ICD-10 Code M32.9: Systemic lupus erythematosus, unspecified
M32.9 codes SLE when the notes name no organ involvement. Treat it as the fallba...
Last Updated: August 3, 2026
ICD-10 Code C19 is the billable 2026 ICD-10-CM diagnosis code for malignant neoplasm of rectosigmoid junction, the anatomical zone where the sigmoid colon meets the rectum.
C19 is valid only when pathology spans or originates at the rectosigmoid junction; tumors confined to the rectum use C20, and sigmoid colon primaries use C18.7.
C19 converts directly to ICD-9-CM 154.0 and groups to MS-DRG 374, 375, or 376 (Digestive Malignancy) under the FY2026 MS-DRG grouper (v43.0) for Medicare reimbursement purposes.
Accurate documentation of tumor location is the most common coding failure point; practice management software like Pabau, including its clinical documentation and patient records tools, helps oncology practices maintain precise, audit-ready records.
Rectosigmoid junction tumors sit at one of the most debated anatomical boundaries in colorectal cancer coding. Get the location wrong in the clinical note, and a clean claim becomes a denial. ICD-10 Code C19 covers this specific junction. It applies only when the tumor genuinely involves the transition zone between the sigmoid colon and rectum. Coders in gastroenterology and oncology practices regularly face scrutiny over C19 versus C20 versus C18.7. Payers follow the documentation closely.
ICD-10 code C19 is the billable diagnosis code for malignant neoplasm of the rectosigmoid junction, the zone where the sigmoid colon meets the rectum. This C19 ICD-10 reference covers its 2026 ICD-10-CM status, clinical scope, applicable synonyms, MS-DRG grouping, adjacent code distinctions, documentation requirements, and the ICD-9-CM crosswalk. The sections below address the specifics coders get wrong most often. It is useful whether you’re preparing a claim, auditing a chart, or training a coding team.
ICD-10 Code C19 designates a malignant neoplasm of the rectosigmoid junction. The WHO ICD-10 classification places this code within Chapter II (Neoplasms, C00-D49), subrange C15-C26. For 2026, C19 remains an active, fully billable ICD-10-CM diagnosis code. No revisions were made to its descriptor or hierarchical placement.
The rectosigmoid junction is not simply a named location on a diagram. It is the functional transition zone where the sigmoid colon narrows into the rectum. This sits roughly 15 to 20 centimeters from the anal verge. Tumors that originate at or span this zone are assigned C19. Tumors confirmed to lie entirely within the rectum take C20. The distinction matters because payers use it to validate procedure codes, staging, and surgical claims. Oncology practices using claims management software with structured diagnosis fields reduce location-coding errors at the point of chart entry.
ICD-10 Code C19 carries official “Applicable To” notes that define which clinical terms map to this code. These synonyms are not informal alternatives. They are documented inclusions recognized by the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). Both bodies include them in the ICD-10-CM Tabular List.
When the pathology report uses “carcinoma of rectosigmoid” without further subtyping, C19 remains correct — provided the location is documented as the junction. Never assign C19 based solely on proximity. The clinical or pathology note must confirm junction involvement.
The three-way distinction between C19, C20, and C18.7 is the most frequent coding error in colorectal oncology billing. Each code corresponds to a distinct anatomical zone. Payers audit them against operative reports, colonoscopy findings, and pathology results. Misassignment can trigger medical necessity denials and post-payment audits. The CDC/NCHS ICD-10-CM web tool provides the official 2026 tabular list for verifying these boundaries.
ICD-10-CM lists a Type 1 Excludes note under C18.7 that points to C19, confirming the two codes are mutually exclusive and should never be reported together for the same lesion. If pathology confirms a sigmoid colon primary, C18.7 applies regardless of proximity to the junction.
C19 carries its own Type 1 Excludes note, for malignant carcinoid tumors of the colon, which are reported separately under C7A.02-. When documentation is genuinely ambiguous, query the treating physician before assigning a code. Assumptions based on anatomy alone do not meet official guidelines.
For practices managing patients with colorectal malignancies, accurate code differentiation also affects quality reporting. Structured diagnostic code documentation habits built into clinical workflows reduce boundary errors between C19 and adjacent codes. They catch issues at the note-writing stage, before a coder ever sees the chart.
When the operative or endoscopy report describes a tumor as ‘at the junction of sigmoid and rectum’ or ‘involving the rectosigmoid,’ C19 is appropriate. When the report says ‘distal sigmoid’ without mentioning the junction, query the physician before coding.
Under the FY2026 MS-DRG grouper (v43.0), C19 as the principal diagnosis groups to MS-DRG 374, 375, or 376 (Digestive Malignancy with MCC, with CC, or without CC/MCC) under MDC 06. MS-DRG groupings determine the base payment rate for inpatient hospital claims.
Service dates must fall on or after October 1 of the applicable fiscal year. The specific DRG within that family depends on whether coded diagnoses include a major complication or comorbidity (MCC) or complication or comorbidity (CC).
For outpatient billing, C19 appears on claims for colonoscopy encounters, staging workups, chemotherapy visits, and surgical pre-authorization requests. Each claim type requires accurate diagnosis-to-procedure pairing. The CMS ICD-10 codes page publishes current code files and grouper logic. Practices can also consult the AAPC Codify ICD-10-CM lookup for crosswalk and grouper reference.
Avoid citing specific dollar reimbursement amounts by MS-DRG. Payment weights shift annually with the Inpatient Prospective Payment System (IPPS) final rule. Site-neutral adjustments also affect many facilities. Reference the MS-DRG grouping for claim routing only — not as a proxy for expected payment. For practices building reimbursement reporting workflows, structured reporting tools that track case mix alongside MS-DRG assignment give a fuller picture of payment variability across a caseload.
Pabau helps oncology and specialty practices capture structured diagnosis data, link procedures to the right ICD-10 codes, and keep audit-ready records. See how it works for your team.

According to the CMS and NCHS Official ICD-10-CM Guidelines, C19 is a primary site code. Assign it when the rectosigmoid junction is the confirmed origin of the malignancy. Do not assign C19 for metastatic disease spreading to the junction from another primary. Those encounters require both the primary site code and the appropriate secondary malignant neoplasm code from the C78 or C79 series.
C19 applies only to primary tumors. When a patient has a known primary elsewhere — for example, C10.1 — and presents with junction involvement, assign the original primary code plus the applicable C78 secondary code. Conflating primary and secondary coding is a high-risk audit area for oncology practices. The distinction affects both clinical communication and payer processing.
C19 may require additional codes to reflect the full clinical picture. Common codes alongside C19 include Z-codes for chemotherapy status, personal history of malignancy, or follow-up encounters. When a patient is receiving chemotherapy or radiation, list the appropriate encounter code as the reason for the visit. Use Z51.11 for antineoplastic chemotherapy and Z51.12 for antineoplastic immunotherapy. C19 is then added as a secondary code to identify the primary malignancy.
Practices with high volumes of oncology follow-up visits benefit from practice management software features that let coders attach recurring secondary codes to patient profiles. This reduces the risk of omitting required Z-codes on submissions. For clinical documentation and patient records to support accurate coding, the note must state whether the encounter is for active treatment, follow-up, or surveillance.
The treating clinician must document tumor location with enough specificity to support C19. Acceptable terms include “rectosigmoid junction,” “rectosigmoid (colon),” or “colon with rectum.” Vague entries such as “colorectal cancer” or “lower GI malignancy” do not support C19. Coders should not infer junction involvement from imaging or diagrams alone. A corresponding clinical statement is required.
For coding teams in gastroenterology or oncology, a documentation checklist helps. Prompting physicians to specify tumor location at endoscopy or surgical note completion reduces query turnaround time. Patient care management workflows that integrate note templates into appointment workflows provide measurable efficiency gains.
Build a physician query template for colorectal cases that asks: ‘Is the tumor located at the rectosigmoid junction, within the rectum, or within the sigmoid colon?’ A single clarifying question at note completion prevents downstream coding errors and payer denials.
Understanding how C19 relates to adjacent codes helps coders navigate complex colorectal cancer encounters. This is especially useful for patients with overlapping or multi-site disease. The following codes are directly relevant to C19 coding decisions.
ICD-10 Code C19 converts directly to ICD-9-CM 154.0 via the CMS General Equivalence Mappings (GEMs). This is a one-to-one forward and backward mapping with no ambiguity. Practices reviewing historical claims or handling audits spanning the ICD-9 transition can use this crosswalk with confidence. For a free lookup, the ICD List platform supports bidirectional crosswalk searches. Note that HIPAA compliance for medical offices governs how historical diagnostic data is retained and transmitted across system migrations.
Coding accuracy for rectosigmoid junction malignancies depends on the clinical note, not the coder. When physicians use structured templates that prompt for tumor location, downstream coding becomes straightforward. The challenge is building that habit into routine documentation. Relying on coders to query every colorectal case is not sustainable.
Gastroenterology and oncology practices see measurable improvements when documentation tools prompt clinicians to specify anatomical boundaries at the time of the procedure note. Digital intake and assessment forms with structured fields for tumor location, histology, and staging give coders the data they need. This removes the need for retrospective querying and supports CMS and NCHS specificity requirements.
For multi-location oncology practices, standardized templates reduce note quality variability across sites. When one site uses “colorectal tumor” and another documents “malignant neoplasm of rectosigmoid junction,” coding outcomes diverge — even for identical clinical presentations. Consistent templates solve this at the source.
The same discipline pays off upstream, too. Primary care practices ordering the initial referral colonoscopy, and wellness clinics tracking screening due-dates, see similar gains from structured note fields. For practices evaluating structured documentation tools, this same approach provides useful context on aligning clinical and administrative data flows.
The single biggest coding risk with C19 is location ambiguity in the clinical note. When the physician documents the rectosigmoid junction precisely, code selection is clear and claims process without friction. When the note is vague, coders must choose between querying — which delays the claim — or guessing, which creates audit exposure. That same trade-off shows up in far different diagnosis categories, from A64 to G09, wherever ICD-10 rewards precise clinical detail over shorthand.
Pabau’s clinical documentation tools help oncology and specialty practices build structured note templates. These capture anatomical specificity at the point of care — not during retrospective coding. To reduce ICD-10 coding errors and improve documentation quality, book a demo to see how Pabau supports oncology practice management.
Comparing C19 with a confirmed rectal-only diagnosis? C20 is the code to use when there is no documented junction involvement.
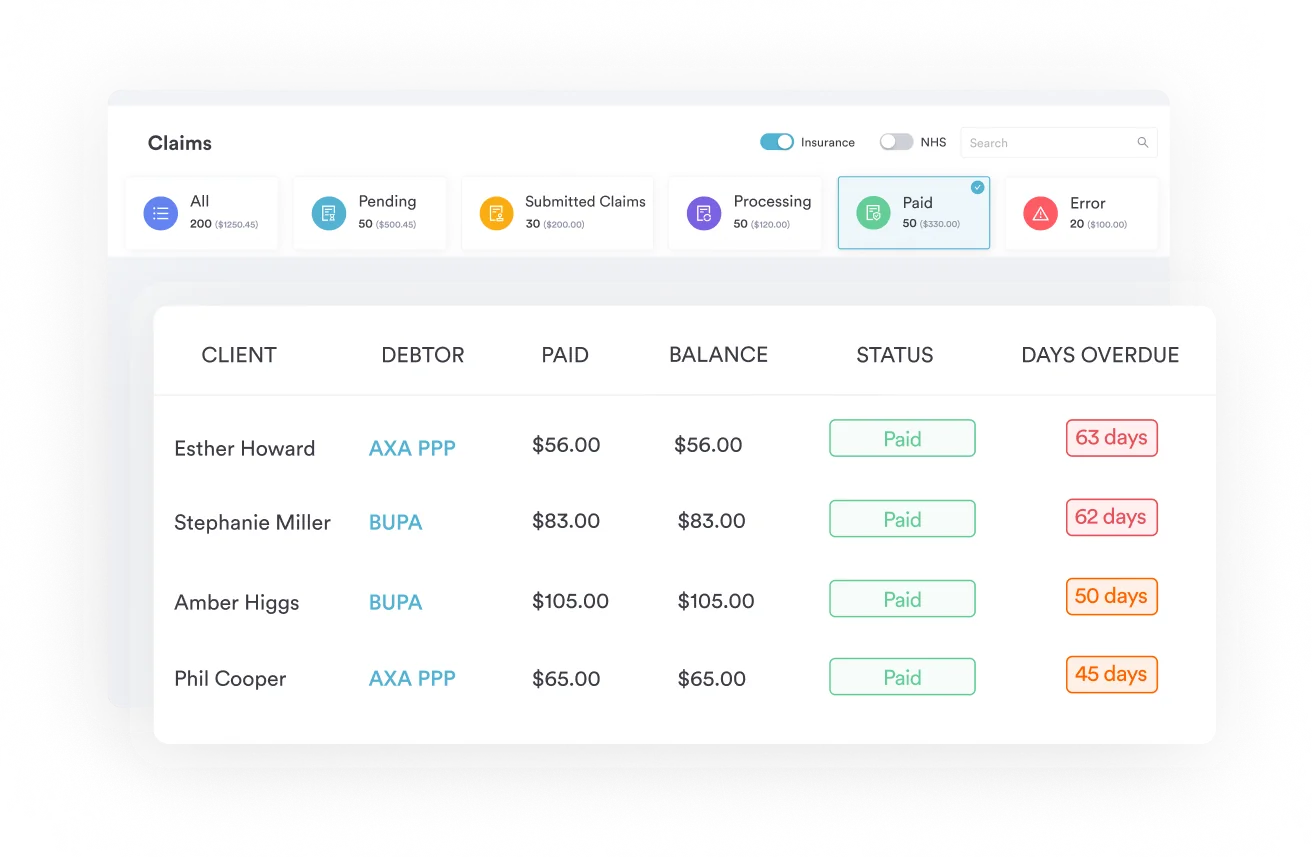
Managing claims accuracy across a specialty practice? Pabau’s claims management software links diagnosis codes to procedures and flags common pairing errors before submission.
Looking to improve overall practice management for oncology workflows? Oncology practice management explores how structured clinical and administrative data flows reduce operational errors.
ICD-10 Code C19 is the 2026 ICD-10-CM diagnosis code for malignant neoplasm of rectosigmoid junction, the anatomical zone where the sigmoid colon meets the rectum. It is a billable primary site code classified under Chapter II (Neoplasms, C00-D49) in the WHO and CMS classification systems.
C19 is used when the malignant tumor originates at or spans the rectosigmoid junction; C20 is used when the tumor is confined entirely to the rectum with no junction involvement documented. The clinical or pathology note must specify which location applies: coders cannot infer junction involvement from proximity alone.
Yes. C19 is an active, fully billable ICD-10-CM diagnosis code for fiscal year 2026. No descriptor changes or code revisions were made to C19 in the 2026 update cycle, and it remains valid for claims with a date of service on or after October 1, 2025.
C19 groups to MS-DRG 374, 375, or 376 (Digestive Malignancy with MCC, with CC, or without CC/MCC) under the FY2026 MS-DRG grouper (v43.0). The specific DRG assignment within that family depends on whether the claim includes diagnoses that qualify as a major complication or comorbidity (MCC) or complication or comorbidity (CC), which affects the payment weight applied to the inpatient episode.
ICD-10 Code C19 converts directly to ICD-9-CM 154.0 (Malignant neoplasm of rectosigmoid junction) via the CMS General Equivalence Mappings. This is a one-to-one forward and backward crosswalk with no ambiguity.
The official Applicable To notes for C19 include: adenocarcinoma of rectosigmoid junction, malignant neoplasm of colon with rectum, and malignant neoplasm of rectosigmoid (colon). Lymphoma and sarcoma at the junction site are also covered under C19 when the rectosigmoid junction is the confirmed primary location.
No. C19 is a complete three-character ICD-10-CM code with no decimal subdivisions, so C19.9 does not exist. Unlike C18, which splits into C18.0 through C18.9 by colon subsite, the rectosigmoid junction is coded with C19 on its own.