ICD-10 Code M32.9: Systemic lupus erythematosus, unspecified
M32.9 codes SLE when the notes name no organ involvement. Treat it as the fallba...
Last Updated: August 3, 2026
ICD-10 Code H90.6 describes mixed conductive and sensorineural hearing loss, bilateral, meaning both ears show both conductive and sensorineural components simultaneously.
H90.6 is a billable ICD-10-CM code valid for 2026 reimbursement; documentation must explicitly state bilateral presentation and both loss types to avoid claim denial.
Coders often confuse H90.6 with H90.8 (unspecified mixed) or H90.7 (unilateral mixed); selecting the wrong code without bilateral documentation is a common audit trigger.
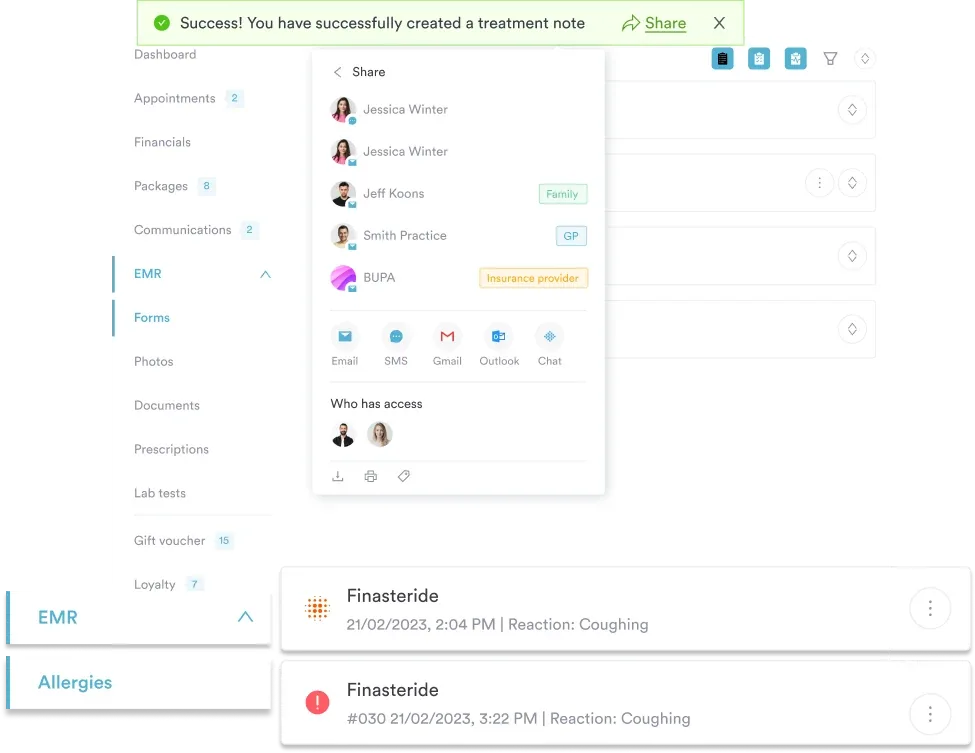
Practice management software like Pabau helps audiology and ENT practices document bilateral mixed hearing loss precisely and submit cleaner claims through structured forms and integrated billing.
H90.6 is the ICD-10-CM code for bilateral mixed conductive and sensorineural hearing loss, the diagnosis of mixed hearing loss affecting both ears. The term “mixed” means the patient has hearing loss arising from two distinct pathological mechanisms at the same time: a conductive component (a mechanical problem in the outer or middle ear) and a sensorineural component (damage to the inner ear or auditory nerve). “Bilateral” means this combination is present in both ears, not just one.
Conductive hearing loss occurs when sound cannot efficiently travel through the outer or middle ear structures, including the auditory canal, tympanic membrane, or ossicles. Sensorineural hearing loss arises from damage to the cochlea or the eighth cranial nerve. When both mechanisms are active simultaneously, pure-tone audiometry shows an elevated bone-conduction threshold alongside an air-bone gap, confirming the mixed nature of the loss.
Common clinical causes include chronic otitis media with secondary cochlear damage, otosclerosis with sensorineural involvement, and noise-induced sensorineural loss compounded by middle-ear pathology. Accurate diagnosis requires a full audiological evaluation, typically including pure tone average (PTA) testing, tympanometry, and speech discrimination assessment.
H90.6 sits within the H90 category, the group that holds every bilateral hearing loss ICD-10 code alongside the unilateral and unspecified options. If you are hunting for the ICD 10 code for bilateral hearing loss and the record shows both a conductive and a sensorineural component, H90.6 is the specific code the hierarchy points to. Reading the hierarchy this way helps coders pick the right level and avoid under-coding with a less specific parent code. The ICD-10-CM classification system requires the most specific code supported by clinical documentation.
The H90 category falls under the larger block H60-H95 (Diseases of the ear and mastoid process), which in turn belongs to Chapter 8 of ICD-10-CM. According to the WHO’s ICD-10 browser, this block groups all conditions affecting ear anatomy and function.
The H90 category structure is as follows:
H90.6 is a terminal (leaf) code in this hierarchy. No additional digits refine it further. This contrasts with H90.7, which has sub-codes specifying whether the affected ear is right or left.
The neighboring codes matter when only one loss type is present. If the record supports the bilateral conductive hearing loss ICD 10 scenario with no nerve involvement, H90.0 applies, not H90.6. For a bilateral sensorineural hearing loss ICD 10 picture with no air-bone gap, the sensorineural-only codes fit instead, starting with H90.3 for bilateral involvement. H90.6 is reserved for cases where both mechanisms are documented in both ears.
Incomplete documentation is the leading cause of claim denial when coding H90.6. Payers require the medical record to support every element of the code before approving reimbursement. Three documentation elements are non-negotiable.
Clinicians should attach or reference audiometric reports, including pure tone average values and air-bone gap measurements, in the clinical note. The CMS ICD-10-CM coding guidelines consistently emphasize that the highest level of specificity supported by the record is required.
For ENT and audiology practices, structured digital intake forms that capture laterality, audiogram results, and both conductive and sensorineural findings at the point of care significantly reduce documentation gaps before claims are submitted.
Pabau helps audiology and ENT practices capture structured clinical notes, audiogram data, and bilateral documentation at the point of care so H90.6 and related codes are always supported before submission.

Selecting the wrong code in the H90 mixed hearing loss group is a frequent source of audits. The differences between H90.6, H90.7, and H90.8 are clinically meaningful and payer-distinguishable. Using H90.8 when documentation supports H90.6 constitutes under-coding and can trigger downcoding adjustments.
The key coding decision point: if the record documents bilateral loss with both air-bone gap and elevated bone conduction, ICD-10 Code H90.6 is correct. If only one ear has mixed loss and the other is normal, H90.7 applies. If laterality is genuinely absent from the documentation, H90.8 is acceptable but should prompt a documentation query to the clinician. The ICD List lookup tool provides a quick reference for comparing H90 sub-codes and their applicable-to notes.
Before finalizing H90.6, run a quick three-question check: (1) Does the note state bilateral? (2) Is an air-bone gap documented, confirming the conductive component? (3) Are bone-conduction thresholds elevated, confirming the sensorineural component? If all three are yes, H90.6 is supported. If laterality is missing, query the provider before submission.
H90.6 functions as a diagnosis code, not a procedure code. It identifies the condition being treated and supports medical necessity for the associated audiology or ENT procedures billed on the same claim. Sequencing rules determine whether H90.6 is coded as the principal diagnosis or a secondary diagnosis.
When the primary reason for the encounter is evaluation and management of bilateral mixed hearing loss, H90.6 is the principal diagnosis. When the encounter targets a specific underlying cause (for example, otosclerosis coded as H80.x), the underlying condition may be sequenced first, with H90.6 as an additional code. The CDC/NCHS ICD-10-CM web tool provides the official tabular list guidance on sequencing instructions for the H90 category.
ICD-10-CM Official Guidelines state that when coding a condition that clinicians describe as both conductive and sensorineural, coders should assign a code from H90 that captures the combined nature, rather than coding each component separately. H90.6 satisfies this requirement for the bilateral presentation, which is why the conductive and sensorineural hearing loss ICD 10 assignment collapses into one combined code rather than two separate ones. Practices using structured patient record systems that flag audiogram data automatically can reduce the manual review step for sequencing decisions.
The H90 category carries Type 1 Excludes notes that prevent certain codes from being used with H90.6:
There are no Type 1 Excludes notes that prevent H90.6 from being coded alongside underlying etiology codes (such as otosclerosis H80.x, chronic suppurative otitis media H66.x, or otitis media in diseases classified elsewhere, H67.9). Coders should use H90.6 alongside the appropriate etiology code when documentation supports both. For practices integrating HIPAA-compliant documentation workflows, the HIPAA compliance standards for medical offices apply equally to how audiometric records and diagnosis codes are stored and transmitted.
H90.6 does not generate a claim on its own. It must be paired with a CPT procedure code that reflects the service rendered. The following CPT codes are most frequently submitted alongside H90.6 in audiology and ENT settings. Practices can use the AAPC Codify ICD-10-CM lookup to verify crosswalk relationships before claim submission.
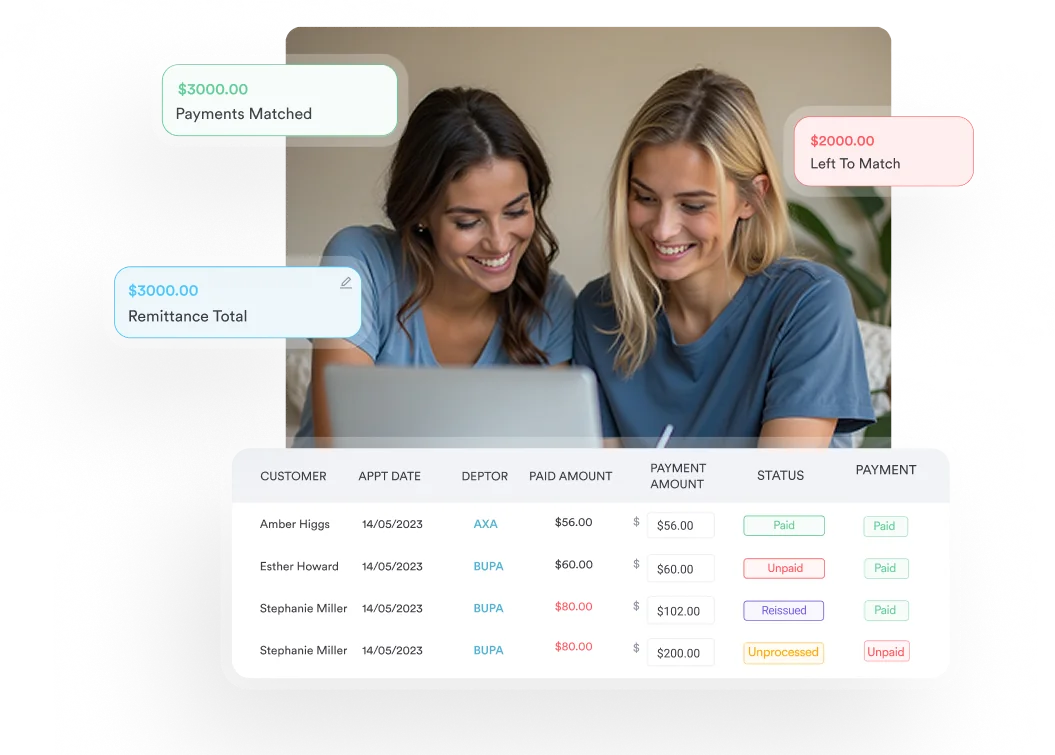
Cochlear implant candidacy is a specific context where H90.6 appears frequently. When a patient presents with bilateral mixed hearing loss and is being evaluated for cochlear implant suitability, H90.6 supports the medical necessity documentation for both the evaluation (CPT 92626) and any subsequent implant procedure. An integrated claims management workflow that links diagnosis codes to procedure codes at the point of order entry can flag mismatches before submission rather than after denial.
For cochlear implant candidacy evaluations, verify that H90.6 appears on all claims in the evaluation pathway, not just the initial diagnostic visit. Payers auditing cochlear implant authorizations will review the full diagnostic record for consistent bilateral mixed hearing loss documentation across multiple encounters.
Coding accuracy for H90.6 is ultimately a documentation workflow problem as much as a coding knowledge problem. Most denials occur not because coders select the wrong code but because the clinical documentation did not capture all required elements before they built the claim. ENT and audiology practices benefit from structured workflows that prompt clinicians to document laterality and both hearing loss components at the point of care.
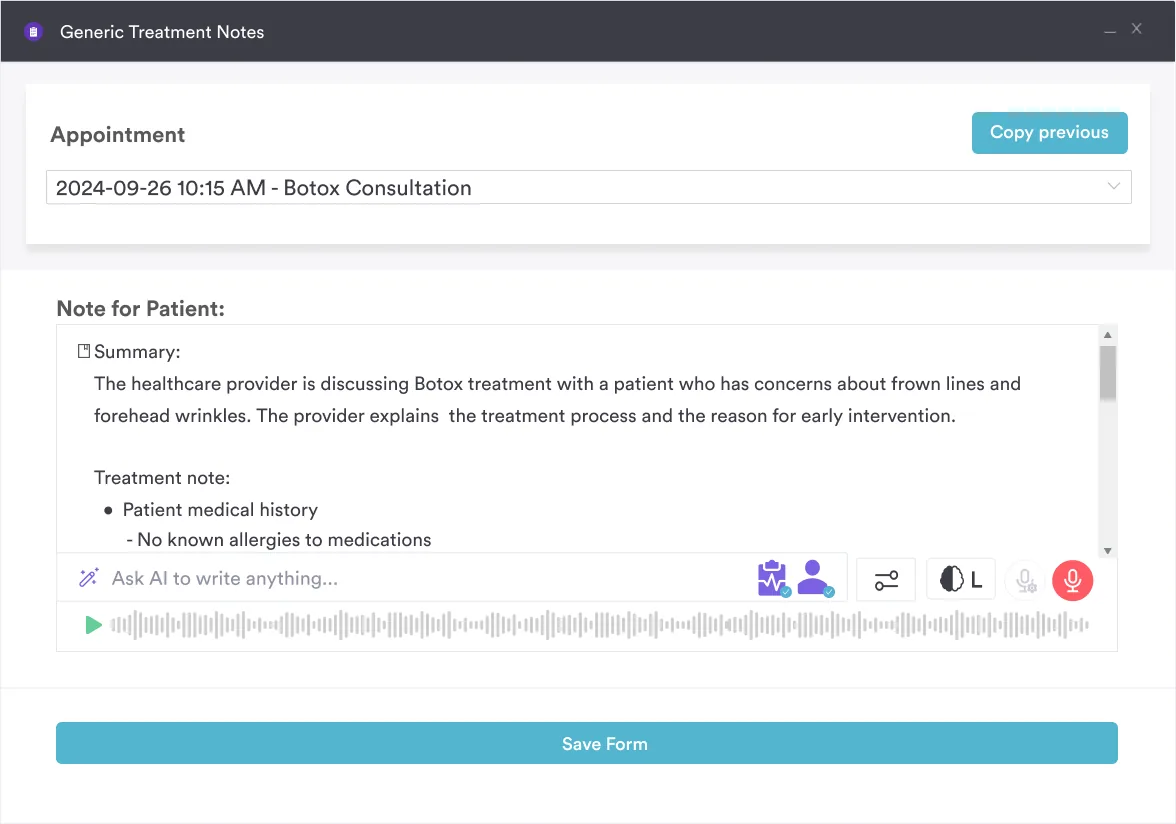
Practice management systems that support structured ENT note templates can automatically surface fields for air-bone gap measurements, bone-conduction thresholds, and laterality confirmation. This reduces the documentation query cycle, which in high-volume audiology practices can add days to the billing lag. Pabau Scribe, our AI scribe, helps practitioners generate structured clinical notes that capture the specific diagnostic detail needed to support codes like H90.6, so coders rarely have to go back to providers for clarification.
For practices managing pediatric bilateral mixed hearing loss, documentation requirements have an additional dimension. Pediatric patients undergoing cochlear implant evaluation, hearing aid fitting, or early intervention assessments will have H90.6 as a recurring diagnosis across multiple encounters. Maintaining a consistent, longitudinal patient management record that carries forward audiometric data across visits supports both continuity of care and coding consistency.
Multi-location ENT groups face a compounding challenge: ensuring that every site uses the same documentation template so that coders apply H90.6 consistently regardless of which clinician or location performed the evaluation. A compliance management system with standardized form templates across locations closes this gap and reduces inter-site coding variation — a discipline that extends across the wider H-chapter in combined eye-and-ear groups that also code conditions such as unspecified keratitis. For practices looking at broader EHR integration strategies, consistent ICD-10 code usage across connected systems also matters for population health reporting and payer analytics.
ICD-10 Code H90.6 is the correct, billable code when both ears present with a combination of conductive and sensorineural hearing loss, but the claim succeeds only when documentation confirms all three required elements: bilateral presentation, conductive component, and sensorineural component. Choosing H90.8 when H90.6 is supported is under-coding; choosing H90.6 without bilateral documentation is unsupported coding.
Audiology and ENT practices that build structured documentation workflows, use templates that prompt laterality and dual-component confirmation, and link diagnosis codes to procedure codes at the point of entry will consistently file cleaner claims. Pabau’s digital forms and claims management tools are built for exactly this kind of structured, compliance-ready documentation. To see how Pabau supports ENT and audiology billing workflows, book a demo with the team.
Need a reference for other ICD-10 diagnostic codes? Situational anxiety ICD-10 code guide covers documentation and coding workflows for anxiety diagnoses in clinical practice.
Looking for ENT and audiology practice management tools? Practice management software for clinics explains what to look for in a system that supports ENT billing and documentation compliance.
Want to reduce claim denials across your specialty? ADHD screening CPT code reference demonstrates how structured procedure and diagnosis code pairings reduce submission errors across specialty practices.
There is no single code for every bilateral hearing loss; the code follows the type of loss documented in both ears. Bilateral conductive loss is H90.0, bilateral sensorineural loss is H90.3, and mixed conductive and sensorineural loss in both ears is H90.6. Choose the option the audiogram and clinician note support, since payers expect the most specific code the record allows.
The code depends on laterality. For mixed conductive and sensorineural loss in both ears, use H90.6. For loss in one ear with normal hearing on the other, use the H90.7 sub-codes. When the record does not state which ears are affected, H90.8 is the unspecified option. Documenting laterality is what moves the claim from the unspecified code to the specific one.
ICD-10 Code H90.6 is the diagnosis code for mixed conductive and sensorineural hearing loss affecting both ears simultaneously. It means the patient has both a mechanical hearing loss component (affecting the outer or middle ear) and a nerve-related hearing loss component (affecting the inner ear or auditory nerve), and this dual pattern is present in both ears.
Yes. H90.6 is a fully billable and specific ICD-10-CM code valid for 2026. It can be used on insurance claims to indicate the diagnosis for reimbursement purposes when the clinical documentation supports bilateral mixed conductive and sensorineural hearing loss.
H90.6 specifies bilateral mixed hearing loss; H90.8 is used when the laterality of the mixed loss is unspecified. Use H90.6 when the clinical note confirms both ears are affected. Use H90.8 only when the documentation genuinely does not specify whether the mixed loss is bilateral or unilateral. Defaulting to H90.8 when H90.6 is supported constitutes under-coding.
H90.3 describes bilateral conductive hearing loss only, with no sensorineural component. H90.5 describes unspecified sensorineural hearing loss, with no conductive component documented. H90.6 applies specifically when both components are confirmed in both ears. Selecting H90.3 or H90.5 when mixed loss is documented is a specificity error that payers may flag on audit.
The most common CPT pairings are 92557 (comprehensive audiometry, bilateral), 92553 (pure tone audiometry, air and bone), 92567 (tympanometry), and 92587 (otoacoustic emissions). For cochlear implant candidacy, 92626 is used alongside H90.6 to document the evaluation. Each CPT code should be supported by its own documentation beyond the H90.6 diagnosis.
The clinical record must explicitly state bilateral hearing loss, confirm the conductive component through air-bone gap or middle-ear pathology documentation, and confirm the sensorineural component through elevated bone-conduction thresholds. Audiogram results should be attached or referenced in the note. Missing any of these three elements risks downcoding to H90.8 or claim denial.