








ICD-10 Code M45.6: Ankylosing spondylitis lumbar region
ICD-10 Code M45.6 is the billable ICD-10-CM diagnosis code for ankylosing spondy...
Last Updated: August 3, 2026
HCPCS Code G8510 reports a negative depression screening result with no follow-up plan required, effective since January 1, 2009 and valid for 2026 claims.
G8510 satisfies QPP Measure 134 ‘Performance Met’ for the Screening for Depression and Follow-Up Plan quality measure under CMS.
Bill G8431 (not G8510) when screening results are positive and a follow-up plan is documented – the most common selection error.
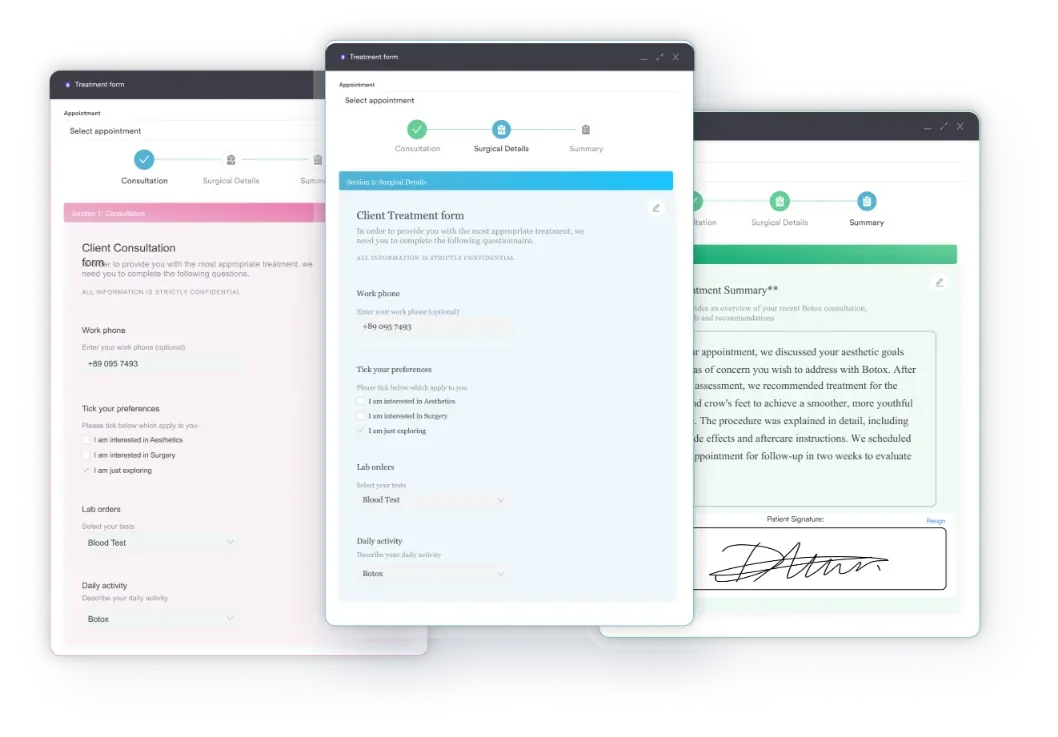
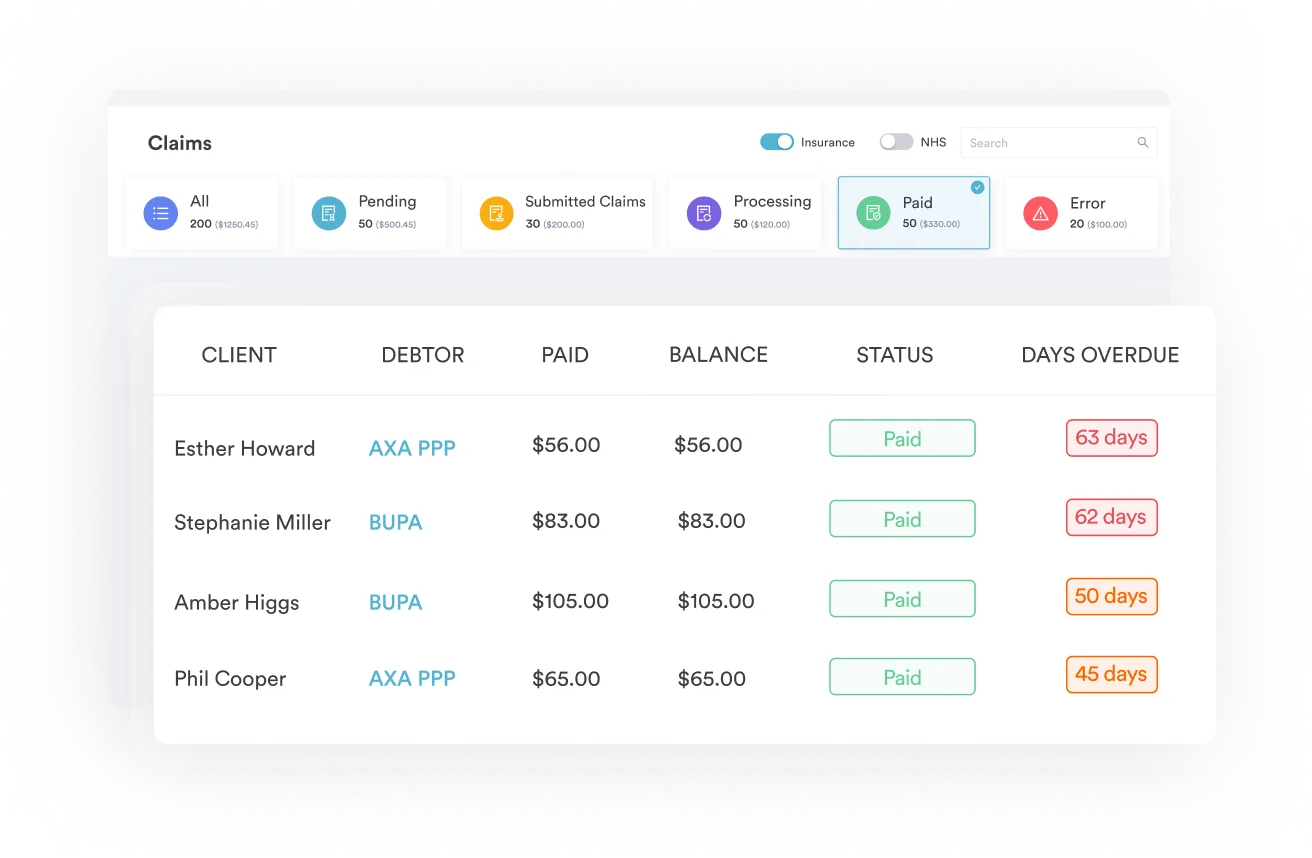
Practice management software like Pabau supports structured depression screening documentation with claims management tools and digital forms, reducing G8510 claim denials.
HCPCS Code G8510 reports that a depression screening was completed and came back negative, with no follow-up plan required. It is a quality data code for CMS Quality Payment Program Measure 134, not a code that generates separate payment. This guide covers what G8510 documents, how it differs from G8431, the Measure 134 reporting rules, and the modifiers and documentation that keep claims clean.
Most claim denials involving depression screening codes trace back to the same root cause: providers bill a code that doesn’t match what they actually documented. Mental health EMR workflows that automate screening capture can prevent the most common G8510 errors before submission.
Specifically, HCPCS Code G8510 is the billing code used when a patient is screened for depression and the result is negative, with no follow-up plan required. The official long description reads: “Screening for depression is documented as negative, a follow-up plan is not required.”
CMS (Centers for Medicare and Medicaid Services) maintains the code under the HCPCS Level II G-code category for additional quality measures. Visit the CMS HCPCS resource page for the full code set.
Additionally, CMS added the code on January 1, 2009 and assigned it Action Code N, meaning CMS does not actively maintain or update it. It remains valid for 2026 billing.
In practice, selecting between G8510 and G8431 is the single most consequential coding decision in depression screening billing. The codes are mirror images of each other: one reports a negative result, the other a positive.
Both codes satisfy QPP Measure 134 when properly documented. The error pattern coders report most is billing G8510 for a visit where the patient scored above the PHQ-2 or PHQ-9 threshold but the follow-up plan wasn’t documented. That visit requires G8431, not G8510. Billing G8510 in that scenario creates a documentation mismatch that payers can audit.
For example, the PHQ-2 is the most common first-line screening tool triggering G8510. A score of 2 or below typically indicates a negative screen. The PHQ-9 serves as a secondary confirmatory tool when initial PHQ-2 scores are borderline.
Your documentation must record both the tool used and the score that led to the negative determination — the same standard that applies when a positive result is billed under G8431.
Document the specific screening tool (PHQ-2, PHQ-9, or equivalent validated instrument), the numeric score, and the clinical determination (negative) in the same encounter note. Generic statements like ‘patient screened for depression, no concerns’ are insufficient for audit purposes.
HCPCS Code G8510 is a performance measure code, not a procedure code. Its primary function is Quality Payment Program (QPP) reporting under QPP Measure 134 specifications for Screening for Depression and Follow-Up Plan.
Specifically, when a provider submits G8510 on a Medicare Part B claim alongside an eligible E&M or preventive care service, it signals to CMS that Measure 134 was met for that patient encounter. This contributes to MIPS performance scoring for eligible clinicians. Psychiatry billing workflows that integrate quality measure tracking can automate this process across payer types.
In particular, Annual Wellness Visits are a high-volume trigger for G8510. CMS requires depression screening as a component of the AWV, making G8510 (or G8431) a standard attachment to G0438 and G0439 claims. Providers who conduct AWVs without appending the depression screening result code are leaving QPP credit on the table and creating incomplete quality reporting.
In most cases, claim denials for G8510 trace back to incomplete encounter documentation. Payers auditing these claims look for four specific elements — the same level of structured detail built into other standardized intake templates, such as an opioid risk assessment.
Using digital intake forms that capture PHQ-2 or PHQ-9 responses directly into the patient record eliminates transcription errors and creates a structured data trail that supports G8510 documentation automatically. Furthermore, HIPAA-compliant documentation practices also require that screening results be stored securely as part of the permanent encounter record.
Notably, practices billing G8510 for maternal depression screening may have an additional modifier requirement depending on the payer. This is covered in detail in the modifier section below.
Pabau's digital forms capture PHQ-2 and PHQ-9 results directly into the patient record, so your G8510 documentation is always complete and audit-ready.

Submit G8510 on the same claim line as the qualifying service, not as a standalone billable procedure. A few payer-specific rules affect how it’s reported.
Importantly, G8510 does not generate a separate payment line. It appends to the primary E&M code (99202-99215), AWV code (G0438, G0439), or preventive visit code (99381-99397) on the same date of service. Payers read it as a quality measure addendum, not an additional service. Submitting it on a separate claim line from the qualifying E&M is a common denial trigger.
As a result, strong claims management software flags this bundling rule automatically, ensuring G8510 attaches correctly to the parent service line before submission. Good compliance management tools also track QPP measure reporting across your patient population so no eligible encounters are missed.
Under statewide Medi-Cal (DHCS) policy, modifier HD on G8431 or G8510 has been allowable but optional since July 1, 2020, per the official Medi-Cal NewsFlash on modifier updates. Its absence does not trigger a denial under that policy.
Individual Medi-Cal managed care plans, such as San Francisco Health Plan (SFHP), may still ask providers to append HD to flag the maternal population, so the actual requirement depends on which plan processes the claim. Some other payers mandate it outright: EmblemHealth requires modifier HD on positive maternal screens billed with G8431, while certain BCBS plans use modifier U8 instead.
Always verify modifier requirements with your specific state Medicaid agency, managed care plan, or payer before billing — HD is not a universal requirement, but plan-specific rules and other payers’ mandates still apply. Patient compliance strategies make it easier to build maternal depression screening into the routine intake workflow, keeping the billing step consistent.
The Illinois Department of Healthcare and Family Services (HFS) added G8510 and G8431 to its fee schedule effective April 1, 2023, per a Meridian Health Plan claims notice from July 2023.
Providers billing these codes to Illinois Medicaid managed care plans should verify current coverage with their specific plan administrator, since coverage and modifier requirements in state Medicaid programs can differ from Medicare guidance.
Run a monthly audit of G8510 claims submitted without an accompanying qualifying E&M or AWV code. These claims reliably deny, and the pattern often indicates a workflow breakdown in how coders attach the performance measure code to the parent service line.
CMS does not publish a standard national facility or non-facility reimbursement rate for G8510 in 2026. The CMS Physician Fee Schedule lookup returns no RVU values or payment amounts for this code.
However, this is expected behavior for a performance measure G-code. G8510 exists to report quality measure compliance, not to generate a separate payment event.
The economic value it delivers comes through QPP MIPS performance scores, which affect Medicare payment adjustments for eligible clinicians. A strong MIPS performance score can increase Medicare payments by a percentage that exceeds what any single procedural code would generate.
Beyond Medicare, Medicaid and private payer reimbursement rates vary by plan and state. Contact individual payers directly to confirm whether G8510 generates a separate line-item payment in their fee schedule.
Some state Medicaid programs do reimburse G8510 as part of depression screening quality initiative payments. Illinois Medicaid and Medi-Cal are examples of state programs that have specifically added these codes to their coverage policies.
Consistent clinical documentation practices for depression screening carry over to other behavioral health billing scenarios, since payers apply the same audit standard across co-occurring condition codes. A purpose-built behavioral health EHR that integrates QPP tracking reduces the manual overhead of quality measure reporting for mental health-focused practices.
Importantly, G8510 does not operate in isolation. Four additional HCPCS codes complete the depression screening code set under QPP Measure 134, each covering a different clinical scenario.
Providers who leave the reason undocumented when a screening isn’t completed report G8432, a Performance Not Met outcome that negatively affects MIPS scoring.
When a patient declines screening or a medical reason prevents it, document that reason explicitly and report G8433 instead, which counts as a Denominator Exception rather than a Performance Not Met result. Verify current codes against AAPC’s HCPCS code lookup for the current measurement year’s specifications.
G8510 denials cluster around three root causes. Knowing them in advance turns a reactive denial management process into a front-end quality check.
Similarly, the Illinois Medicaid-specific denial pattern differs: practices in Illinois that began billing G8510 and G8431 before April 1, 2023 encountered systematic denials because HFS had not yet covered these codes.
If claims from that period are still outstanding, verify coverage dates with your managed care plan before resubmitting. Medical practice compliance reviews that include coding accuracy audits catch these historical billing issues before they age past the timely filing window.
Overall, HCPCS Code G8510 is a narrow, high-stakes code: one documentation mismatch separates a clean QPP Measure 134 submission from a payer denial or MIPS performance shortfall. The code works correctly only when the encounter note records the validated screening tool, the numeric score, the negative determination, and the absence of a required follow-up plan.
Pabau’s digital forms capture structured PHQ-2 and PHQ-9 responses directly in the patient record, giving your billing team the audit trail G8510 requires. To see how Pabau handles depression screening documentation and quality measure reporting across your practice, book a demo.
Need a structured mental health assessment workflow? Psychiatric Evaluation Template provides a step-by-step framework for comprehensive mental health assessments in clinical practice.
Looking for a practice management platform built for mental health? Mental health EMR software covers the scheduling, documentation, and billing features behavioral health practices need.
Want to understand HIPAA documentation obligations? HIPAA compliance for clinic software explains how to keep patient records secure and audit-ready across your practice.
HCPCS Code G8510 is a performance measure code used to report that a patient was screened for depression using a standardized tool, the result was negative, and no follow-up plan is required. It satisfies the “Performance Met” outcome for CMS QPP Measure 134 on Medicare Part B claims.
G8510 reports a negative depression screening result with no follow-up plan required, while G8431 reports a positive result where a follow-up plan has been documented. Both satisfy QPP Measure 134 “Performance Met,” but selecting the wrong code creates a documentation mismatch auditors can flag.
No. CMS does not publish a standard national facility or non-facility reimbursement rate for G8510 in 2026. The code’s value is indirect: it contributes to MIPS performance scoring under QPP Measure 134, which affects Medicare payment adjustments for eligible clinicians. Some state Medicaid programs may reimburse it separately.
Modifier HD is optional, not required, under statewide Medi-Cal policy since July 1, 2020 — its absence does not trigger a denial. Some managed care plans, such as San Francisco Health Plan, still ask providers to append it to flag the maternal population, and a few other payers, like EmblemHealth, require it outright. Confirm the rule with your specific plan before billing.
Yes. G8510 is a HCPCS Level II G-code classified as a performance measure code maintained by CMS. It does not represent a standalone billable procedure; it appends to an eligible E&M or preventive care code on the same claim to report quality measure compliance for QPP Measure 134.
The encounter note must record the validated screening tool used (e.g., PHQ-2, PHQ-9), the numeric score, an explicit clinical determination that the result is negative, and a statement that no follow-up plan is clinically required. All four elements should appear in the same encounter note as the qualifying E&M or preventive visit.
G8510 is a HCPCS Level II quality data code, not a CPT code — it is often searched as a “G8510 CPT code,” but CPT codes describe the visit or screening service while G8510 records the quality-measure result. It carries no separate payment and reports Measure 134 compliance.
Yes. Measure 134 applies to patients aged 12 and older at the time of the eligible encounter, so G8510 is reported for those patients when a screening is negative and no follow-up is required. Confirm the current age denominator in the active measure specification before reporting.



