Body measurement chart
Free printable body measurement chart to track waist, hips, bust, thighs, and ar...
July 23, 2026
An assisted living assessment tool evaluates functional capacity, medical needs, cognitive status, and behavioral considerations to determine resident care requirements.
The assessment covers ADLs (Activities of Daily Living) and IADLs (Instrumental Activities of Daily Living) using standardized scoring that guides level of care placement.
State regulations vary widely — use this template as a foundation and adapt per your jurisdiction’s specific regulatory requirements (e.g., Maryland COMAR 10.07.14, Minnesota Statutes 144G).
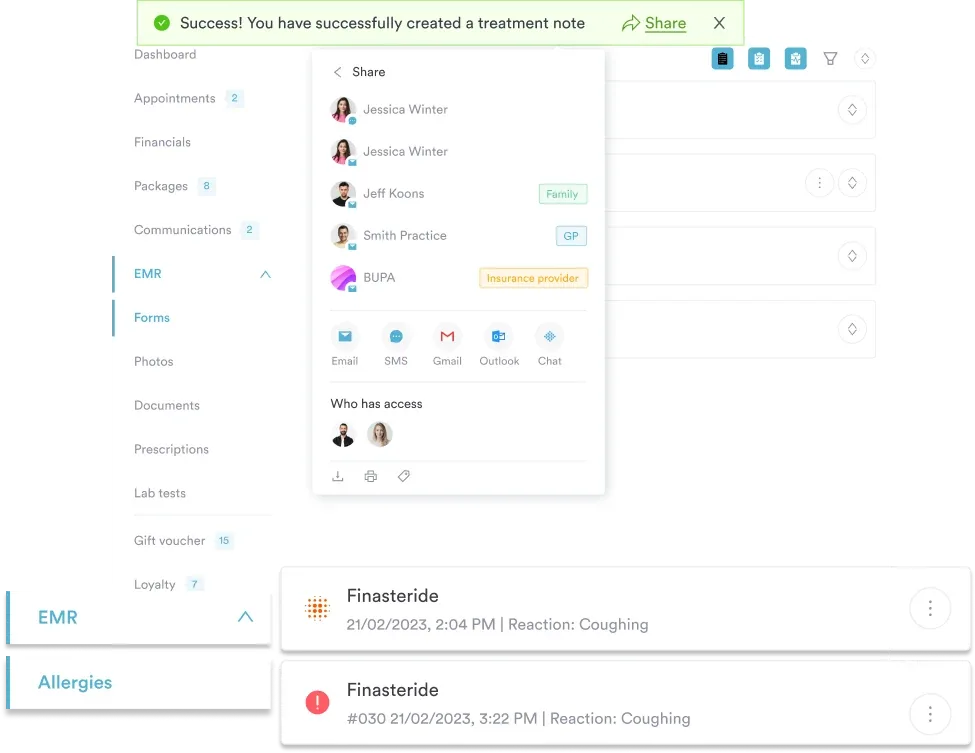
Pabau’s digital forms and client record features streamline assessment workflows, enabling care coordinators to complete evaluations, store results securely, and link findings directly to individual care plans.
A standardized evaluation form covering Activities of Daily Living (ADLs), Instrumental Activities of Daily Living (IADLs), medical and nursing care needs, cognitive and behavioral assessment, and level of care scoring for admission and ongoing resident evaluation.
Download templateAn assisted living assessment tool is a structured evaluation form that determines whether a prospective or current resident requires assisted living support and what level of care is appropriate. Care coordinators, nurses, and assisted living managers use it to document functional abilities, medical complexity, cognitive status, and behavioral considerations — producing the clinical record needed for individualized care planning and regulatory compliance.
This guide explains what the assessment covers, how to use it within your care workflow, how to translate scores into a level of care, and how practice management software like Pabau can streamline evaluation with digital assessment forms that improve documentation accuracy. For related clinical evaluation tools, see our body map template and ADHD psychological assessment for adults.
An assisted living assessment tool is a structured evaluation form that documents how residents manage daily activities, their medical and nursing requirements, cognitive abilities, behavioral health status, and any special needs. It gives care teams the objective data needed to guide admission decisions and ongoing care planning.
The tool serves three primary purposes. First, it establishes a baseline of functional and medical status at admission so care coordinators can set realistic expectations and determine support needs. Second, it generates the clinical justification for your facility’s level of care classification — critical for state licensing and Medicaid long-term services and supports compliance.
Third, it creates the foundation for a structured resident record that tracks changes over time and informs care plan updates.
At its core, the assessment works as a structured checklist covering eight key domains:
Using an assessment tool effectively requires a structured five-step workflow. Begin by scheduling a quiet, unrushed interview in the resident’s preferred environment — typically the prospective resident’s home or current care setting. Allow 45-60 minutes and gather relevant medical records, current medication lists, and any prior assessments beforehand.
Once the assessment is complete, share results with the resident and family, incorporate findings into the Individual Service Plan (ISP), and securely store the assessment in a resident portal accessible to authorized care team members. Schedule reassessment every 6-12 months or when significant functional changes occur.
State-specific guidance: Regulatory requirements vary widely. Maryland’s Resident Assessment and Level of Care Scoring Tool, published under COMAR 10.07.14, provides a validated methodology that scores residents into three levels of care. Massachusetts publishes official assisted living residency regulatory guidance.
Minnesota Statutes Section 144G and the state health department provide guidance and self-audit tools. Always consult your state’s assisted living licensure regulations before finalizing your template — adapt this tool to match your jurisdiction’s specific requirements.
Pabau's digital forms let care coordinators complete assessments on mobile or desktop, auto-save progress, and link results directly to resident records for seamless care planning.

An assessment score is only useful once it maps to a level of care. Assisted living isn’t regulated federally, so there’s no single national scale — each state, and often each facility, defines its own tiers. Most use a three-level model, some communities publish five, and memory care is treated as a distinct specialty rather than a number on the scale.
A common three-tier structure, used as the backbone of this assisted living level of care assessment tool, works like this:
Here’s a worked example. A resident who scores independent on eating and continence but needs hands-on help with bathing and dressing, plus daily medication management, typically lands in Level 2 — enough support to stay safe without the round-the-clock oversight of Level 3. Record the score, the level it maps to, and the reasoning behind it, so the determination holds up in a licensing survey.
Because level names vary between communities, always cross-reference your total against your own state’s or facility’s level of care matrix. A “Level 2” in one community may not mean the same thing in another.
The assisted living assessment tool is used across multiple care settings and professional roles.
Objective clinical documentation: A standardized form ensures every resident is evaluated on the same criteria, reducing bias and enabling meaningful comparison over time. Consistent documentation also protects your facility during regulatory surveys and liability claims.
Accurate level of care determination: Systematically evaluating functional abilities and medical complexity guides appropriate staffing models and care intensity, protecting residents and your facility from mismatches that could compromise safety or escalate costs.
Evidence-based care planning: Assessment data forms the clinical foundation for the Individual Service Plan, allowing staff to tailor interventions to each resident’s specific functional profile and medical needs.
Regulatory compliance and defensibility: Standardized assessments align with state licensure requirements. Billing for related caregiver evaluations may involve CPT code 96161 (caregiver health risk assessment) or CPT code 96160 (patient-focused health risk assessment). Documentation demonstrates due diligence during licensing inspections and quality audits, reducing regulatory risk.
Family communication and informed consent: Clear assessment results help families understand why a recommended level of care is appropriate and set realistic expectations for services and outcomes.
Conduct reassessments at regular intervals (every 6-12 months) and after significant events (hospitalization, falls, medication changes, family concerns). Compare current scores to baseline to identify functional decline, stability, or improvement, allowing care teams to adjust support proactively rather than reactively.
Relevant diagnostic codes for cognitive or behavioral findings include ICD-10 Code F02.80 (dementia in other diseases classified elsewhere), ICD-10 Code F06.31 (mood disorder due to known physiological condition), and ICD-10 Code F59 (unspecified behavioral syndromes) for presentations that don’t fit a more specific category.
Many assisted living facilities complete assessments on paper and file them in a cabinet, losing the connection between findings and ongoing care planning. Going paperless closes that loop: care coordinators complete the evaluation on mobile or desktop, the system auto-saves progress, and results flow directly into each resident’s record.
Automated care workflows can then trigger follow-up tasks — e.g., “Fall risk score >3: schedule PT evaluation within 7 days.”
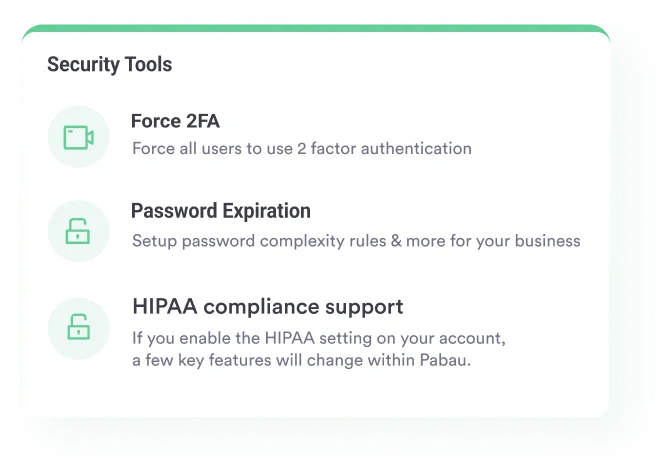
Digital storage also enables rapid access during family meetings, clinician consultations, or regulatory reviews. Compliance features keep assessment data encrypted, audit-logged, and accessible only to authorized staff — meeting HIPAA and state privacy requirements. For broader context on digital tools in care settings, see digital patient engagement strategies.
Assisted living regulations are state-specific. Maryland, Minnesota, and Rhode Island each have published standardized assessment tools and scoring methodologies. Some states mandate specific assessment instruments; others allow facilities to design custom tools provided they evaluate core domains (ADLs, IADLs, cognitive status, medical needs, behavior, fall risk).
Before deploying this template, check your state health department website for: required assessment forms, mandated scoring methods, minimum assessment frequency, who is authorized to conduct assessments (RN vs. social worker vs. care coordinator), and how results must be documented and retained.
The HCPCS Code H2015 (comprehensive community support services) billing guide may also be relevant for facilities billing community-based care. Adapt the template to match your state’s specific language, item definitions, and scoring protocols.
If your state mandates a specific assessment tool, use it as your primary document. If your state allows facility-designed tools, use this template as your foundation and customize domains or scoring per your facility’s care model and state guidance.
An assisted living assessment tool converts subjective impressions into objective, defensible clinical data. Systematically evaluating ADLs, IADLs, medical complexity, cognitive status, and behavioral factors lets care coordinators and facility managers match residents with appropriate care levels, build evidence-based care plans, and satisfy regulatory requirements.
Download this free template, adapt it to your state’s requirements, and integrate it into integrated care management workflows for faster, more accurate assessments and stronger compliance.
Need guidance on regulatory compliance? HIPAA compliance software helps protect assessment data through the privacy and security safeguards facilities are required to have in place.
Want to streamline your resident intake process? Medical forms at your healthcare practice explains how to design and deploy assessment workflows effectively.
Looking for software to manage assessments? What is practice management software shows how practice management platforms simplify documentation and care coordination.
An assisted living assessment tool is a standardized evaluation form that documents an individual’s functional abilities (ADLs and IADLs), medical and nursing care needs, cognitive status, and behavioral health to determine the appropriate level of care and guide care planning.
Licensed nurses (RNs), care coordinators, social workers, or facility intake staff complete assessments. Some states mandate an RN complete the assessment; others allow trained care coordinators under clinical supervision.
Conduct full reassessments every 6-12 months or immediately after significant events (hospitalization, falls, medication changes, family concerns, or notable functional decline).
This template covers core domains (ADLs, IADLs, medical needs, cognitive and behavioral assessment, fall risk). Check your state health department for required forms, scoring methods, or regulatory adaptations before deployment.
Use this tool for both admission evaluations and ongoing resident reassessment. Regular reassessment (every 6-12 months) detects functional changes and supports proactive care plan adjustments.
It examines the resident’s activities of daily living (ADLs) like bathing, dressing, and transferring; instrumental activities such as medication and meal management; cognitive and behavioral status; medical and nursing needs; nutrition; and fall risk. Together, these determine the appropriate level of care.
Most communities use three levels — minimal, moderate, and extensive assistance — while some publish up to five, with memory care as a separate specialty. Each state and facility defines its own tiers, so the same label can mean different things between communities. A resident’s assessment score maps to the level that matches their support needs.