








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
HCPCS Code J1557 describes injection, immune globulin, (Gammaplex), intravenous, non-lyophilized (e.g., liquid), billed per 500 mg unit administered
Coverage is subject to carrier judgment; prior authorization requirements vary by payer and are not universally mandated by Medicare
Always apply the JW modifier for discarded drug amounts and the JZ modifier to attest zero waste; CMS requires accurate wastage reporting
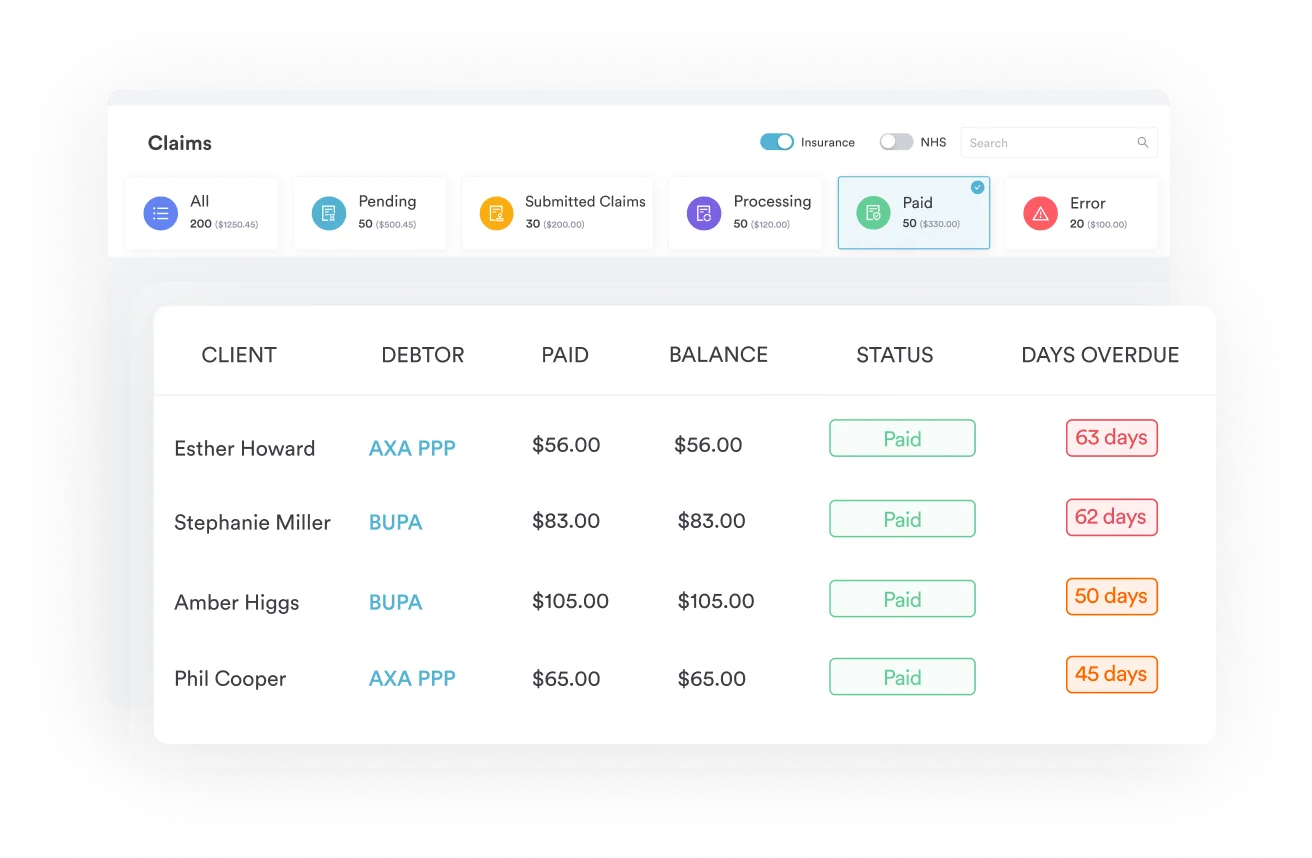
Pabau’s claims management software supports J-code infusion billing workflows, reducing manual errors across multi-location IV therapy practices
HCPCS Code J1557 bills intravenous immune globulin (Gammaplex), non-lyophilized liquid form, at one unit per 500 mg administered. This Level II J-code, maintained by CMS, requires accurate unit calculation, a JW or JZ waste modifier, and a covered ICD-10 diagnosis to avoid payer denials.
Most IVIG billing errors happen before the claim is even submitted. The wrong unit count, a missing modifier, or a mismatched diagnosis code are enough to trigger an immediate denial from Medicare or a commercial payer. For HCPCS Code J1557, getting those details right starts with understanding exactly what the code represents and how its billing rules work.
HCPCS Code J1557 describes: Injection, immune globulin, (Gammaplex), intravenous, non-lyophilized (e.g., liquid), 500 mg. It is a Level II HCPCS J-code maintained by the Centers for Medicare and Medicaid Services (CMS) under the category “Drugs Administered Other than Oral Method.” The code was added to the HCPCS system on January 1, 2012, and remains active without modification changes as of 2026.
This reference covers the full J1557 billing workflow: code properties, unit calculation, Medicare reimbursement methodology, modifier requirements, ICD-10 diagnosis code crosswalk, payer-specific considerations, and common denial patterns.
The “carrier judgment” coverage status is a critical billing signal. It means Medicare does not have a national coverage determination (NCD) specifically governing J1557; instead, individual Medicare Administrative Contractors (MACs) and commercial payers apply their own local coverage determinations (LCDs) and medical policies. Refer to HIPAA-compliant clinic software practices when storing patient records associated with these claims.
Calculating units correctly is where most J1557 claims go wrong. Under-reporting units leaves revenue on the table; over-reporting triggers audits. The billing rule is straightforward: one unit of HCPCS Code J1557 equals 500 mg of Gammaplex administered intravenously.
Gammaplex is available in multiple vial sizes (2.5 g, 5 g, 10 g, and 20 g concentrations). To calculate the correct number of units to report, divide the total dose administered in milligrams by 500.
Report only what was administered, not what was drawn from the vial. If drug was discarded, those milligrams require separate modifier documentation, covered in the modifiers section below. Clinics running infusion programs benefit from claims management software that tracks administered quantities against ordered quantities and pre-populates unit counts before submission.
For practices exploring IV-based therapeutic programs, understanding IV therapy clinic best practices alongside correct J-code billing produces the cleanest revenue cycle outcomes.
Audit your Gammaplex purchase invoices against the units billed on every J1557 claim. Vial sizes and administered doses often do not align, and undocumented variance is the most common trigger for IVIG-related RAC audit targets. Document vial size, lot number, amount drawn, and amount administered in the clinical record for every infusion session.
Under Medicare Part B, HCPCS Code J1557 is reimbursed using the Average Sales Price (ASP) methodology. The standard payment rate is ASP plus 6% of the ASP, which accounts for handling and storage costs under the buy-and-bill model. This percentage is applied to the ASP figure published quarterly in CMS drug pricing files.
Because ASP adjustments occur every quarter, the reimbursement rate for J1557 changes four times per year. Always verify the current quarter’s figure using the CMS Physician Fee Schedule lookup or the CMS ASP drug pricing files before locking in expected reimbursement amounts for budgeting or pre-authorization purposes. For practices considering opening an infusion service, understanding the buy-and-bill margin is also a prerequisite for opening an IV therapy clinic viably.
Two reimbursement pathways exist for Gammaplex infusions. The choice between them significantly affects how the claim is submitted and where the financial risk sits.
Which model your clinic uses determines what appears on the claim. Billing J1557 under the specialty pharmacy model when the drug came from a pharmacy, not your practice, is a common audit flag. Confirm the supply chain with your compliance officer before choosing the billing pathway.
Pabau's claims management tools help IV therapy and infusion clinics track administered drug quantities, apply modifiers automatically, and reduce J-code denials before claims reach the payer.

Modifier compliance is among the most scrutinized areas of IVIG billing. CMS began requiring the JW and JZ modifiers for separately payable drugs like J1557 in 2023. Submitting J1557 claims without the correct modifier now results in claim rejection from many MACs.
Three modifiers apply most frequently to HCPCS Code J1557 billing. Each has a specific and non-interchangeable purpose.
The JW modifier requires documentation in the patient chart specifying the amount of drug drawn, the amount administered, and the amount discarded. Without this documentation, the JW line is unsubstantiated and the claim can be audited or recouped. The AAPC’s HCPCS code reference provides modifier usage guidance alongside the J1557 code entry. Clinics with structured IV therapy intake forms that capture draw and administration amounts are better positioned to support JW modifier claims on audit.
Separate the administered and wasted units on two distinct claim lines: one J1557 line for units administered (no wastage modifier), and one J1557 line with the JW modifier for units discarded. Both lines must reference the same date of service. Never combine administered and wasted units on a single line, and never report wasted units under a different J-code.
Gammaplex (IVIG) has established clinical applications across immunodeficiency and autoimmune conditions. Each qualifying diagnosis must be linked to a valid ICD-10-CM code on the claim. Per CMS Billing and Coding Article A57778, which governs immune globulin billing, providers are responsible for selecting ICD-10 codes at the highest level of specificity from the current year’s code book.
Coverage for HCPCS Code J1557 is conditional on a supported diagnosis. The following ICD-10-CM codes are among the most commonly paired with J1557 claims, though payer-specific LCDs may restrict or expand this list. Always verify covered diagnoses with the applicable MAC or commercial payer policy before submitting.
Off-label use of Gammaplex raises a separate compliance question. Billing J1557 for an indication not recognized by the applicable LCD without prior authorization or medical necessity documentation creates significant audit risk. This is distinct from an unapproved use; many off-label applications have clinical evidence but still lack payer coverage. Document the clinical rationale in the medical record before submitting, and consult the MAC’s LCD for covered diagnosis requirements. For IV therapy EMR workflows, linking diagnosis codes directly to infusion orders at the point of documentation prevents crosswalk errors downstream.
CMS classifies coverage for HCPCS Code J1557 as “carrier judgment,” which places coverage decisions with individual MACs and, for commercial claims, with each plan’s medical policy. There is no national coverage determination (NCD) that definitively establishes Medicare coverage for all uses of Gammaplex. CMS Billing and Coding Article A57778 governs IVIG billing guidance across intravenous formulations and is the primary CMS reference for coverage context.
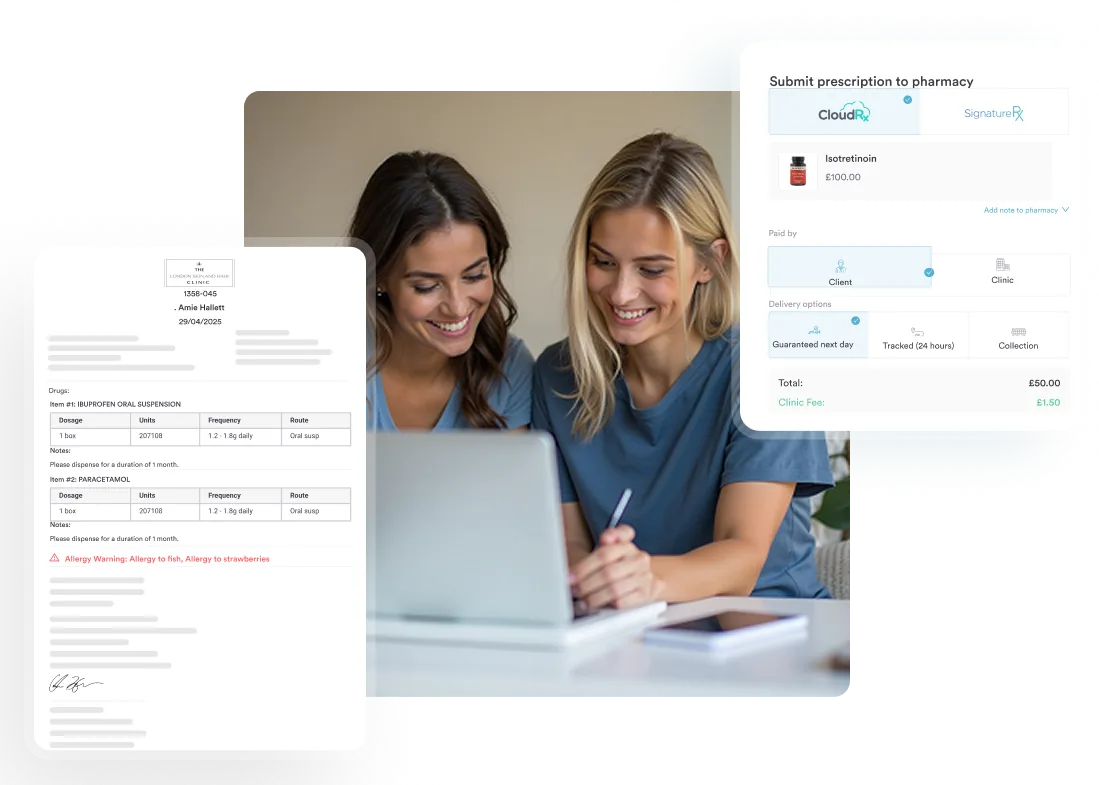
For practices building out infusion programs, understanding state-specific compliance obligations matters before the first patient arrives. Resources like IV hydration business requirements illustrate how payer and regulatory requirements intersect at the operational level. Using prescription and drug management tools that track authorization status per patient ensures no infusion proceeds without verified coverage.
Billing HCPCS Code J1557 requires pairing it with the appropriate infusion administration CPT code. The drug code and the administration code are billed together but are distinct line items. NCCI (National Correct Coding Initiative) edits govern which code pairs are permitted on the same date of service, and violating these edits results in automatic claim denial or bundling downcodes.
Standard infusion administration codes used alongside J1557 include the following. Sequence and timing rules apply depending on whether additional infusions occur in the same session.
Only one initial infusion code (96365) can be billed per encounter, regardless of how many drugs are infused. If Gammaplex is administered after another infusion, it becomes a sequential infusion (96367). Misreporting a sequential as an initial infusion is a frequent NCCI edit trigger. Verify crosswalk compatibility using the CMS list of CPT/HCPCS codes and review the applicable NCCI edits before submitting multi-drug infusion claims. Clinics managing multiple infusion patients daily benefit from mobile IV therapy operations frameworks that standardize encounter documentation and infusion sequencing records.
Even well-prepared J1557 claims get denied. Most denials follow predictable patterns, and understanding their root causes reduces both denial volume and rework time. For practices new to infusion billing or opening an IV therapy clinic, building denial tracking into the intake and billing workflow from day one is more efficient than retrofitting it after the first wave of rejections.
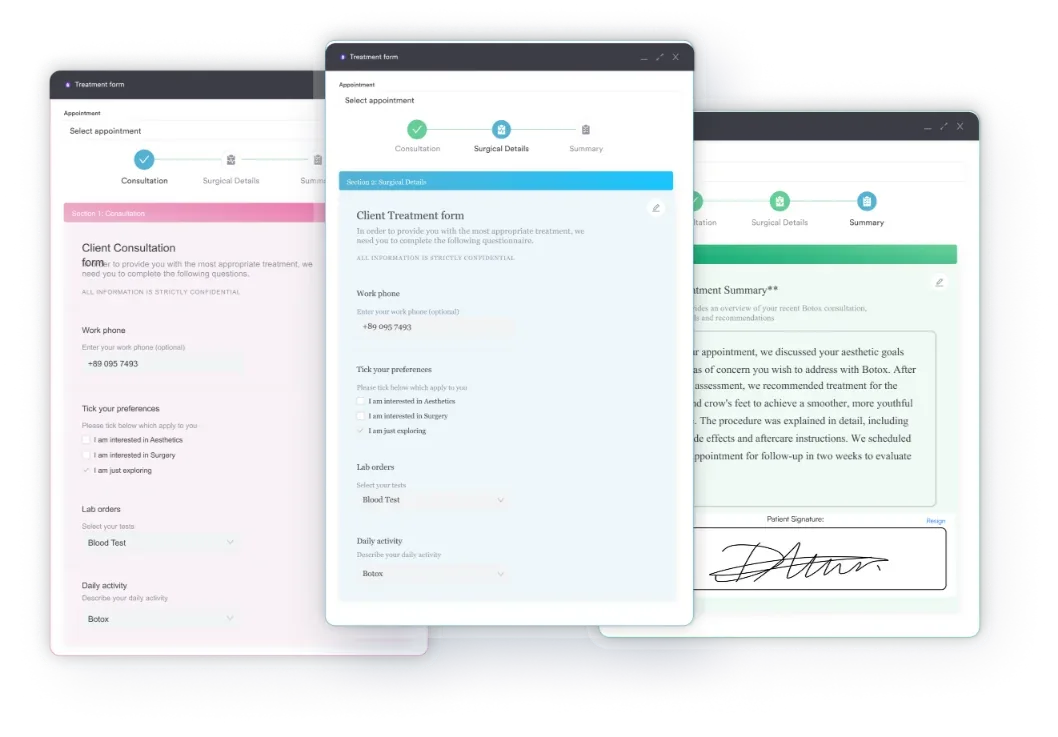
Documentation quality is the single most controllable variable in J1557 denial prevention. Structured digital intake forms that capture immunoglobulin levels, infusion history, and diagnosis context before every session build the audit trail that supports both initial claims and appeal responses. For practices scaling to multiple sites, IV therapy practice management systems that centralize records across locations reduce the inconsistency that drives multi-site denial rates up.
Gammaplex is one of several intravenous immune globulin products with distinct HCPCS J-codes. Using the wrong code, whether J1557 or a related code, for the product actually administered is an impermissible billing practice. Each J-code is brand-specific; the code follows the product, not the generic drug class.
J1599 is the “not otherwise classified” code and should only be used when no brand-specific code exists for the product administered. Using J1599 for Gammaplex when J1557 is the correct code is a coding error that will attract payer attention. The AAPC’s HCPCS code reference maintains current crosswalk data between brand names and their assigned J-codes. Practices managing multiple infusion products benefit from IV therapy clinic best practices that include product-to-code matching protocols for each drug in the formulary. For teams scaling to additional locations, opening an IV therapy clinic guides cover formulary setup and payer enrollment steps.
Billing HCPCS Code J1557 accurately demands attention to four core variables: correct unit calculation per 500 mg administered, the right modifier (JW or JZ) on every claim, a supported ICD-10 diagnosis code that satisfies the applicable LCD, and verified prior authorization before the infusion takes place. Missing any one of them converts a clean claim into a denial or an audit flag.
Pabau’s claims management software supports J-code billing workflows across infusion practices, helping teams track administered quantities, apply modifiers consistently, and catch crosswalk errors before claims leave the system. To see how Pabau handles infusion billing documentation end-to-end, book a demo.
Running an IV infusion clinic and need compliant EMR support? IV therapy EMR software covers how Pabau supports infusion clinic documentation, scheduling, and billing workflows.
Want to understand IVIG intake and documentation requirements? IV therapy intake form guide explains what patient data to capture before every infusion session.
Exploring whether to launch a mobile infusion service? Mobile IV therapy business guide covers regulatory, operational, and billing considerations for off-site infusion delivery.
HCPCS Code J1557 is the Level II HCPCS code for injection, immune globulin, (Gammaplex), intravenous, non-lyophilized (e.g., liquid), 500 mg. Maintained by CMS and active since January 1, 2012, one unit equals 500 mg administered intravenously.
Report 20 units. Divide the total milligrams by 500: 10,000 ÷ 500 = 20. Base the count on the amount administered, not drawn. Use the JW modifier on a separate line for any discarded volume.
Medicare Fee-for-Service has no universal prior authorization requirement, but individual MACs may impose one under local coverage determinations. Medicare Advantage plans typically do require it. Verify with the specific MAC or plan before administering.
Use JW when drug was drawn but a portion was discarded. Use JZ when the entire vial was administered with no waste. One of the two is required on every Medicare J1557 claim since 2023. Document wastage in the clinical record before applying JW.
Yes, if the applicable LCD or payer policy recognizes the indication and coverage is verified in advance. Without a covered diagnosis code and documented medical necessity, the claim will be denied. Check the MAC’s LCD and obtain prior authorization before administering.



