Body measurement chart
Free printable body measurement chart to track waist, hips, bust, thighs, and ar...
Last Updated: July 28, 2026
A Doppler ultrasound report is a structured clinical document recording blood flow assessment using spectral, color, and power Doppler techniques with standardized vascular terminology.
Normal reference values for peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistive index (RI) vary by vessel and anatomical region — always reference published ACR or AIUM guidelines.
A standardized report template prevents omissions, improves clinical communication, and reduces liability exposure during audits or peer review.
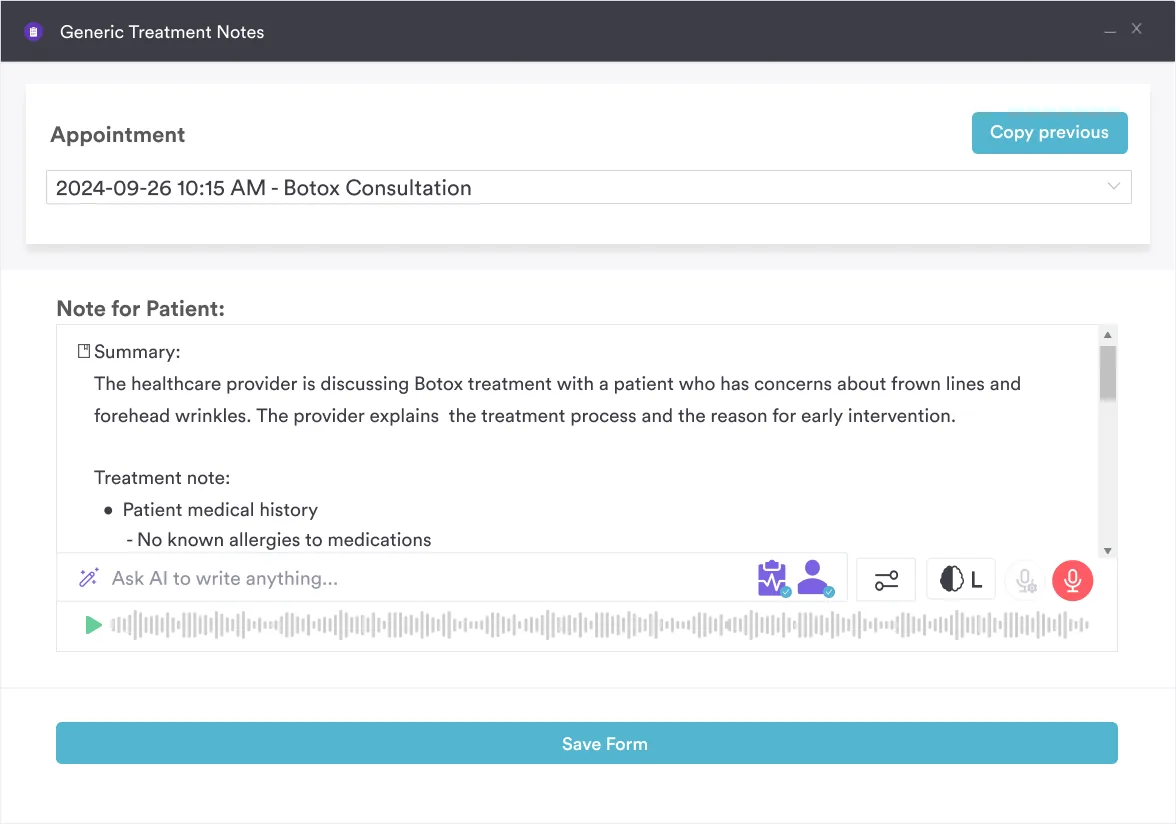
Digital forms in practice management software like Pabau let you build the report once and reuse it across every sonographer and location, so documentation stays consistent.
Download your free Doppler ultrasound report template
A comprehensive diagnostic template for documenting Doppler ultrasound findings across multiple vascular regions, with structured fields for spectral Doppler measurements, color Doppler findings, clinical impressions, and standardized vascular terminology.
Download templateA Doppler ultrasound report documents blood flow through arteries and veins from a non-invasive scan. Unlike standard B-mode ultrasound, which creates static tissue images, Doppler detects the motion of red blood cells and converts frequency shifts into velocity measurements shown as spectral waveforms or color-coded flow maps.
Radiologists and sonographers read that information to diagnose stenosis, occlusion, thrombosis, and other blood flow abnormalities.
The problem is that normal values and required fields change with every vessel, so one flat form never fits a carotid scan, a leg vein study, and an obstetric Doppler equally well. This template branches by anatomical region and pairs each with its own reference bands.
It works as a standalone PDF, or you can rebuild it as a digital form inside practice management software like Pabau, so every sonographer and location documents the same way. The sections below explain how to fill it in and how each specialty section differs.
A Doppler ultrasound report is the formal diagnostic documentation generated after a Doppler examination. It communicates findings to the referring physician, creates a legal medical record, supports accurate billing and coding, and provides a baseline for future comparison studies.
The report captures three elements. Technical information covers which Doppler modes and transducers were used, patient preparation, and imaging quality. Measurement data records quantitative hemodynamic parameters like PSV and RI for each vessel studied. Clinical interpretation states whether findings are normal, abnormal, or uncertain, and what pathology is present.
A study usually combines color Doppler to locate vessels and show flow direction, spectral (pulsed or continuous wave) Doppler to quantify velocities, and sometimes power Doppler for slow flow. When B-mode imaging and Doppler are recorded together, the study is often called a duplex ultrasound.
Different anatomical regions — carotid arteries, renal vessels, lower and upper limb arteries, obstetric umbilical artery, penile or testicular vasculature — need their own report sections because normal reference ranges and clinical significance vary by vessel.
Practices often struggle with fragmented report formats, where sonographers record findings in free-text notes rather than structured fields. That increases omission risk and complicates peer review. Digital forms with conditional logic can automatically adjust report sections based on which anatomical region was scanned, cutting unnecessary data entry.
A practical Doppler ultrasound report workflow follows five operational steps:
Pabau Scribe, our AI scribe, can speed up report completion by transcribing sonographer voice notes into structured fields, which cuts manual typing and standardizes terminology. That helps most in high-volume imaging centers, where sonographer fatigue leads to incomplete or inconsistent reports.
Doppler ultrasound reports serve multiple clinical audiences. Radiologists and vascular surgeons rely on precise hemodynamic data to grade stenosis severity and plan interventions. Cardiologists and internists use patient care workflows grounded in imaging results to adjust medications or schedule follow-up.
Obstetric care teams in OB/GYN practices depend on fetal and placental Doppler findings to identify high-risk pregnancies and guide delivery timing. Primary care physicians and urgent care clinics order peripheral vascular Doppler to rule out DVT or PAD.
Specialized imaging centers — vascular laboratories, interventional radiology suites, fetal medicine units, and standalone ultrasound practices — benefit most from standardized templates because they process high volumes and need consistent documentation across multiple sonographers.
Multi-location practices face a particular challenge: without a unified report template, each location develops its own format, making it hard for radiologists to compare studies or for referring physicians to understand findings from different branches.
Standardization and compliance: A templated format ensures every sonographer documents the same required fields. This reduces variability, improves quality, and simplifies peer review and accreditation audits. Accreditation bodies such as the American College of Radiology (ACR) and the Intersocietal Accreditation Commission (IAC) expect imaging facilities to demonstrate consistent documentation practices.
Clinical safety and liability protection: Complete, accurate Doppler reports reduce diagnostic errors and support clinical decision-making. If a patient later brings litigation over a delayed diagnosis, a thorough contemporaneous report is your strongest defense. Vague findings (“possible narrowing”) or missing measurements increase medicolegal exposure.
Billing and coding accuracy: Structured reports that state the exact anatomical regions and Doppler modes scanned support accurate procedure coding. This matters because the code depends on the study performed — for example, the CPT code for a carotid Doppler ultrasound differs from a lower limb venous study — and incomplete documentation often leads to claim denials or downcoding that reduces revenue.
Workflow efficiency: Once a template is embedded into your practice management system or clinical records platform, sonographers complete reports faster using dropdown menus and auto-populated fields rather than free-text composition. This reduces transcription errors and turnaround time to referring physicians.
Different clinical scenarios need region-specific report formats. A carotid Doppler ultrasound report template emphasizes plaque morphology and degree of stenosis (mild under 50%, moderate 50-69%, severe 70% or greater). Renal Doppler focuses on peak systolic velocity ratios and accessory renal artery detection to screen for renovascular hypertension.
A lower limb Doppler ultrasound report template documents arterial waveforms and venous compressibility to assess PAD or rule out DVT, while an upper limb Doppler ultrasound report covers the subclavian, axillary, and brachial vessels. Obstetric Doppler highlights umbilical artery and middle cerebral artery findings to assess placental insufficiency and fetal well-being.
A comprehensive template should include branching logic. After the sonographer selects the anatomical region, the form displays only the relevant sections, field labels, and reference value tables for that region. This reduces cognitive load and makes sure the right measurements are always captured.
Building each variant once and reusing it keeps every branch on the same reference bands.
Every Doppler ultrasound report must include standard hemodynamic measurements. Peak systolic velocity and end-diastolic velocity anchor stenosis grading, while the resistive index and pulsatility index describe downstream resistance:
Always compare measured values against published reference ranges for the vessel and patient population. For example, normal carotid artery PSV is typically under 125 cm/s; PSV of 125-230 cm/s suggests 50-69% stenosis; PSV above 230 cm/s indicates 70% or greater stenosis.
Obstetric reference values change sharply with gestational age, so documenting the precise gestational week is essential for accurate interpretation.
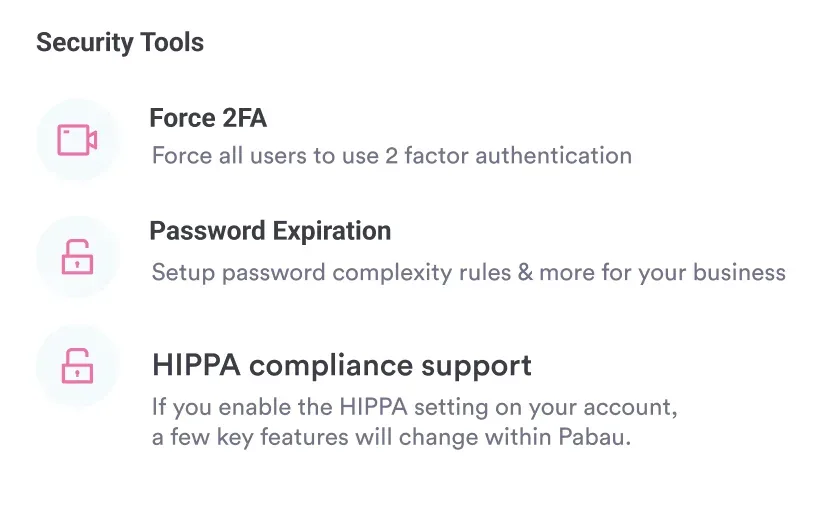
Doppler ultrasound reports are regulated medical records subject to HIPAA (US) and GDPR (EU) compliance requirements. Report templates should include fields for patient consent and data protection acknowledgment.
Obstetric Doppler in the first trimester carries higher thermal and mechanical index risk, so reports should document that pulsed Doppler intensities are higher than B-mode and that use was justified by clinical indication per FDA and AIUM guidelines.
Penile Doppler for erectile dysfunction in men’s health practices requires neutral clinical language. Focus on hemodynamic parameters rather than functional outcomes.
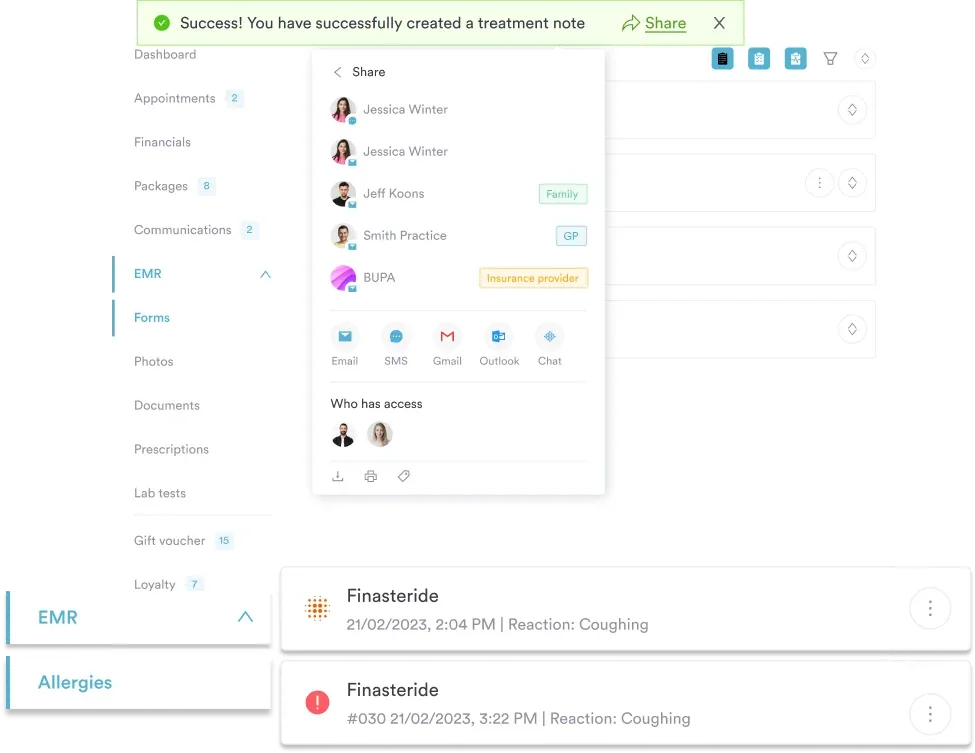
For multi-location imaging practices, centralized compliance workflows and audit trails ensure all locations use the same template version and that regulatory updates reach every branch. Version control prevents sonographers at different sites from applying outdated reference values.
Professional organizations publish standardized reporting lexicons to improve clarity and reduce ambiguity. AIUM reporting standards define terms like “normal,” “abnormal,” “indeterminate,” and “technical failure” with explicit criteria.
For stenosis grading, the SRU (Society of Radiologists in Ultrasound) consensus criteria unify carotid stenosis classification. For obstetric Doppler, ISUOG practice guidelines provide gestational-age-specific nomograms and terminology for normal and abnormal findings.
Use your template to enforce this standardized language through dropdown menus and auto-suggested findings. Instead of allowing free-text descriptions like “narrowing appears present,” constrain options to “mild stenosis (under 50% diameter reduction),” “moderate stenosis (50-69% diameter reduction),” or “severe stenosis (70% or greater diameter reduction).” This enforces consistent grading and simplifies audit and peer review.
Pabau's digital forms and automated clinical workflows help imaging departments standardize Doppler reports, reduce transcription time, and ensure regulatory compliance across all locations.

Accurate Doppler reporting depends on technical detail and clinical context. Angle-correct all velocity measurements so the Doppler cursor aligns with vessel flow (under 60 degrees); skipping this introduces errors that propagate into stenosis grading.
Sample the same vessel at multiple points to tell focal from diffuse disease. Always compare bilateral vessels when imaging paired structures (both carotid arteries, both lower extremity arteries) to spot asymmetries that suggest pathology.
Document when vessels are not fully visualized and explain why (for example, “Right ICA ostium not visualized due to tortuous anatomy; clinical correlation recommended”). Transparent communication about study limitations with referring physicians prevents misinterpretation.
For borderline findings (such as PSV of 225 cm/s near the 70% stenosis threshold), note the gray zone and recommend clinical correlation or repeat imaging in 3-6 months.
Obstetric Doppler reports must include precise gestational age (from LMP and early ultrasound), since normal reference ranges shift week to week. Penile Doppler studies should document erectile status at the time of the exam (flaccid or induced tumescence), because PSV and flow patterns differ sharply.
Venous Doppler must document transducer position, the compression maneuvers performed, and whether color fill is present — sonographers sometimes omit these details assuming they are obvious, but they are essential for reproducibility.
A comprehensive Doppler ultrasound report template ensures clinicians document findings consistently, completely, and in clinically defensible detail. Standardized fields for anatomical regions, Doppler modes, reference measurements (PSV, EDV, RI), and interpretation grading remove the omissions that lead to diagnostic errors or liability exposure.
For imaging centers and multi-location practices, embedding the template into your practice management system guarantees sonographers use the same version, reference values, and terminology across all locations — the foundation of quality assurance, peer review, and regulatory compliance.
Book a demo with Pabau to see how digital forms and automated clinical workflows can streamline your imaging documentation and free up clinician time for patient care.
Need guidance on standardized clinical documentation formats? Intake assessment template applies the same structured-field approach to capturing consistent clinical information from the first patient visit.
Curious how other specialties standardize exam documentation? Pediatric neurological exam checklist uses the same structured-field format to keep exam findings consistent across every clinician who completes it.
Want treatment documentation that stays consistent across a care team? Pain management treatment template applies the same structured approach to tracking a patient’s plan across every provider involved.
A Doppler ultrasound report is a clinical document recording findings from a Doppler ultrasound examination, which uses sound waves to measure blood flow velocity through vessels and detect abnormalities like stenosis, occlusion, or incompetence. It includes patient demographics, technical parameters, quantitative hemodynamic measurements (PSV, EDV, RI), B-mode findings, and clinical interpretation graded as normal, abnormal, or indeterminate.
Normal values vary by vessel and patient population. Carotid artery PSV is typically under 125 cm/s, with 125-230 cm/s suggesting 50-69% stenosis and above 230 cm/s indicating 70% or greater stenosis. A normal umbilical artery resistive index in the third trimester runs 0.58-0.74. A normal color Doppler report describes patent vessels with expected flow direction and velocities that fall within the published reference band for that vessel, so always state which reference standard you applied.
Read a Doppler ultrasound report in three passes. First check the technical section to confirm which modes and transducer were used and that the Doppler angle was under 60 degrees. Then compare the measured velocities (PSV, EDV) and indices (RI, PI) against the reference range for that vessel. Finally read the clinical impression, which grades the finding as normal, abnormal with severity, or indeterminate, and note any stated limitations or follow-up recommendation.
Standardized templates ensure consistent capture of required fields across all sonographers and locations, reducing omissions and variability. This improves clinical communication with referring physicians, simplifies peer review and regulatory audits, supports accurate billing and coding, reduces liability exposure, and enables meaningful comparison of serial studies over time.
Spectral Doppler displays blood flow velocity as a waveform graph over time, allowing precise measurement of PSV, EDV, and calculation of RI; it provides quantitative data but only samples one location at a time. Color Doppler overlays velocity information on B-mode images, showing flow direction and relative velocity across a 2D region, but does not provide exact quantitative measurements. Both modes complement each other: color localizes vessels and detects flow; spectral quantifies velocities for clinical grading.
Doppler reports are medical records subject to HIPAA (US) and GDPR (EU) compliance requirements for patient privacy and data security. Obstetric Doppler in the first trimester must comply with FDA and AIUM guidelines on safe thermal and mechanical index limits. Vascular laboratory reports should follow AIUM standards. Facilities pursuing accreditation from the American College of Radiology (ACR) or the Intersocietal Accreditation Commission (IAC) must demonstrate consistent documentation. Always verify applicable regulations in your jurisdiction.