ICD-10 code S52.131R: Displaced fracture of neck of right radius
ICD-10 code S52.131R is a billable diagnosis code for a displaced fracture of th...
Last Updated: August 5, 2026
ICD-10 Code H42 is a billable diagnosis code for glaucoma that arises as a manifestation of a systemic disease classified elsewhere in ICD-10-CM.
H42 requires a Code First instruction: the underlying condition (such as amyloidosis E85.-, aniridia Q13.1, or Lowe’s syndrome E72.03) must be sequenced as the principal diagnosis.
H42 does not use laterality or staging sub-codes, unlike the H40.x range; congenital glaucoma (Q15.0) and absolute glaucoma (H44.51) are excluded.
Pabau’s claims management software supports accurate diagnosis code sequencing and ophthalmology documentation workflows.
ICD-10 Code H42 (Glaucoma in diseases classified elsewhere) is a billable diagnosis code for glaucoma occurring as a manifestation of a systemic disease coded elsewhere in ICD-10-CM. Unlike the H40.x range, it carries a Code First instruction, so the underlying systemic condition must be sequenced ahead of H42 on every claim.
ICD-10 Code H42 applies only when glaucoma is a direct manifestation of a systemic disease that is coded elsewhere in ICD-10-CM. It is not a code for primary glaucoma, and it is not interchangeable with the H40.x range that covers most glaucoma claims.
H42 sits within ICD-10-CM Chapter 7 (Diseases of the eye and adnexa, H00-H59), block H40-H42 (Glaucoma). Per the WHO ICD-10 classification browser, the code’s full descriptor is “Glaucoma in diseases classified elsewhere.” It covers secondary glaucoma presentations driven by metabolic, congenital structural, or systemic disease processes, where the root cause receives its own ICD-10 code in a separate chapter.
Ophthalmologists and optometrists using dermatology EMR software or ophthalmic practice management systems encounter this code when managing patients whose elevated intraocular pressure stems from an underlying systemic condition rather than primary glaucoma. The distinction matters for claim submission: payers expect a correctly sequenced code pair, not H42 listed in isolation.
H42 is a billable and specific ICD-10-CM diagnosis code. It is valid for reimbursement purposes for the 2026 fiscal year, as confirmed by the CDC/NCHS ICD-10-CM web tool.
Its position in the code hierarchy is:
Unlike most H40.x codes, H42 has no sub-codes. There are no laterality extensions (no right eye, left eye, or bilateral variants) and no staging sub-codes. The American Academy of Ophthalmology ICD-10 Glaucoma Reference Guide explicitly notes “No eye indicators” and “Staging codes not required” for H42. This simplifies code selection. However, laterality and severity should still be recorded in the note, even though the code itself does not capture them.
The Code First instruction is the most critical rule governing H42. Under the etiology-manifestation coding convention in ICD-10-CM, certain conditions require two codes: one for the underlying disease and one for the body-system manifestation. H42 is always the manifestation code. Never list it first.
The CMS ICD-10-CM Official Guidelines, accessible through the CMS ICD-10 codes page, define this convention clearly. When a condition such as amyloidosis causes glaucoma, amyloidosis is the principal diagnosis and H42 follows as the secondary diagnosis. Reversing that order is a sequencing error and a common cause of claim denial. Understanding this principle applies beyond ophthalmology, for example in etiology-manifestation coding for neurological conditions where the same two-code convention applies.
The officially recognized underlying conditions that trigger H42 are:
Only conditions listed in this group justify H42. Documenting a systemic condition not found within this set (such as diabetic retinopathy or hypertension-related eye changes) does not trigger H42. Those presentations use different code paths in the H40.x range or disease-specific codes.
Review the sequencing before every H42 submission. If the underlying condition code (E85.-, Q13.1, E72.03, Q13.81, or E70-E88) does not appear as the first-listed diagnosis on the claim, the payer will almost certainly deny it. Build a coding checklist into your EHR template to catch sequencing errors at the point of documentation.
The H40.x range covers primary, secondary, and unspecified glaucomas (H40.9) with laterality and staging sub-codes. H42 covers one specific scenario: the patient has a systemic disease from the approved underlying-condition list and glaucoma is a recognized manifestation of that disease.
Common selection mistakes include using H42 for steroid-induced glaucoma (H40.6-, glaucoma secondary to drugs), pigmentary glaucoma (H40.13-), or pseudoexfoliation glaucoma (H40.14-). Each of these is a form of secondary glaucoma with its own H40 sub-code that carries laterality and staging, which H42 does not. H42 also does not apply to traumatic glaucoma due to birth injury (P15.3) or congenital glaucoma (Q15.0), both of which are Type 1 Excludes for the H40-H42 block.
For practices managing complex comorbidity profiles, the AAPC Codify ICD-10-CM lookup provides crosswalks and clinical criteria that can help clarify which H40 sub-code applies when H42 is ruled out. Similar attention to diagnostic specificity is needed when coding related systemic manifestations, such as in ICD-10 coding for autism spectrum disorder, where the etiology-manifestation convention also influences sequencing decisions.
Type 1 Excludes codes are conditions that cannot be coded alongside H42 under any circumstance. The H40-H42 block carries the following Type 1 Excludes:
If any of these is the clinical diagnosis, do not use H42. These are distinct conditions with their own dedicated codes.
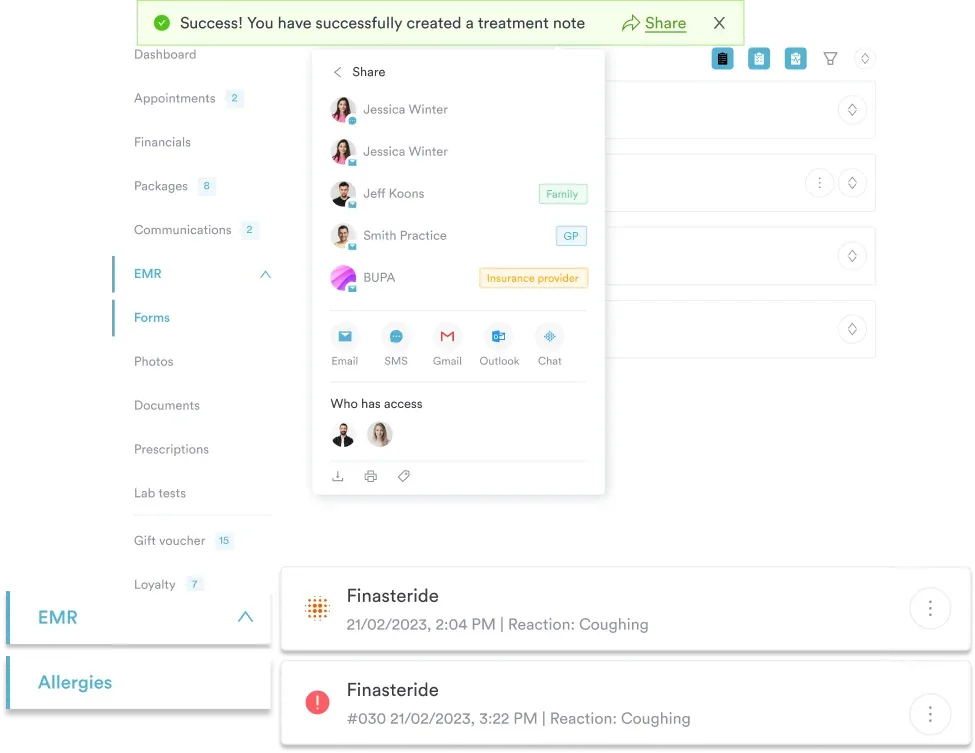
Pabau's claims management software helps ophthalmic and specialist practices submit accurate diagnosis code pairs, reduce sequencing errors, and manage complex comorbidity documentation from one platform.

Payers auditing H42 claims look for three things in the clinical note: a confirmed diagnosis of the underlying systemic condition, a documented causal link between that condition and the glaucoma, and evidence of ophthalmic evaluation including IOP measurement and visual field or optic nerve assessment.
Generic documentation such as “glaucoma in a patient with amyloidosis” may not satisfy payer requirements. The note should explicitly state that the glaucoma is caused by the systemic condition. If ophthalmology and a referring internist or metabolic specialist are both involved, reference the treating specialist’s evaluation too. Medical forms for healthcare practices that capture systemic history at intake make this documentation far easier to build into the clinical note.
Practices using clinical documentation tools with structured note templates can configure fields that prompt clinicians to record the causal relationship explicitly. This reduces the chance of a claim going out with a weak narrative that fails a payer’s medical necessity review. Practices that also use digital intake forms can capture systemic disease history from patients before the encounter, giving clinicians pre-populated data to reference in the note.
Maintaining HIPAA-compliant clinical documentation standards is particularly important when sharing notes across referring specialists who contribute to the diagnostic picture for H42 cases.
Flag H42 cases for a pre-submission coding review whenever a new underlying condition is identified. If the underlying condition has changed or been refined (e.g., a metabolic disorder sub-classified more specifically), the paired E-code will change too. Catching that mismatch before claim submission costs far less than managing a denial and resubmission cycle.
Claim denials for H42 almost always trace back to three errors. These are: sequencing the manifestation code first, using H42 for a glaucoma type with its own H40 sub-code, or omitting the underlying condition code entirely. Building a structured workflow around these three failure points prevents most rejections.
Practices using claims management software that supports diagnosis code pairing validation can catch sequencing errors automatically at the point of claim generation. This is particularly useful in multi-provider ophthalmology settings where different clinicians may document the systemic condition and the ocular manifestation in separate encounters.
Integrating ophthalmic coding workflows with the broader EHR environment also reduces transcription risk. EHR integration for ophthalmology practices ensures that systemic diagnoses recorded by referring physicians flow through to the ophthalmology encounter note, supporting accurate code selection without manual re-entry.
For practices evaluating their current coding accuracy, reviewing historical H42 claims against the Code First requirement is a practical audit starting point. Review any H42 claim submitted without a paired E-code in the principal position for potential corrected claim submission. Tracking denial patterns by ICD-10 code through structured diagnostic coding records helps identify systemic coding errors that may affect reimbursement across multiple code types, not just H42.
ICD-10 Code H42 is a billable code, but it never stands alone. Every valid H42 submission pairs it with an underlying condition code sequenced first, reflecting the etiology-manifestation convention that defines how ICD-10-CM handles secondary disease manifestations. Getting that sequencing right is the difference between a clean claim and a denial.
Pabau’s claims management software supports practices in building diagnosis code pairing rules and structured documentation workflows, reducing the sequencing and documentation errors that drive H42 denials. To see how Pabau handles ophthalmology coding and billing workflows, explore features that save private practices time or book a demo.
ICD-10 Code H42 is a billable ICD-10-CM diagnosis code for glaucoma that occurs as a manifestation of a systemic disease classified elsewhere in the code set, requiring the underlying condition to be sequenced first on any claim.
Yes, but it cannot be submitted in isolation — the underlying systemic condition must appear as the principal diagnosis on the claim.
H40.x covers primary and most secondary glaucoma types with laterality and staging sub-codes; H42 applies only when glaucoma is a manifestation of a specific systemic disease coded elsewhere, and has no laterality or staging variants.
Amyloidosis (E85.-), aniridia (Q13.1), Lowe’s syndrome (E72.03), Rieger’s anomaly (Q13.81), and specified metabolic disorders (E70-E88). Other systemic conditions causing glaucoma use different H40 sub-codes.
If the cause is a systemic disease from the H42 approved list, sequence the underlying condition code first and H42 second; for other causes such as steroid use or pseudoexfoliation, use the appropriate H40.x sub-code with laterality and staging.
Steroid-induced glaucoma is not reported with H42. It is a drug-induced secondary glaucoma coded in the H40.6- range (glaucoma secondary to drugs), with a laterality and staging sub-code selected from the clinical note.
Code First is the etiology-manifestation convention requiring the underlying disease to be listed as the principal diagnosis before the manifestation code — for H42, the systemic condition is always sequenced ahead of H42 on the claim.