Lateral pivot shift test: How to perform, grade, and interpret
A positive lateral pivot shift test is 97-98% specific for ACL deficiency, but a...
Last Updated: August 5, 2026
Cozen’s test is a resisted wrist extension test used to assess lateral epicondylitis (tennis elbow) by reproducing familiar lateral elbow pain.
Proper patient positioning (shoulder neutral, elbow flexed to 90°, forearm pronated, wrist neutral) is critical for test accuracy and reproducibility.
A positive result indicates reproduction of lateral elbow pain during resisted wrist extension. Cozen’s test cannot detect intrasubstance degenerative tendon changes.
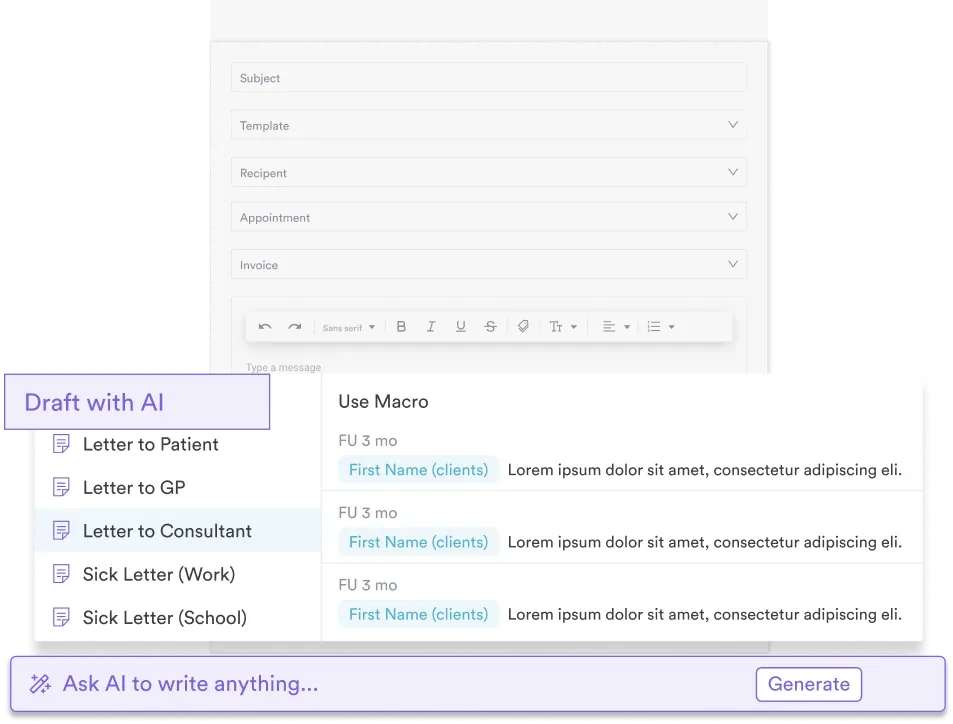
Digital assessment forms in practice management software like Pabau streamline test recording and enable automated follow-up workflows.
A ready-to-use assessment form covering patient details, positioning criteria, test procedure steps, pain reproduction criteria, clinical interpretation, and documentation fields for recording a positive or negative Cozen’s test result.
Download templatePhysiotherapists and musculoskeletal clinicians performing Cozen’s test rely on consistent patient positioning and standardized assessment criteria to reliably identify lateral epicondylitis, commonly known as tennis elbow. This downloadable form helps practitioners document findings systematically, ensuring consistent clinical decision-making and comprehensive patient records. Whether you’re screening for lateral elbow tendinopathy or establishing baseline function before treatment planning, a structured digital assessment form reduces documentation time and improves data capture accuracy.
Cozen’s test, also known as the resisted wrist extension test or resistive tennis elbow test, is a physical examination maneuver used to assess for lateral epicondylitis and related extensor tendon irritation. The test loads the extensor carpi radialis brevis (ECRB) and surrounding wrist extensor muscles at their origin point on the lateral epicondyle of the humerus. A positive result raises clinical suspicion for lateral epicondylalgia. It shows up as reproduction of the patient’s familiar lateral elbow pain during resisted wrist extension.
Cozen’s test stands out among orthopedic special tests because it is quick to perform, requires minimal equipment, and delivers reliable clinical findings when combined with patient history and palpation findings. Research confirms that Cozen’s test and grip strength measurement present high accuracy in the diagnosis of lateral elbow tendinopathy, though the condition typically requires imaging confirmation for definitive diagnosis.
However, Cozen’s test cannot detect degenerative tendon changes such as intrasubstance tears. The test identifies pain reproduction, not structural pathology. Ultrasound imaging (USI) or MRI may be necessary when advanced tendon assessment is needed or when clinical presentation suggests intrasubstance pathology.
Performing Cozen’s test accurately requires systematic patient positioning and careful application of resisted wrist extension. The following five steps outline the standard Cozen’s test procedure used by physiotherapists and sports medicine practitioners worldwide.
Consistency across repetitions is essential. If you perform Cozen’s test twice during a single session, pain reproduction should be similar. Marked variability may suggest non-organic findings or central sensitization factors worth exploring through additional history and examination.
Cozen’s test is invaluable across multiple healthcare disciplines. Physiotherapists specializing in musculoskeletal conditions use it daily to screen for lateral epicondylitis in patients presenting with lateral elbow pain. Sports medicine practitioners apply it to assess athletes returning to racquet sports, throwing activities, or repetitive gripping tasks. Occupational therapists use Cozen’s test to establish baseline function in patients with work-related lateral elbow tendinopathy.
Chiropractic and osteopathic practitioners also rely on Cozen’s test as part of comprehensive elbow assessment protocols. General practitioners and nurse practitioners in primary care settings use it to differentiate lateral epicondylitis from other causes of lateral elbow pain before considering imaging or referral to specialist services.
Standardized documentation ensures consistent, comparable findings across multiple assessment visits. When practitioners record test results using the same form structure, benchmarking treatment outcomes becomes straightforward. Has pain reproduction intensity decreased? Has the pain location shifted? Does the familiar pain quality stay consistent?
A downloadable template also supports clinical documentation efficiency. Instead of writing narrative descriptions of test findings, clinicians tick positioning boxes, note pain intensity using a numeric scale, and record whether pain matched the patient’s familiar complaint. This structured format reduces documentation time and improves data quality for audit and research purposes.
Additionally, a formal assessment template creates a paper trail for medicolegal protection. Should a patient question the thoroughness of your assessment, a completed Cozen’s test form demonstrates that you systematically evaluated lateral epicondylitis as part of your differential diagnosis process.
Practice management software like Pabau keeps these forms inside one clinical system. Book a demo to see how customizable assessment forms streamline your workflow, trigger automated patient follow-ups, and centralize clinical records for your whole team.
Physiotherapy clinics must meet HCPC and CSP professional standards for clinical documentation. Structured assessment forms demonstrate compliance with these standards by showing systematic evaluation of presenting complaints using validated orthopedic special tests. Documentation completeness is also critical for HIPAA compliance in US-based practices and GDPR compliance in UK and EU settings.
Three special tests dominate lateral epicondylitis assessment: Cozen’s test, Mill’s test, and Maudsley’s test. All three reproduce pain at the lateral epicondyle, but they differ in wrist position and the specific tendon loading pattern.
| Test | Wrist position | Mechanism | Clinical use |
|---|---|---|---|
| Cozen’s test | Neutral flexion-extension, extended | Resisted wrist extension loads ECRB | Most common; high reproducibility across clinicians |
| Mill’s test | Flexion, pronated | Passive wrist flexion stretches extensor origin | Passive alternative; useful if patient guarding prevents active testing |
| Maudsley’s test | Neutral, middle finger extended | Resisted extension of middle finger isolates ECRB | Discriminates ECRB from other extensors; less commonly used in routine practice |
For routine clinical practice, Cozen’s test remains the first choice because it is quick, reproducible, and familiar to most clinicians. Efficient screening of multiple patients benefits from using the test that delivers reliable information in 30 seconds rather than 2 minutes.
Clinicians often want exact sensitivity and specificity values for Cozen’s test, but the diagnostic accuracy studies are limited and vary in method. A systematic review in the Journal of Hand Therapy reported high sensitivity for Cozen’s test (around 91%) while noting that its specificity is poorly investigated. A negative result therefore helps lower the likelihood of lateral epicondylitis, but a positive result needs corroboration before you act on it.
Treat a positive Cozen’s test as a strong screening signal rather than a standalone diagnosis. No orthopedic special test confirms lateral epicondylitis on its own, so pair it with point tenderness on palpation of the lateral epicondyle, grip strength testing, and Mill’s or Maudsley’s test to raise diagnostic confidence. When the clinical picture stays unclear, ultrasound or MRI confirms the structural tendon changes this test cannot detect.
When recording Cozen’s test findings, clarity and specificity are essential. Rather than writing “Cozen’s test positive,” document the exact pain reproduction pattern: pain location, whether it matched the patient’s familiar complaint, pain intensity on a numeric scale (0-10), and any patient comments about the quality or onset of pain.
A sample SOAP note entry might read: “Cozen’s test performed with shoulder neutral, elbow 90° flexion, forearm pronation. Resisted wrist extension reproduced familiar lateral elbow pain at epicondyle region, intensity 6/10, onset immediate, quality sharp-aching consistent with patient’s chief complaint. Right forearm slightly more tender than left on palpation of lateral epicondyle.”
This level of detail supports clinical decision-making, enables outcome tracking across visits, and provides evidence for comprehensive patient management. When combined with grip strength testing, palpation findings, and patient history, documented Cozen’s test results form the foundation of a defensible clinical diagnosis.
While Cozen’s test is reliable for identifying pain reproduction, it has important limitations. The test cannot identify intrasubstance tendon tears, calcification, or early degenerative changes. If a patient presents with severe functional limitation, chronicity beyond three months without improvement, or a history of sudden onset suggesting acute rupture, integrated clinic management systems should flag a referral pathway for ultrasound or MRI imaging.
Additionally, Cozen’s test may yield false positives in patients with central sensitization, fibromyalgia, or global hyperalgesia. A positive test should always be interpreted within the context of patient history, palpation findings, and functional limitations, not in isolation.
The reverse Cozen’s test applies the same methodology but assesses for medial epicondylitis (golfer’s elbow). Rather than resisted wrist extension, the clinician applies resisted wrist flexion or resisted pronation while the patient’s forearm is supinated, loading the flexor-pronator muscle group at its origin on the medial epicondyle. A positive reverse Cozen’s test reproduces familiar medial elbow pain. Documentation should clearly distinguish medial from lateral findings to avoid confusion during clinical handover or team-based clinic workflows.
Cozen’s test remains a first-choice orthopedic special test for lateral epicondylitis assessment because it is quick, reproducible, and immediately actionable in clinical practice. Consistent patient positioning, careful observation of pain reproduction, and detailed documentation enable clinicians to track functional changes and inform treatment planning decisions across multiple visits.
Using a downloadable assessment template standardizes your approach, reduces documentation time, and supports compliance with professional standards. See how Pabau’s clinical documentation system enables consistent, efficient Cozen’s test documentation across your entire physiotherapy team.
Need a standardized orthopedic assessment form? Physical therapy practice management software enables teams to create custom special test templates aligned with your clinic protocols.
Want to track patient outcomes over time? Patient care management systems centralize assessment results and automatically generate progress reports for clinician review.
Looking to improve clinical documentation speed? Digital client records with structured data-entry fields cut write-up time compared with narrative documentation.
A positive Cozen’s test indicates reproduction of familiar lateral elbow pain during resisted wrist extension with the forearm pronated and elbow at 90° flexion. Combined with point tenderness over the lateral epicondyle and a relevant clinical history, this finding raises clinical suspicion for lateral epicondylitis (tennis elbow).
Position the patient with shoulder neutral, elbow 90° flexion, forearm pronated, and wrist in neutral flexion-extension. Stabilize the forearm above the wrist, then ask the patient to extend the wrist against your manual resistance. Observe for reproduction of familiar lateral elbow pain.
Cozen’s test uses active resisted wrist extension to load the extensor tendons, while Mill’s test uses passive wrist flexion and pronation to stretch the extensor origin. Cozen’s test is more reproducible and commonly used; Mill’s test is a useful alternative when patient guarding prevents active testing.
No. Cozen’s test identifies pain reproduction but cannot detect intrasubstance degenerative changes, calcification, or tendon tears. Ultrasound imaging or MRI is required to visualize structural tendon pathology.
The reverse Cozen’s test applies resisted wrist flexion or pronation to assess for medial epicondylitis (golfer’s elbow). A positive result reproduces familiar medial elbow pain rather than lateral pain.
A negative Cozen’s test means resisted wrist extension did not reproduce the patient’s familiar lateral elbow pain. This lowers the likelihood of lateral epicondylitis but does not rule it out. Correlate the result with patient history, palpation, and grip strength before excluding the diagnosis.
Cozen’s test is pronounced “KOH-zenz.” The test is named after Dr. Lewis Cozen, the American orthopedic surgeon who first described the maneuver, which is why the possessive spelling (Cozen’s) is standard in clinical notes.