdiction. Getting them wrong in either direction creates problems: retain too little and you lose legal protection; retain too long and you carry unnecessary data liability.
| Jurisdiction | Framework | Minimum Retention Period | Key Notes |
|---|---|---|---|
| United States | HIPAA | 6 years from creation or last effect (whichever is later) | State laws may require longer; always check your state |
| United Kingdom (NHS) | NHS Records Management Code of Practice 2016 | Up to 20 years after last patient interaction | 8 years after death; 25 years for maternity records (last child’s birth) |
| UAE (Dubai) | DHA / NABIDH | Minimum 25 years for adult records | NABIDH framework integrates records across Dubai health facilities |
US clinics often assume the HIPAA 6-year minimum is the only rule they need to follow. It’s not. California requires 7 years; New York requires 6 years for adults but until age 23 for minor patients. Understanding your state’s rules is a prerequisite to building a retention policy. Reading up on HIPAA compliance for medical offices is a practical starting point for US-based clinics.
UK NHS-aligned clinics face a more complex matrix. The 20-year baseline applies to most adult records, but maternity, mental health, and paediatric records carry longer requirements. Private practices in the UK don’t operate under NHS governance directly, but they are subject to UK GDPR and ICO requirements. Running through a UK GDPR compliance checklist is a sensible step for any UK private clinic building or reviewing its records policy.
UAE clinics operating under the Dubai Health Authority (DHA) or Abu Dhabi Department of Health (DOH) must align with NABIDH, the National Backbone for Integrated Dubai Health. NABIDH requires digital records to be accessible across the network and imposes its own retention and interoperability standards. This is a rapidly evolving framework and clinics should verify current DHA guidance directly.
Retention periods are minimums, not maximums. Before destroying any records, confirm both the federal/national minimum AND your local state or regional requirement. When the two conflict, default to the longer period. Then document when and how destruction occurred.
Paper records aren’t just inefficient. They’re a structural liability. A misfiled chart can’t be found in a search. A water-damaged folder can’t be restored. And a stack of manila folders in a locked cabinet can’t be audited, accessed remotely, or transferred to another provider electronically.
The clinical literature is clear on this point. Digital records reduce transcription errors, make records accessible to authorized staff instantly, and create searchable histories that surface relevant information during a consultation. EHR integration for clinics connects records with scheduling, billing, and clinical workflows so that data entered once flows across the entire system.
Three meaningful improvements from switching to digital:
Going paperless in a HIPAA-compliant way requires more than just scanning existing documents. It means building a system where new records are captured digitally from the first patient interaction, stored securely, and retrievable on demand. Clinics that have made this transition report significant reductions in administrative time, even at small scales.
Effective medical records management doesn’t happen by default. It requires deliberate policies, the right tools, and staff who understand why the policies matter. These five practices are where most clinics need to start.
Records inconsistency begins at the front door. When different staff members collect different information at intake, you end up with patient histories that have structural gaps. Standardized digital intake forms capture the same fields for every patient, in the same format, every time. That consistency pays off during audits, when completing referrals, and when reviewing treatment histories.
Every clinic needs a documented policy that covers: minimum retention periods by record type, the approved method for record destruction (shredding for paper, secure deletion for digital), who is authorized to initiate destruction, and how destruction is logged. A policy that exists only in someone’s head is not a policy. It’s a liability.
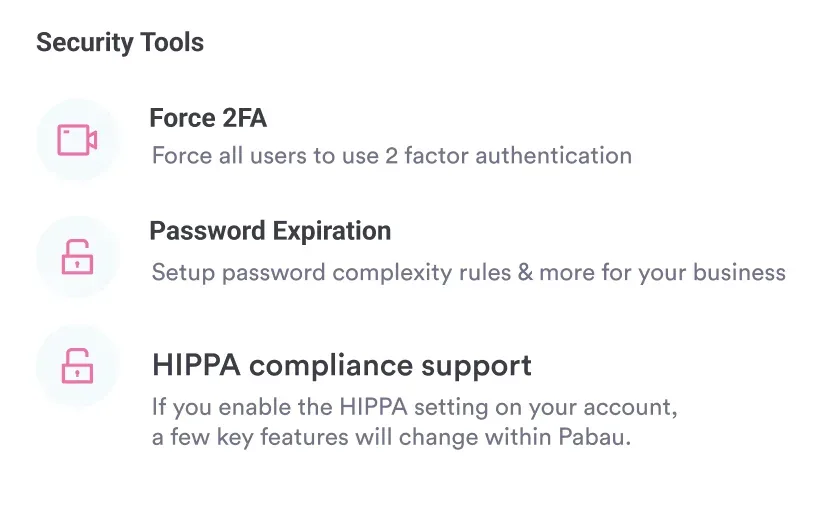
Not every team member needs access to every record. A billing coordinator needs financial data. A treating clinician needs clinical notes. A front-desk team member needs scheduling history. Overly broad access is one of the most common causes of accidental breaches. Review your access permissions and apply the principle of least privilege: each role accesses only what they need to do their job. Reviewing available patient data security tools is a useful starting point for clinics building or revisiting their access model.
Audit your own records before a regulator does. Quarterly spot checks on a sample of patient files can surface gaps in consent documentation, missing signatures, or incomplete clinical notes before they become compliance findings. Build this into the clinic calendar as a standing task.
Every patient request for their records, and every transfer to another provider, should be logged with date, recipient, and authorization. The HHS HIPAA Right of Access guidance requires covered entities to respond to patient access requests within 30 days. That deadline is only trackable if requests are formally documented. Using data protection best practices as a framework helps clinics build systematic processes around records access and transfer.
Pabau gives clinics a single place to capture, store, and manage patient records from intake to audit. Structured forms, compliance-ready documentation, and automated workflows come built in.

Electronic Medical Records (EMR) and Electronic Health Records (EHR) are sometimes used interchangeably, but the distinction matters operationally. An EMR is a digital version of a clinic’s own records for a patient. An EHR is designed to be shared across providers and systems. For most private clinics, the practical question isn’t which term applies. It’s whether their system supports the records workflows they actually need.
Whatever the label, effective electronic medical records management rests on four capabilities that matter most for clinic operators:
The Office of the National Coordinator for Health IT (ONC) provides guidance on interoperability standards that underpin modern EHR systems in the US, including the requirements that apply to clinics participating in federal programs.
Practice management software built specifically for private clinics does more than store records. It makes records management a natural output of normal clinical workflow rather than a separate administrative task.
Pabau’s client record management system gives clinicians a complete, chronological view of every patient interaction: consultations, treatments, prescriptions, consent forms, invoices, and communications. Every record is searchable, timestamped, and accessible to authorized staff based on their role.
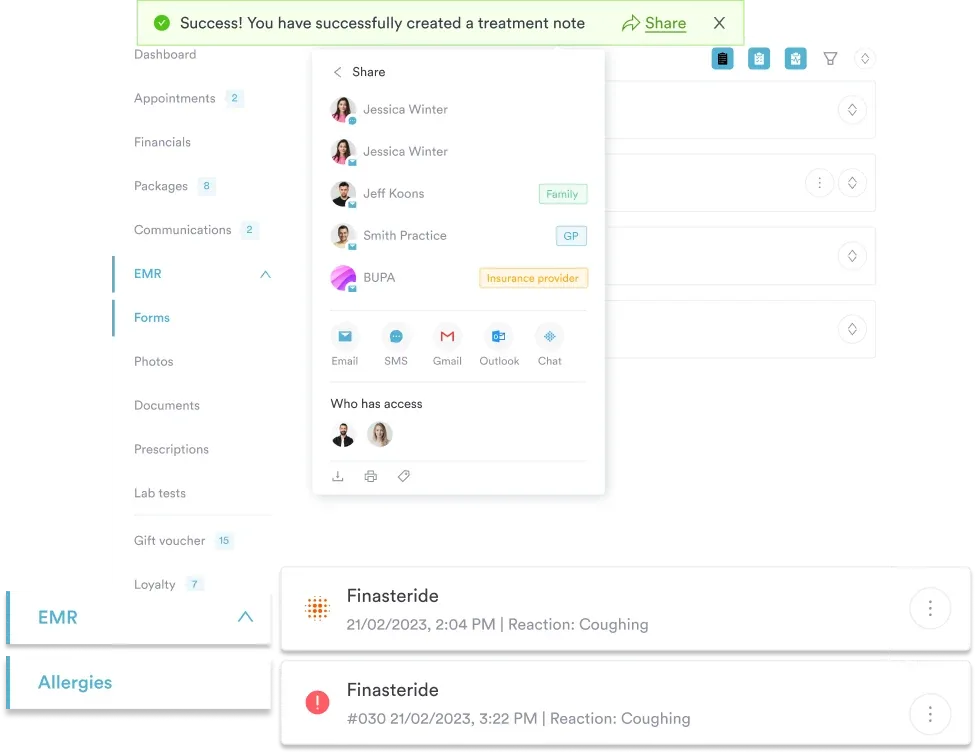
Several features directly address the records management challenges covered in this guide:
Pabau also supports the compliance features clinics need to meet their regulatory obligations. For clinics building or reviewing their compliance posture, Pabau’s compliance management software features are worth reviewing alongside this guide.
When evaluating practice management software for records management, ask the vendor three questions: Can I produce a complete audit trail for any patient record on demand? Can I configure role-based access by job function? And how does the system handle records retention and deletion requests under HIPAA or GDPR? Vague answers to any of these are a red flag.
Clinics that treat records management as an afterthought are carrying risk they can’t see. A missing consent form, an inaccessible record during an audit, or a breach triggered by a permission gap are all documentation failures before they’re compliance failures.
Pabau’s client record management system centralizes documentation, automates compliance workflows, and gives clinic operators the audit trail they need to demonstrate compliance across HIPAA, UK GDPR, and UAE regulatory frameworks. If you’re ready to replace fragmented records processes with a structured, searchable system, see how Pabau’s client records work or book a demo to see it in context.
Need a HIPAA compliance framework for your clinic? HIPAA compliance checklist for primary care covers the documentation and security controls primary care practices need to have in place.
Concerned about how your clinic handles patient data security? HIPAA Security Rule requirements explains the technical safeguards and risk assessment processes that apply to electronic health information.
Thinking about your broader compliance obligations? Med spa compliance provides an overview of the regulatory landscape for aesthetic clinics operating across multiple jurisdictions.
Medical records management is the organized process of creating, maintaining, securing, retaining, and disposing of patient health information across its full lifecycle — from initial intake through to lawful record destruction, governed by policies, technology, and staff training.
HIPAA requires a minimum of 6 years from the date of creation or last effect, whichever is later. State laws may require longer, so always check your state’s rules and default to the longer period.
The five most impactful practices are: standardizing record capture at intake using structured digital forms, maintaining a written retention and destruction policy, implementing role-based access controls, conducting regular internal documentation audits, and formally logging all records requests and transfers.
An EMR (Electronic Medical Record) is a digital record maintained within a single clinic. An EHR (Electronic Health Record) is designed to be shared across multiple providers and systems. The practical question for most private clinics is whether their system supports sharing records externally via standards like HL7 or FHIR.
Digital records are instantly searchable, create a full audit trail for every access and amendment, and can be reached by authorized staff from any location. Integration with scheduling, billing, and clinical tools means records update as part of normal workflow rather than as a separate administrative task.
Most clinics run records through an EHR or EMR, or an all-in-one platform. Practice management software like Pabau keeps records, consent forms, treatment notes, and communications in one patient timeline, with role-based access and a full audit trail built in.



