Body measurement chart
Free printable body measurement chart to track waist, hips, bust, thighs, and ar...
Last Updated: July 28, 2026
A cytarabine administration note records every step of chemotherapy delivery: patient ID, route verification, dose calculation, diluent selection, and infusion monitoring parameters.
Preservative-free cytarabine is mandatory for intrathecal routes; benzyl alcohol diluents are contraindicated in neonates and high-dose regimens – documentation must reflect this critical safety distinction.
Pre-administration checks prevent catastrophic errors (especially in pediatric intrathecal dosing); post-administration observations capture adverse reactions and guide clinical decision-making.
Pabau’s digital forms and client record system standardize drug administration documentation workflows, supporting compliance with FDA labeling and oncology nursing standards.
A ready-to-use documentation template covering pre-administration patient verification, cytarabine preparation steps (diluent selection, concentration calculation, preservative-free confirmation), route-specific administration protocols (IV continuous/bolus, intrathecal, subcutaneous), infusion monitoring parameters, and post-administration clinical observations for oncology nursing teams.
Download templateA cytarabine administration note is a structured clinical record documenting the complete cytarabine infusion event. It captures pre-administration verification steps, drug preparation details, route of administration, dosage confirmation, infusion parameters, and post-administration observations.
This template helps oncology nurses and clinical staff follow best practices during every cytarabine administration. It also keeps documentation aligned with the FDA prescribing information for cytarabine.
Cytarabine (Ara-C) is a chemotherapy drug, specifically an antimetabolite antineoplastic agent. It treats acute myeloid leukemia (AML), acute non-lymphocytic leukemia (ANLL), and lymphomas.
Clinicians can give it four ways: intravenous infusion, intravenous bolus, subcutaneous injection, or intrathecal injection. Each route has its own prep needs, diluent details, and safety points.
This documentation captures those route-specific details and confirms clinicians verify the correct preparation before administration. That verification step is a critical safeguard against potentially fatal dosing errors, particularly in pediatric intrathecal administration.
This template meets the record-keeping rules set by the FDA, oncology nursing standards (Oncology Nursing Society), and hospital policy. It creates a permanent record tied to the treating clinician and supports quality audits, adverse-event reviews, and compliance checks.
The template mirrors the workflow oncology nurses follow when they give cytarabine, step by step. Each step prompts a check before the drug reaches the patient, which cuts errors and builds an auditable record.
Once completed, the template becomes part of the permanent medical record and supports quality reviews, clinical audits, and digital intake forms integration within your oncology practice management system.
This template is essential for oncology and hematology practices and comprehensive cancer centers where cytarabine is a standard treatment agent. Oncology nurses and clinical staff use it to document every cytarabine administration safely and consistently.
It also fits a range of settings: hospital inpatient units treating leukemia patients, outpatient chemotherapy infusion centers running on infusion practice management software, and multi-location oncology groups. Each one benefits from a standardized template that prevents errors and supports compliance.
Practices preparing for accreditation surveys also depend on templates like this. Bodies such as the Joint Commission, DNV GL, and CAP (in laboratory settings) look for documented adherence to best practices. Solo practitioners and small group practices use it too, to keep documentation consistent across clinicians and maintain continuity when staff change.
Safety through standardization: A structured template eliminates the guesswork that leads to medication errors. Pre-printed fields force clinicians to verify critical details (route, diluent, dose) before administration. This is particularly vital for cytarabine, where high-dose and intrathecal regimens carry narrow safety margins.
Regulatory compliance: The template captures the elements required by FDA prescribing labeling, CMS documentation standards, and Oncology Nursing Society (ONS) chemotherapy administration guidelines. It creates an auditable record that satisfies accreditation bodies and protects your practice during compliance reviews.
Adverse event investigation: When adverse reactions occur, a detailed administration record provides a complete timeline of what was administered, how, when, and what clinical signs followed. This supports rapid root-cause analysis and guides clinical management of complications like cytarabine syndrome or myelosuppression.
Clinical communication: The template creates a shared reference point for all clinicians involved in the patient’s care. Oncologists, nurses, and pharmacists can review the same structured record without ambiguity. When you keep comprehensive client records in practice management software like Pabau, the template integrates into the broader patient history.
Institutional knowledge: Over time, aggregated templates reveal clear patterns. You can see which patient populations react most often, which routes are used most, and which preparation errors recur. This data informs staff training priorities and process improvements. The same principle drives protocol tracking in a regenerative medicine EMR, where aggregated outcome data shapes future dosing decisions.
Pabau's digital forms and client record system integrate drug administration templates directly into your oncology workflow, eliminating paper and ensuring every infusion is documented, auditable, and compliant.

Automate your pre-administration verification checklist using digital forms. Build a checklist that flags missing data (renal function, allergy history, prior adverse reactions) before the nurse opens the cytarabine vial. That way the record is complete before the infusion starts, not reconstructed afterward from memory.
Cytarabine’s four administration routes carry distinct pharmacological profiles and preparation requirements. This documentation must capture those differences because each route carries unique adverse event risks and monitoring parameters.
This is the standard induction route for AML. Typical regimens give 100 mg/m² per day over 24 hours, often across 7 days of induction. You dilute the cytarabine into 5% Dextrose in Water or 0.9% Sodium Chloride injection, then infuse it through a central line or peripheral IV. A central line lowers the risk of vein inflammation.
Some outpatient protocols deliver the infusion through a portable ambulatory infusion pump, letting the patient complete the cycle at home. Continuous infusions reach steady-state plasma concentrations within 8 to 24 hours, so document the infusion start time and target completion time.
High-dose cytarabine regimens (1 to 3 g/m² IV over 3 hours every 12 hours) need closer monitoring and a carefully chosen diluent, and you must never use benzyl alcohol. Patients with poor kidney function (creatinine clearance below 60 mL/min) face a higher risk of brain and nerve toxicity, so oncology standards call for a lower dose.
High-dose therapy also carries a risk of cerebellar neurotoxicity (ataxia, slurred speech) and ocular toxicity. Many protocols add prophylactic corticosteroid eye drops and a pre-dose neurological exam. Your template must flag renal function status and record any dose adjustments alongside the neurological and ophthalmic checks performed.
Clinicians use intrathecal cytarabine (preservative-free only) to prevent leukemia in the central nervous system, at doses of 30 to 100 mg based on the patient’s age and protocol. The template must explicitly confirm that the preparation used is preservative-free, because benzyl alcohol is neurotoxic when injected into cerebrospinal fluid.
Every intrathecal dose requires special handling, post-injection observation, and an independent double-check by a second chemo-trained clinician. Pediatric intrathecal dosing errors have caused permanent harm, so this route demands the highest verification rigor.
Clinicians use subcutaneous cytarabine in maintenance therapy and in some low-dose protocols. The template should note the injection site (abdomen, thigh, or upper arm), any local reactions such as firmness or redness, and time to absorption. Subcutaneous administration typically produces lower, more sustained plasma concentrations than an IV bolus.
Oncology documentation is audited more frequently and more carefully than most healthcare records because chemotherapy errors carry life-or-death consequences. A template that follows best practices protects both patient safety and clinician accountability.
Align your template with HIPAA-compliant documentation standards and institutionalize its use through electronic health records or paper-based nursing protocols. Never skip sections or leave fields blank. Incomplete records suggest incomplete verification, which invites regulatory scrutiny and puts patients at risk.
Real-time documentation (not retrospective chart completion hours later) captures observations accurately. Adverse reactions like cytarabine syndrome often develop during or immediately after infusion. Documenting the exact time of onset helps clinicians tell true drug toxicity from unrelated symptoms. Use timestamps for infusion start, end, and all notable clinical events.
Build your automated documentation workflows around mandatory fields: patient ID, dose, route, diluent type, and infusion time. Add validation logic that blocks submission when a critical field is empty. This enforcement works far better than verbal reminders or periodic audits.
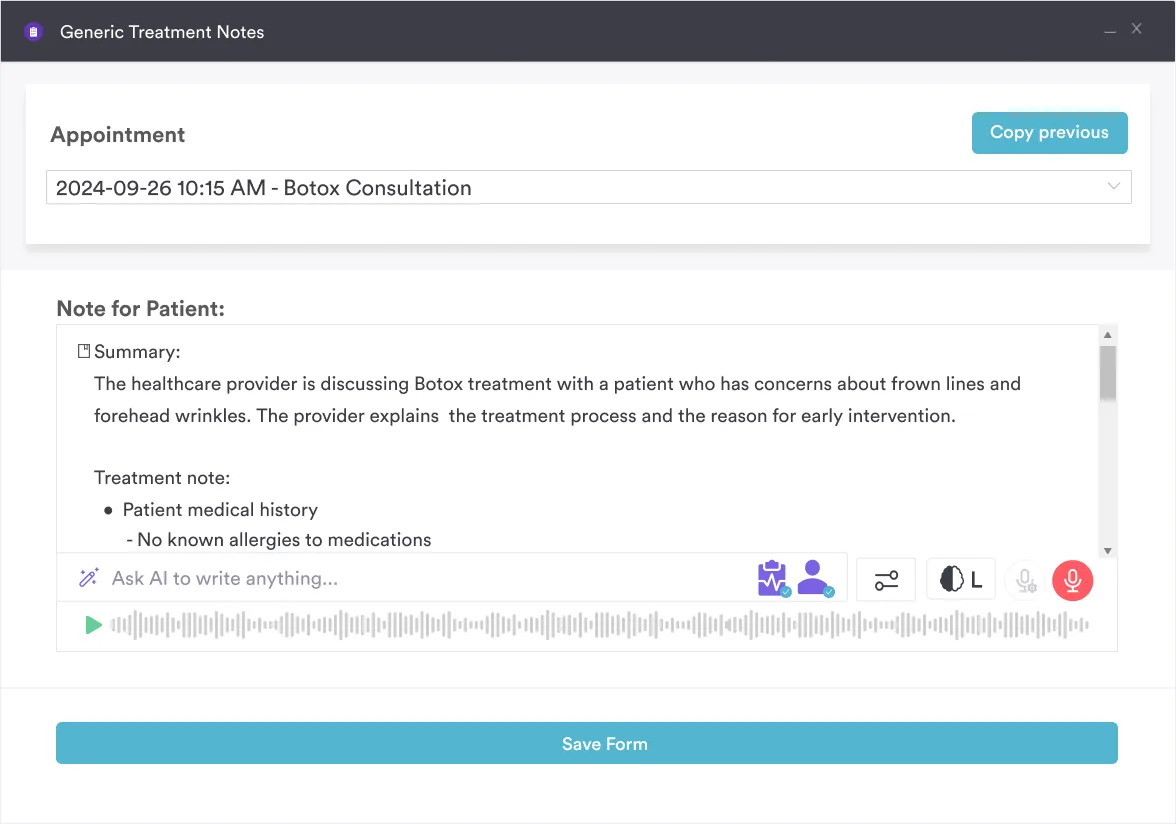
The template works best when integrated into a broader clinical documentation system. Print copies for each scheduled infusion, or use Pabau Scribe, our AI scribe, to structure notes after each infusion session. Store completed templates in your patient’s permanent medical record, linking them to the date of service and the treating clinician’s name for accountability.
Review aggregated templates monthly to identify trends (common adverse reactions, preparation errors, route-switching patterns). Share findings with your oncology team during clinical meetings to reinforce safe practices and update protocols based on real-world experience. Over time, individual administration notes become the evidence base for protocol updates the whole team follows.
A structured cytarabine administration note is essential for any oncology practice giving this chemotherapy agent. It captures pre-administration verification, route-specific preparation details, infusion parameters, and post-administration observations in a format that satisfies FDA labeling requirements and nursing standards.
The template creates a permanent, auditable record that protects patient safety and clinician accountability. Book a demo to see how Pabau’s digital forms and client record system can bring this template into your daily workflow and replace inconsistent paper documentation.
Documenting other cancer-care billing details? HCPCS G0103 covers PSA screening documentation and reimbursement, another piece of the oncology billing picture.
Tracking post-surgical oncology status codes? ICD-10 Z90.3 documents acquired absence of the stomach, common in the history of GI cancer patients.
Need a reference for another injectable drug code? HCPCS J0178 covers billing for aflibercept injections, a different specialty but the same administration-note discipline.
A cytarabine drug administration note is a structured template that records every infusion: patient ID, order checks, drug prep (concentration and diluent), route, dose confirmation, infusion details (rate, duration, carrier solution), and post-infusion notes on any reactions, the finish time, and how the patient responded.
A chemotherapy-trained nurse should give cytarabine, checking the order, dose, and route against the protocol and running an independent double-check for intrathecal and high doses. Confirm preservative-free prep for intrathecal use, give anti-nausea drugs before highly emetic regimens, and track blood counts, liver function, and kidney function throughout. Treat cytarabine as a hazardous drug and record every check.
Benzyl alcohol, a preservative in standard cytarabine vials, harms nerves when it reaches the spinal fluid. The FDA bars benzyl-alcohol diluents for intrathecal use because they can cause lasting nerve damage. Use only preservative-free cytarabine for this route, and confirm and record it before every intrathecal dose.
Standard induction is about 100 mg/m² per day as a continuous IV infusion for 7 days. Consolidation or salvage therapy uses high doses of 1 to 3 g/m² every 12 hours, and intrathecal doses run 30 to 100 mg by age and protocol. Always check the dose against the treatment protocol and record any change made for kidney or liver function.
Cytarabine syndrome is an acute infusion reaction (fever, muscle pain, chest pain, rash, malaise) that usually shows up 6 to 12 hours after a high-dose infusion. Note any of these symptoms in the post-infusion section with the exact onset time. Dexamethasone and NSAIDs often clear it within 48 hours, so record the treatment given and the patient’s response.
Cytarabine side effects are mostly dose-related. The most common is bone-marrow suppression, meaning low red cells, white cells, and platelets. White cells dip first around days 7 to 9, then fall to a deeper low around days 15 to 24. Platelets start dropping near day 5 and bottom out around days 12 to 15. Nausea, vomiting, mouth sores, and higher liver enzymes are also common, and high doses add a risk of cerebellar and eye toxicity. Cytarabine syndrome (fever, muscle pain, rash) can appear within hours, so record any reaction and its onset time.
A vial mixed with bacteriostatic water for injection lasts up to 48 hours at room temperature (59 to 86°F / 15 to 30°C). Once you dilute it further into an infusion fluid, such as 5% Dextrose in Water, 0.9% Sodium Chloride, or sterile water, it stays stable for up to 192 hours (8 days). Sterility practice usually means using it within 24 hours, so record the mixing and dilution times and follow your hospital’s shorter limit.