Personal trainer liability waiver: free template and what it covers
Download your free personal trainer liability waiver A two-part form covering as...
Last Updated: August 6, 2026
A biopsychosocial assessment is a structured clinical tool that evaluates biological, psychological, and social factors affecting a client’s mental health and wellbeing.
DCF-compliant assessments require documented risk assessment, diagnostic impression, strengths-based summary, and signatures from qualified clinicians.
Clinical social workers (LCSWs), licensed mental health counselors (LMHCs), and licensed psychologists can conduct biopsychosocial assessments depending on state scope of practice.
Pabau’s digital assessment forms support built-in compliance tracking, e-signatures, and secure storage to streamline DCF documentation workflows.
A ready-to-use clinical assessment form covering presenting problems, biological history (medical conditions and medications), psychological domain (mental health history and trauma), social context (family dynamics, housing, employment), risk assessment, strengths-based summary, and DSM-5-TR diagnostic impression.
Download templateA biopsychosocial assessment carries specific weight in child welfare and behavioral health cases. For example, a DCF caseworker or licensing reviewer looks for a completed risk screen, a diagnostic impression backed by a code, and a signature with the assessing clinician’s credentials attached.
Miss any of these, and as a result, a case review can stall or a licensing audit can flag the file as incomplete. Next, this guide walks through what belongs in each domain, who’s qualified to sign off, and the documentation habits that keep an assessment compliant from the first draft.
A biopsychosocial assessment template is a structured clinical documentation form used by mental health professionals to evaluate how biological, psychological, and social factors interact to affect a client’s mental health, emotional wellbeing, and overall functioning.
In addition, these assessments support broader clinical documentation practices, including SOAP notes, and are foundational for treatment planning in mental health, social work, and child welfare settings, especially in DCF-regulated programs.
The assessment captures presenting problems (reason for referral), medical history, medications, substance use, mental health diagnoses, cognitive functioning, trauma history, family dynamics, housing stability, employment status, cultural background, risk factors, protective strengths, and diagnostic impression. As a result, a biopsychosocial assessment template keeps documentation consistent across clinicians and organizations while meeting official standards.
The Department of Children and Families (DCF) mandates that biopsychosocial assessments completed in child welfare, family preservation, and behavioral health services include specific documentation standards.
DCF is a state-level child welfare agency, used as the name in states including Florida, Massachusetts, Connecticut, and New Jersey. Other states run the same function under different names, such as the Department of Children and Family Services or the Department of Human Services. As a result, documentation requirements vary from state to state.
In addition, all required sections need documentation, especially when assessments are submitted for case review, licensing inspections, or Title IV-E federal funding audits. Therefore, compliance management tools help track these rules instantly.
A DCF-compliant assessment covers these elements:
Qualified clinicians with appropriate licensure and training can conduct biopsychosocial assessments in DCF-regulated settings. In addition, mental health professionals working in licensed clinical settings must hold valid credentials to document diagnostic impressions and treatment recommendations.
Licensed Clinical Social Workers (LCSWs), Licensed Mental Health Counselors (LMHCs), licensed psychologists, and psychiatrists can conduct and sign biopsychosocial assessments on their own. Clinical supervisors, program managers, and case workers may gather assessment information. However, a licensed clinician must review and sign the completed form.
Scope of practice varies by state, so check your state’s requirements before handing off assessment responsibilities. Meanwhile, HIPAA compliance rules apply to all clinical documentation, including assessment forms.
Document the client’s chief complaint, reason for referral (self-referred, court-ordered, school referral, provider recommendation), and the immediate context prompting the assessment. Also, include the client’s perspective on why they are seeking help and any urgent safety concerns driving the referral.
Record all major medical diagnoses, surgical history, current medications with doses and frequencies, allergies, and substance use history including alcohol and recreational drugs. Document any physical health conditions affecting mental health or treatment planning, such as chronic pain, endocrine disorders, or neurological conditions. Finally, note pregnancy status, recent medical appointments, and healthcare provider names when known.
Document mental health diagnoses, psychiatric hospitalizations, prior treatment episodes, and current symptoms. Include trauma history (abuse, neglect, violence exposure), loss and grief history, and mental status exam findings such as mood, affect, thought content, concentration, and memory. Also, note cognitive functioning results, learning disabilities, and developmental history relevant to the current presentation.
Record family structure, relationships with primary caregivers, support access, stable and quality housing, employment or educational status, cultural background and values, spiritual beliefs or religious affiliation, and community involvement, including lifestyle stress documented under Z73.2. In addition, document access to transportation, food security, and social supports. For child welfare cases, note parental strengths, family reunification potential, and kinship resources.
A required DCF element. Document screening for suicide risk (ideation, intent, plan, access to means), self-harm, harm to others, abuse or neglect history, and exploitation risk. Also, note protective factors that reduce risk and any immediate safety steps or referrals made. Therefore, digital clinical systems support consistent risk documentation and audit trails required during DCF inspections.
A strengths-based summary highlighting client assets, coping strategies, protective factors, and signs of resilience. Also, include DSM-5-TR diagnostic codes and clinical summary of assessment findings. Finally, ensure treatment recommendations are specific, trackable, and directly tied to documented assessment data.
Follow these five operational steps to complete a compliant biopsychosocial assessment in clinical practice.
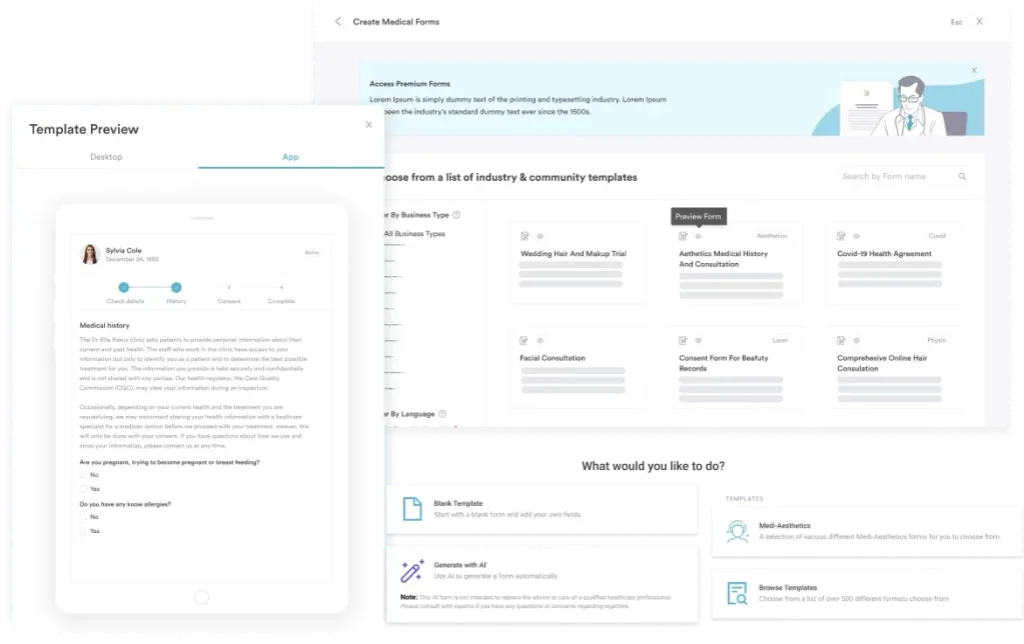
In addition, digital assessment forms reduce documentation burden and support consistent completion of all required sections before submission.
Avoid these frequent errors when completing biopsychosocial assessments for DCF submission.
Manual PDF templates and paper forms create compliance risk. For example, a missing signature or a blank risk-assessment field can go unnoticed until an inspection catches it.
Practice management software like Pabau turns the same fields into a digital form: required sections auto-flag if left empty, e-signature capture adds a timestamp automatically, and secure encrypted storage with role-based access control keeps every completed assessment protected. In addition, a complete audit log records who accessed or edited each assessment, which matters during DCF inspections.
Pabau Scribe adds another layer by drafting the assessment write-up directly from the clinical interview, structuring the biological, psychological, and social domains as the conversation happens. As a result, this cuts down on the time clinicians spend typing up notes after a session and reduces the risk of a domain being left blank.
When assessments are linked to treatment plans and appointment records within Pabau, clinicians reduce documentation duplication and maintain a single source of truth. In contrast to standalone PDF downloads, Pabau assessments integrate compliance requirements directly into your clinical workflow, making it easier to meet DCF standards on every submission.
Explore how digital assessment forms, e-signatures, and secure storage streamline DCF documentation workflows.

The biopsychosocial assessment template is essential documentation in mental health, social work, child welfare, and nurse practitioner-led private practice settings. In short, a complete assessment covers biological, psychological, and social domains, includes documented risk assessment, provides DSM-5-TR diagnostic impression, and meets DCF rules for signature, dating, and confidential storage.
Whether you use the downloadable template provided or use digital assessment forms in Pabau, ensure every required section is completed, risk screening is documented, and clinician credentials and signatures are present. Ultimately, a Book a demo of Pabau’s clinical documentation platform shows how digital assessments reduce compliance gaps and improve clinician efficiency.
Looking for a template for your psychiatric practice? Psychiatric evaluation template provides a structured form for comprehensive mental health evaluations.
Want to streamline your practice’s clinical workflows? Therapy practice management software integrates assessments, notes, and treatment planning into a single secure system.
A biopsychosocial assessment is a thorough clinical evaluation that examines how biological factors (medical conditions, medications, substance use), psychological factors (mental health history, trauma, cognitive functioning), and social factors (family, housing, employment, culture) interact to affect a person’s mental health and wellbeing. In short, it is the foundation for treatment planning in mental health, social work, and child welfare settings.
The three components are: (1) first, the biological domain-medical history, medications, substance use, physical health; (2) second, the psychological domain-mental health diagnoses, trauma, mood, cognitive functioning, mental status exam; (3) third, the social domain-family relationships, housing, employment, education, cultural background, community supports.
In short, a complete assessment includes presenting problem, reason for referral, medical and medication history, mental health diagnoses and treatment history, substance use history, family and social history, risk assessment (suicide, self-harm, safety), mental status exam, strengths and protective factors, DSM-5-TR diagnostic impression, treatment recommendations, clinician signature with credentials, and date of assessment.
Yes. In child welfare, family preservation, and behavioral health services regulated by the Department of Children and Families (DCF), biopsychosocial assessments are required documentation for case opening, service planning, and licensing compliance. In addition, DCF requires documented risk assessment, DSM-5-TR diagnosis, treatment recommendations, clinician signature with license number, and secure storage of completed forms.