Medical power of attorney
A medical power of attorney names an agent to decide your care once a physician ...
Last Updated: August 6, 2026
An advance care planning discussion visit is a billable Medicare encounter (CPT 99497/99498) where clinicians facilitate conversation about patient values, goals of care, advance directives, and healthcare proxies.
Medicare Part B fully covers ACP visits with zero patient cost-sharing when billed during an Annual Wellness Visit. CPT 99497 covers the first 30 minutes, and CPT 99498 covers each additional 30 minutes.
Complete ACP documentation must include patient consent, goals-of-care narrative, advance directive status, healthcare proxy designation, POLST/MOLST form status (where applicable), and next-step action items.
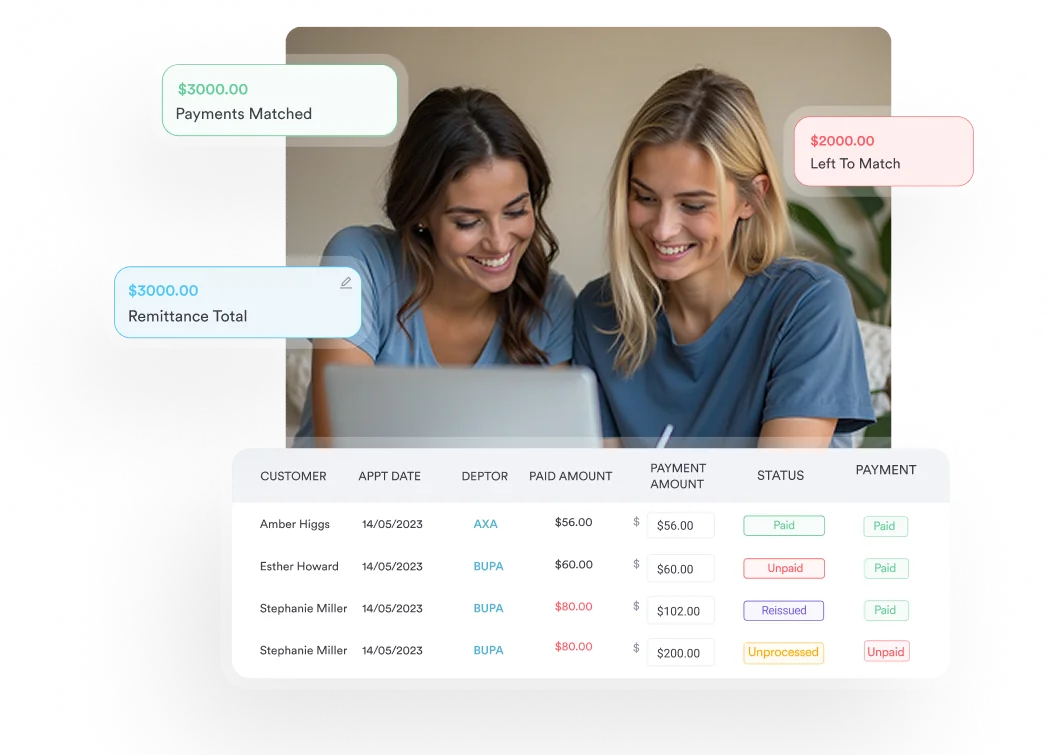
Practice management software like Pabau streamlines ACP visit documentation with digital forms and customizable templates.
A ready-to-use template covering patient demographics, contraindication screening, informed consent, values and goals-of-care documentation, advance directive status, healthcare proxy designation, POLST form review, and post-visit action items.
Download templateMost advance care planning guides teach you how to have the conversation, while the majority of billing guides just list the CPT codes.
Almost none put both in one place.
That disconnect is why a Medicare-billable advance care planning discussion visit so often becomes a strong conversation that gets under-documented and under-billed, especially in a busy primary care practice.
This guide closes the loop: a downloadable template, the exact code stack (CPT 99497 and 99498, plus same-day Annual Wellness Visit billing), and a validated step-by-step conversation framework your team can use at the next appointment.
An advance care planning discussion visit is a dedicated clinical encounter where a provider and patient discuss the patient’s values, goals of care, and treatment preferences in the context of possible future health scenarios such as serious illness, decline, or end-of-life care.
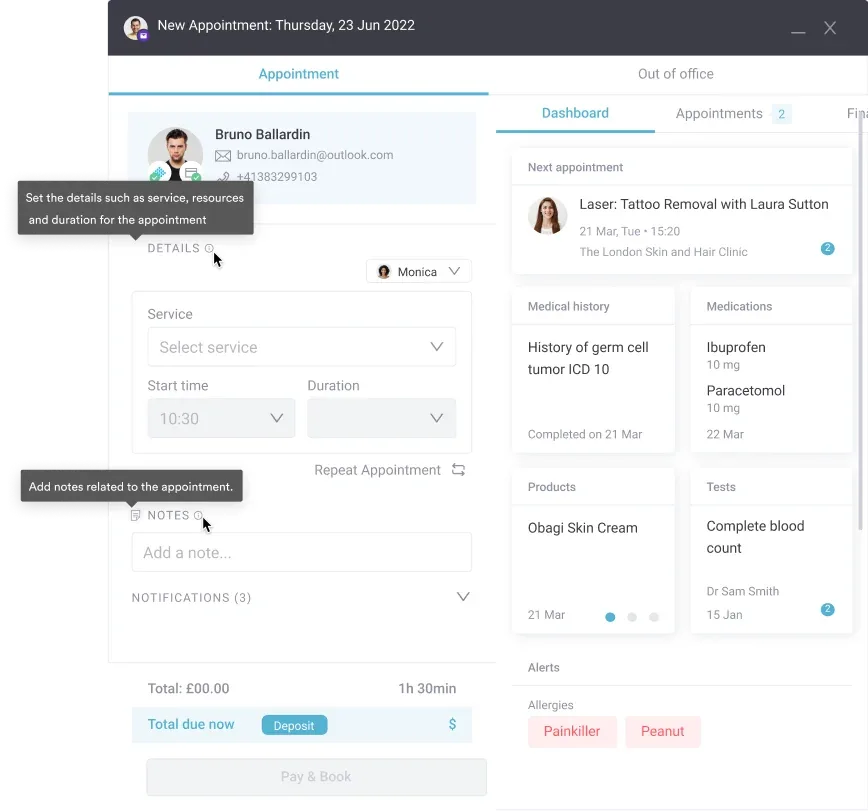
Unlike a routine office visit, an advance care planning discussion visit requires dedicated time, a quiet setting, and family involvement where appropriate. Many practices use digital intake forms and structured templates to reduce clinician burden and make sure no essential elements are missed.
Medicare created two dedicated codes so this time-intensive conversation is reimbursed on its own instead of being bundled into an office visit. The advance care planning CPT code for the first block of time is 99497, and CPT 99498 is the add-on for each additional 30 minutes. The table below gives the 99497 CPT code description alongside time and reimbursement.
Both codes require documentation of time and can be billed the same day as an Annual Wellness Visit (G0438/G0439) without a bundling penalty. That’s a key claims management advantage for primary care practices.
One detail the code descriptions leave out: there is no ICD-10 code specific to advance care planning. You report the diagnosis that prompted the conversation, usually the patient’s relevant chronic or serious condition, or a general counseling code such as Z71.89 for a standalone preventive discussion. Matching the right ICD-10 code to advance care planning is what keeps a well-documented visit from being denied.
Medicare Part B covers advance care planning discussion visits as a preventive benefit with no frequency restrictions, which matters most for preventive care practices billing ACP alongside an Annual Wellness Visit. Patients aren’t required to have an ACP visit annually or on a set schedule.
It’s patient-initiated or clinician-recommended based on clinical appropriateness. The 99497 billing guidelines below hold whether the visit stands alone or rides along with another service.
CMS preventive services guidance confirms the ACP benefit applies nationally to all Medicare beneficiaries, though state scope-of-practice laws determine who can conduct the visit.
A compliant advance care planning discussion visit template captures six elements that together meet the advance care planning documentation requirements for billing, satisfy legal documentation standards, and reflect clinical best practice. Practices using comprehensive client records embed these as a structured form so the same fields are captured at every visit.
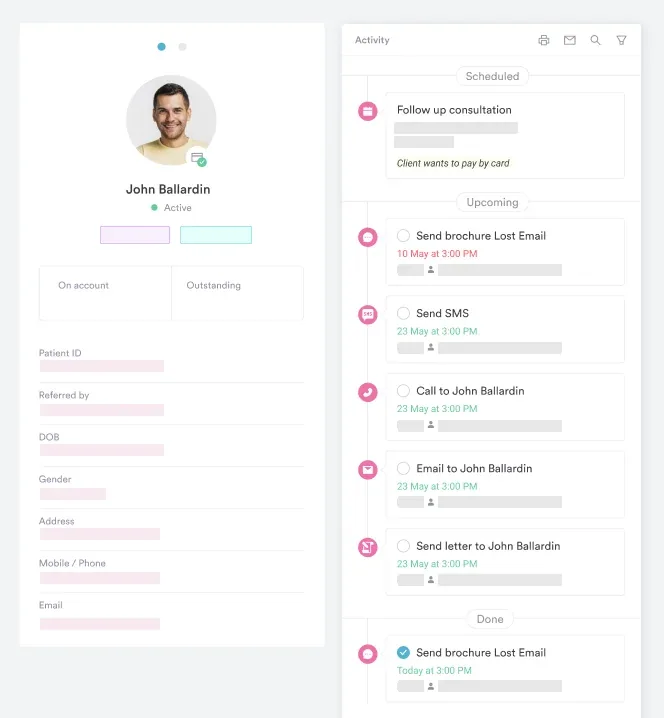
Pabau’s automated workflows route ACP templates to patients before the visit, collect responses through a secure intake form, and populate the clinician’s note at appointment time, so much of the documentation is done before the patient sits down.
A structured framework helps clinicians lead a goals of care conversation with confidence. The Serious Illness Conversation Guide from Ariadne Labs at Harvard provides validated language and example scripts, adapted below for primary care. Not sure who to offer it to? Use the “surprise question” clinicians rely on to prioritize: would you be surprised if this patient died within the next year? If the answer is no, book the visit.
Clinicians new to ACP conversations often worry about time burden. AI-assisted clinical documentation can reduce note-writing time by recording key points and structuring them into your EHR format, leaving the clinical conversation itself uninterrupted.
Use this checklist before, during, and after the visit to ensure billing compliance and documentation completeness.
Compliance management workflows help practices track ACP conversation completion and flag overdue discussions in high-risk populations (age >75, serious chronic illness).
Pabau’s practice management platform simplifies ACP visit workflows through customizable templates, automated patient intake, and structured note generation. Practices use Pabau to streamline the administrative burden while clinicians focus on the conversation.
Advance care planning discussion visits are a high-value, billable service that respects patient autonomy and reduces crisis decision-making. By using a structured template, scheduling dedicated time, and documenting comprehensively, practices can ensure that conversations are clinically sound and reimbursable. Download the template above and begin integrating ACP into your preventive care visits today.
See how Pabau's customizable templates and automated workflows reduce clinician burden and ensure billing compliance for advance care planning visits.

Need a structured clinical assessment tool? Psychiatric evaluation template provides a framework for documenting mental health assessments. Many ACP conversations include discussion of depression or anxiety impacts on goals of care.
Need to document what matters most to the patient? Quality of life assessment template captures a patient’s priorities before the visit, so the goals-of-care conversation starts from real information instead of assumptions.
Planning an ACP visit for a patient with a chronic condition? Diabetes nursing care plan template gives you a structured format for documenting ongoing chronic-disease management alongside advance care planning.
No. CMS imposes no frequency requirement for ACP visits. They’re patient-initiated or clinician-recommended based on clinical appropriateness (e.g., age, serious illness, major life transitions). Many practices recommend ACP to patients aged 65+, those with chronic conditions, or before elective surgeries.
CPT 99497 covers the first 30 minutes of an ACP discussion visit and is billable once face-to-face time reaches 16 minutes. CPT 99498 is an add-on for each additional 30 minutes, but it isn’t reportable until cumulative time reaches 46 minutes. A 50-minute visit would be billed as one unit of 99497 plus one unit of 99498: 99497 alone covers 16–45 minutes, and the 99498 add-on starts at 46 minutes.
Yes. When billed on the same day, both CPT 99497/99498 and AWV codes (G0438/G0439) are paid separately with zero cost-sharing for the patient. That’s a significant advantage for primary care practices offering both services during a comprehensive preventive visit.
Physicians, Nurse Practitioners (NPs), and Physician Assistants (PAs) can bill ACP codes depending on state scope-of-practice laws. Some states require NP/PA practice under physician supervision for billing, while others allow independent billing. Verify your state’s rules and your practice’s credentialing.
A completed ACP visit generates a clinical note documenting the discussion, a written summary to share with the patient, and ideally completion of an advance directive (living will) and healthcare proxy form. POLST/MOLST forms are completed if clinically appropriate and requested by the patient.
A POLST (Physician Orders for Life-Sustaining Treatment) form is a state-specific advance directive that translates a patient’s values into specific medical orders (e.g., do not resuscitate, comfort-focused care). Unlike a living will (which is a general statement of wishes), a POLST is a medical order that EMS and hospitals must follow. Not all patients need a POLST. Discuss it based on age and illness severity.
There is no ICD-10 code specific to advance care planning. Advance care planning is a service billed with CPT 99497/99498. The ICD-10 code you attach is the diagnosis that prompted the conversation, usually the patient’s relevant chronic or serious condition. For a standalone preventive discussion, practices often use a general counseling code such as Z71.89. Always code the clinical reason the visit took place.
An advance directive is a document that records your treatment wishes, while a healthcare power of attorney names the person who speaks for you when you cannot. Most complete plans include both: the directive states what you want, and the proxy decides on anything the document did not anticipate. During the visit, confirm the patient has named a surrogate decision-maker and that the proxy understands the role.