








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
HCPCS Code H2015 describes comprehensive community support services billed in 15-minute increments for individuals with mental health or substance use disorders.
H2015 is primarily a Medicaid code. Medicare coverage varies by state and payer, so always verify reimbursement eligibility before billing.
Common modifiers include AH, AJ, KX, and 99. Incorrect modifier use is one of the leading causes of H2015 claim denials.
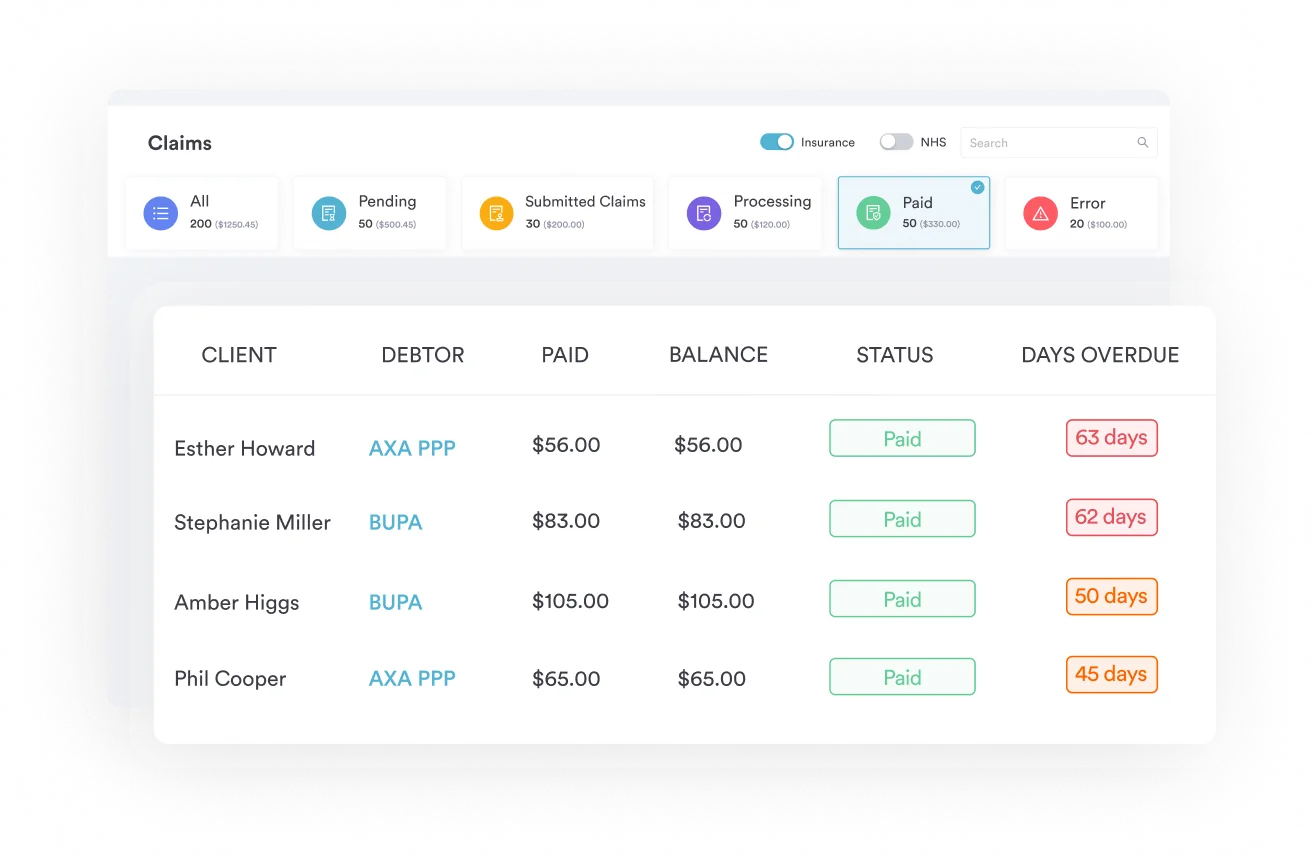
Pabau’s claims management software helps behavioral health organizations track H2015 billing units, attach modifiers, and submit clean claims.
HCPCS Code H2015 describes comprehensive community support services billed in 15-minute increments, primarily under Medicaid, for individuals with mental health or substance use disorders. It’s a Level II HCPCS code, not a CPT code, though the two get confused often enough that some billing guides online mislabel it. This guide covers eligible services, modifiers, documentation, payer coverage, and the billing workflow mental health EMR users and community behavioral health organizations need to submit a clean H2015 claim.
HCPCS Code H2015 has the following official description, as maintained by the Centers for Medicare and Medicaid Services (CMS):
The code falls under HCPCS Level II, a set of codes maintained by CMS to standardize billing for services not captured by CPT codes, including many community-based behavioral health services. For another example of a Level II HCPCS code with specific documentation requirements, see the HCPCS code J9173 billing guide for durvalumab.
H2015 is used primarily by Medicaid-enrolled providers and community mental health centers (CMHCs) to bill for rehabilitative support services delivered in both clinical and community settings.
HCPCS Code H2015 covers a broad range of non-clinical, supportive, psychosocial rehabilitation services. The key distinction from clinical treatment codes (such as H0004 for individual behavioral health counseling) is that H2015 is rehabilitative in nature. It supports the individual’s functional capacity to live and participate in the community, rather than providing direct psychotherapy or medication management.
Covered services under H2015 typically include:
Services are delivered to individuals with mental health disorders and substance use disorders (SUD). For organizations also managing injectable medication billing alongside community support services, see the HCPCS Code J2350 billing guide for ocrelizumab as a reference for pairing drug and service codes.
HEDIS behavioral health quality measures from organizations like CareSource include H2015 alongside H2011, H2012, H2013, H2014, H2017, H2019, and H2020 when measuring community-based behavioral health service utilization.
H2015 is not appropriate for clinical services that require a licensed clinician (therapist, psychiatrist, or prescriber). Those services use separate codes such as CPT codes 90832-90840 for psychotherapy or H0004 for behavioral health counseling.
Provider eligibility to bill H2015 varies by state Medicaid program. Most programs require the billing entity to be enrolled as a Medicaid behavioral health provider. Depending on jurisdiction, qualifying staff often include:
Because staff qualification requirements are set at the state level, a peer support specialist who can bill H2015 in one state may not qualify in another. Always consult your state Medicaid provider manual before assigning H2015 to staff.
Pull your state Medicaid provider manual annually. Staff credential requirements for H2015 change with Medicaid managed care contract renewals. Assign a compliance calendar reminder 90 days before your state’s fiscal year end to review any updates before they affect your billing staff assignments.
Every unit billed must be supported by a corresponding progress note. HIPAA-compliant documentation practices require that notes be completed at or shortly after the time of service. Standardized clinical templates — such as those available for eating disorder worksheets — illustrate how structured documentation captures the goal-linked detail needed to support H2015 claims.
At a minimum, each H2015 service note should capture:
The individual service plan is the clinical anchor for every H2015 claim. Without a current, signed ISP linking the billed service to a specific treatment goal, payers can recoup all related claims on audit. Maintaining patient compliance documentation and a clear audit trail for each session protects revenue during Medicaid managed care organization (MCO) reviews.
H2015 requires a supporting ICD-10-CM diagnosis code on every claim. Commonly paired codes include:
Always select the most specific ICD-10 code available. Using unspecified codes when a more precise code is documented in the clinical record is a common audit trigger. Verify diagnosis codes against the current ICD-10-CM year’s tabular list before billing.
Community support caseloads also include diagnoses outside the table above, including schizotypal disorder (F21), other psychotic disorder (F28), and dissociative and conversion disorder, unspecified (F44.9), particularly for clients with more complex psychiatric histories.
Modifiers communicate additional clinical or administrative context to payers. Incorrect modifier use frequently causes H2015 claims to be denied or returned for additional information. The modifiers most frequently associated with H2015 include:
Modifier requirements for HCPCS Code H2015 differ significantly across state Medicaid managed care plans. A modifier required in Kentucky Medicaid (for example, under Molina Healthcare’s published policy) may not appear in another state’s billing rules. Before adding AH or AJ, confirm with your state Medicaid agency or MCO whether provider-credential modifiers are required or optional for this code.
Pabau's claims management software helps behavioral health organizations log service time in 15-minute increments, attach the right modifiers, and submit clean claims directly from the clinical record. No double entry, no missing units.

HCPCS Code H2015 is primarily a Medicaid code. Medicare does not maintain a standard reimbursement rate for H2015, and coverage through traditional Medicare is limited. The CMS Physician Fee Schedule lookup may return no established rate for H2015, which is a signal that Medicare reimbursement requires specific beneficiary eligibility criteria or a demonstration waiver rather than standard Part B coverage.
Coverage and reimbursement through Medicaid varies substantially by state. Key variables include:
Do not assume that H2015 reimbursement rates are uniform across your state’s MCOs. A single provider credentialed with four Medicaid managed care plans may face four different prior authorization processes, unit caps, and fee schedules for the same HCPCS Code H2015 service.
Knowing where H2015 fits within the H20xx code family helps coders select the right code for each service type. Billing the wrong code from this family is a common cause of denials and overpayment audit findings. Use therapy practice management workflows that clearly distinguish service types at intake.
The most frequent confusion is between H2014 and H2015. H2014 is a more structured, session-based skills training code. H2015 allows for the broader range of community support activities described above.
When a community support worker spends 30 minutes accompanying a client to a job interview and coaching them on communication skills, H2015 is the appropriate code. A structured, classroom-style skills training session in a clinic would more likely be H2014.
For additional context on how per-unit behavioral health codes are structured, the HCPCS Code L1845 billing guide illustrates comparable per-unit billing logic for orthotic devices.
Build a service-to-code crosswalk document specific to your organization. For each service activity your community support workers perform, list whether it maps to H2014, H2015, or another related code. Review it with your compliance team quarterly and update it when your state Medicaid manual changes. This single step prevents the most common upcoding and downcoding audit findings.
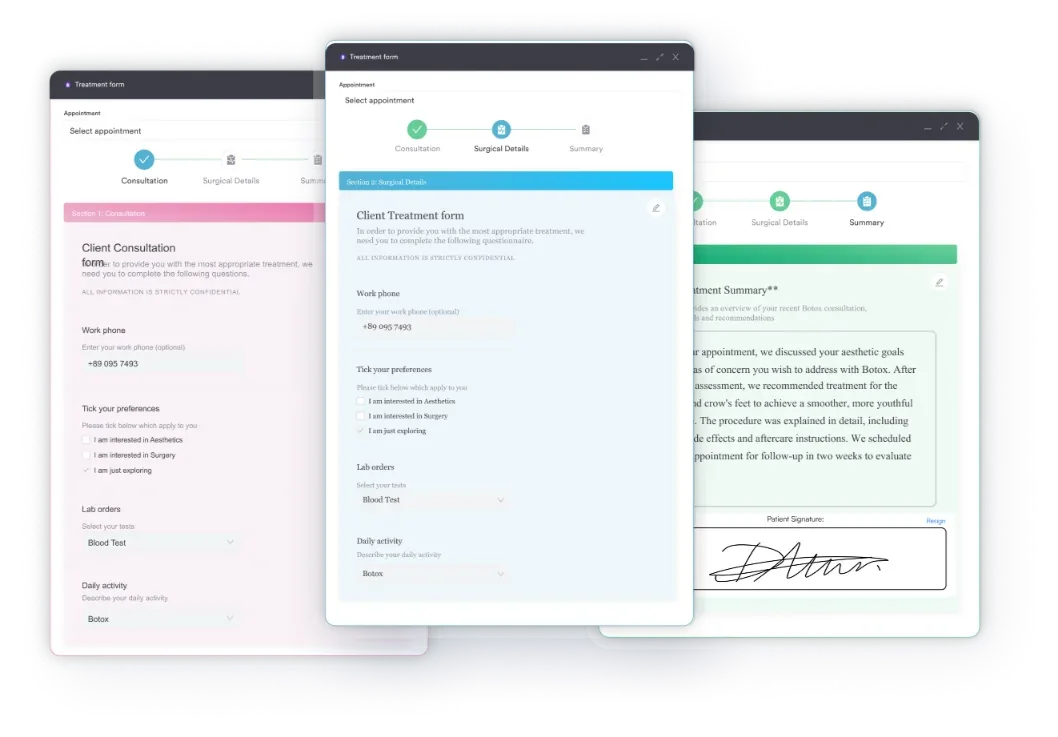
A clean H2015 claim requires accurate data at every step, from intake to submission. Using behavioral health intake forms that capture ISP linkage and service authorization details at the point of care reduces rework and prevents the documentation errors that drive denials.
Integrating this workflow into your claims management software means coders don’t need to cross-reference paper logs. Service time, provider credentials, and ISP linkage should flow directly from the clinical record to the claim, reducing the manual entry errors that inflate denial rates.
Billing teams that handle H2015 regularly encounter the same denial patterns. Knowing them in advance lets you build preventive workflows rather than reactive appeals.
Building denial tracking into your EHR integration for behavioral health workflows surfaces these patterns quickly. When the same denial reason appears three or more times in a 30-day period, it indicates a systemic documentation or authorization problem, not a one-off coding error.
There is no single national Medicaid rate for HCPCS Code H2015. Reimbursement is set at the state level, and managed care organization rates may differ from the state fee-for-service schedule. To find your applicable rate, consult:
Because rates are per 15-minute unit, a one-hour community support session generates four units of H2015. The aggregate daily revenue per client depends on authorized hours, applicable unit caps, and the MCO’s contracted rate. Tracking these variables for each payer contract separately, rather than averaging across payers, is the only reliable way to manage H2015 revenue accurately.
Manual billing workflows for per-unit codes like H2015 create significant administrative burden. Community mental health organizations often have dozens of community support workers generating H2015 claims daily, each requiring time tracking, ISP linkage, modifier assignment, and payer-specific rule application.
Time-saving tools for private practices and community behavioral health organizations share a common principle: reduce the number of manual steps between a delivered service and a submitted claim.
Pabau’s platform supports this through digital intake forms that collect ISP-linked service data at the point of care. It also builds in automated audit trails for compliance reviews and structured progress note templates that capture all required H2015 documentation fields.
For organizations billing H2015 across multiple locations or for large caseloads, integrating time tracking directly with the clinical record eliminates the unit calculation errors that frequently inflate denial rates. When a community support worker logs a 45-minute session, the system calculates 3 billable units automatically, rather than relying on manual conversion by a billing clerk reviewing handwritten time sheets.
HCPCS Code H2015 is one of the most heavily utilized codes in community behavioral health billing, and one of the most frequently denied. Understanding related mental health diagnosis coding — such as ICD-10 code F22 for delusional disorders — helps build complete and accurate claims.
The per-15-minute unit structure, state-specific payer rules, ISP documentation requirements, and modifier variability combine to create a billing environment where small process errors produce large revenue losses.
Pabau’s automated billing workflows help behavioral health organizations standardize H2015 documentation, track time-based units accurately, and reduce the manual steps that drive claim errors. To see how Pabau can support your community behavioral health billing team, book a demo.
Need a structured approach to mental health documentation? Psychiatric evaluation template provides a step-by-step framework for comprehensive mental health assessments and clinical note structure.
Looking to streamline behavioral health practice operations? Behavioral health practice management software comparison breaks down seven platforms built for behavioral health providers.
Want to understand HIPAA compliance for your clinical documentation? HIPAA compliance for clinic software explains the documentation and system requirements for behavioral health practices.
HCPCS Code H2015 is a Level II HCPCS code for “Comprehensive community support services, per 15 minutes,” used to bill Medicaid for non-clinical, rehabilitative behavioral health services delivered to individuals with mental health or substance use disorders. It was added to the HCPCS code set on April 1, 2003, and remains valid for 2026.
H2015 is billed per 15-minute unit, not per session. A 60-minute community support visit generates 4 billable units. Most payers round down to the nearest complete 15-minute increment, so a 50-minute session typically generates 3 units. Verify the rounding rule with each Medicaid managed care organization before billing.
H2015 is primarily a Medicaid code. Medicare does not maintain a standard reimbursement rate for H2015 under the Physician Fee Schedule, and coverage through traditional Medicare Part B is limited. Check with your Medicare Administrative Contractor or state Medicaid agency for any applicable demonstration waiver coverage.
H2014 covers structured skills training and development, typically delivered in a clinical setting in a defined session format. H2015 covers broader comprehensive community support services, including community integration, resource linkage, daily living skills coaching, and crisis prevention support delivered in community settings. When a community support worker accompanies a client in the community rather than conducting a structured training session, H2015 is the appropriate code.
Every H2015 claim requires a progress note with start and stop times, the provider’s name and credentials, a description of services tied to the active individual service plan (ISP), client response to the intervention, location of service, and a supporting ICD-10-CM diagnosis code. An active, signed ISP is required; claims billed without a current ISP are subject to denial and recoupment.
Commonly paired ICD-10-CM codes include F20.9 (schizophrenia, unspecified), F31.9 (bipolar disorder, unspecified), F32.A (depression, unspecified), F41.1 (generalized anxiety disorder), F11.20 (opioid dependence, uncomplicated), and F10.20 (alcohol dependence, uncomplicated). Always select the most specific code documented in the clinical record to support medical necessity.
H2015 is an HCPCS Level II code, not a CPT code. CPT codes make up HCPCS Level I, the numeric codes (like 90837 for psychotherapy) most clinicians already know. H2015 sits in Level II, the alphanumeric codes CMS created for services CPT doesn’t cover, which is why some billing guides mislabel it “CPT H2015.” Level III, a set of state-specific codes, was retired in 2003, leaving Levels I and II as the only ones in active use today.



