Doctor’s note for work
Download your free doctor’s note for work Doctor’s Note for Work A r...
Last Updated: July 27, 2026
Adson’s test is a provocative maneuver used to detect thoracic outlet syndrome by assessing subclavian artery compression.
High sensitivity (72-92%) but low specificity (9-53%) means it screens for TOS risk but cannot confirm diagnosis alone.
Combining Adson’s test with related maneuvers (Roos, Wright’s, Costoclavicular) and clinical history improves diagnostic accuracy.
Pabau’s digital forms and clinical record tools help physiotherapists document test findings and track vascular/neurogenic TOS patterns systematically.
A ready-to-use assessment form for documenting Adson’s test findings, including patient positioning, radial pulse assessment, positive/negative interpretation, and space for noting vascular vs. neurogenic TOS indicators.
Download templateAdson’s test is a clinical assessment maneuver used by physiotherapists, chiropractors, and sports medicine clinicians to screen for thoracic outlet syndrome (TOS). TOS occurs when nerves or blood vessels become compressed in the space between the collarbone and first rib.
The test involves palpating the radial pulse while the patient assumes a specific neck and arm position, then observing whether the pulse diminishes or disappears. A positive result suggests potential subclavian artery or brachial plexus compression, warranting further investigation with imaging and additional provocative maneuvers.
This clinical assessment template and reference guide covers the procedure step-by-step, interpretation criteria, sensitivity and specificity data from peer-reviewed research, and documentation fields for integrating findings into your practice workflow. Whether you document on paper or digitally, this guide ensures consistent, thorough TOS screening and helps clinicians differentiate between vascular and neurogenic presentations.
Adson’s test, also known as Adson’s maneuver, is a provocative test that temporarily narrows the interscalene triangle — the anatomical space bounded by the anterior and middle scalene muscles. Narrowing it lets you assess whether the compression affects blood flow through the subclavian artery or irritates the brachial plexus.
The test is named after Alfred Washington Adson, a pioneering neurosurgeon who first described it in 1927 as a clinical screening tool for TOS.
TOS encompasses three main types: vascular TOS (subclavian artery or vein compression), neurogenic TOS (brachial plexus compression), and disputed TOS (symptoms without objective vascular or neurological findings). Adson’s test primarily detects vascular TOS, though symptom reproduction (arm pain, tingling, or heaviness) may suggest neurogenic involvement.
The test is quick, non-invasive, and requires no special equipment. You only need to palpate the radial pulse and guide the patient through a standardized position.
Performing Adson’s test accurately requires attention to patient positioning, pulse palpation technique, and recognition of positive findings. The following steps ensure reproducible, clinically valid results.
Positive test result: Obliteration or significant diminution of the radial pulse, especially when accompanied by reproduction of the patient’s symptoms (arm pain, numbness, or heaviness), suggests positive findings. A positive pulse change alone, without symptom reproduction, is less clinically meaningful.
Understanding Adson’s test diagnostic accuracy helps clinicians interpret findings correctly and avoid over-reliance on a single screening tool.
| Diagnostic parameter | Finding | Clinical implication |
|---|---|---|
| Sensitivity | 72-92% | High ability to detect TOS when the condition is present; few false negatives |
| Specificity | 9-53% | Low ability to rule out TOS; frequent false positives in healthy volunteers and those with carpal tunnel syndrome |
| Positive predictive value | Low when used alone | A positive Adson’s test does NOT confirm TOS diagnosis in isolation |
| Combined maneuvers | Improved accuracy | Using Adson’s alongside Roos, Wright’s, and Costoclavicular tests increases diagnostic confidence |
Research published in PubMed Central shows that Adson’s test sensitivity ranged from 72% to 92%, while specificity was consistently low at 9-53%. High sensitivity paired with low specificity means the test is effective at flagging people at risk for TOS but cannot confirm the diagnosis on its own.
False positives are common in healthy volunteers and in patients with overlapping upper limb disorders such as carpal tunnel syndrome.
Predictive value improves significantly when Adson’s test is combined with other provocative maneuvers and when patients have confirmed cervical ribs (a structural risk factor for compression). Digital assessment forms that track multiple test results side-by-side help clinicians build a comprehensive TOS workup profile.
This assessment template is designed for healthcare professionals who evaluate upper extremity complaints and screen for thoracic outlet syndrome as part of their clinical practice.
Standardized assessment: A structured form ensures every Adson’s test is performed the same way and documented consistently, reducing variation between clinicians and improving data comparability over time.
Compliance and audit readiness: Physiotherapy and chiropractic practices face strict documentation requirements under state licensing board and professional practice standards. A standardized Adson’s test form demonstrates that your practice follows evidence-based assessment protocols and maintains thorough records for audit and complaint investigation.
Diagnostic confidence: By documenting radial pulse findings, symptom reproduction, and any related maneuvers performed in the same assessment session, you build a complete clinical picture that supports referral decisions, treatment planning, and billing for follow-up physical therapy re-evaluation.
Patient communication: A clear, signed consent form and assessment record demonstrate informed decision-making and provide the patient with a copy of their findings. That improves transparency and reduces misunderstanding about why further imaging or specialist referral is recommended.
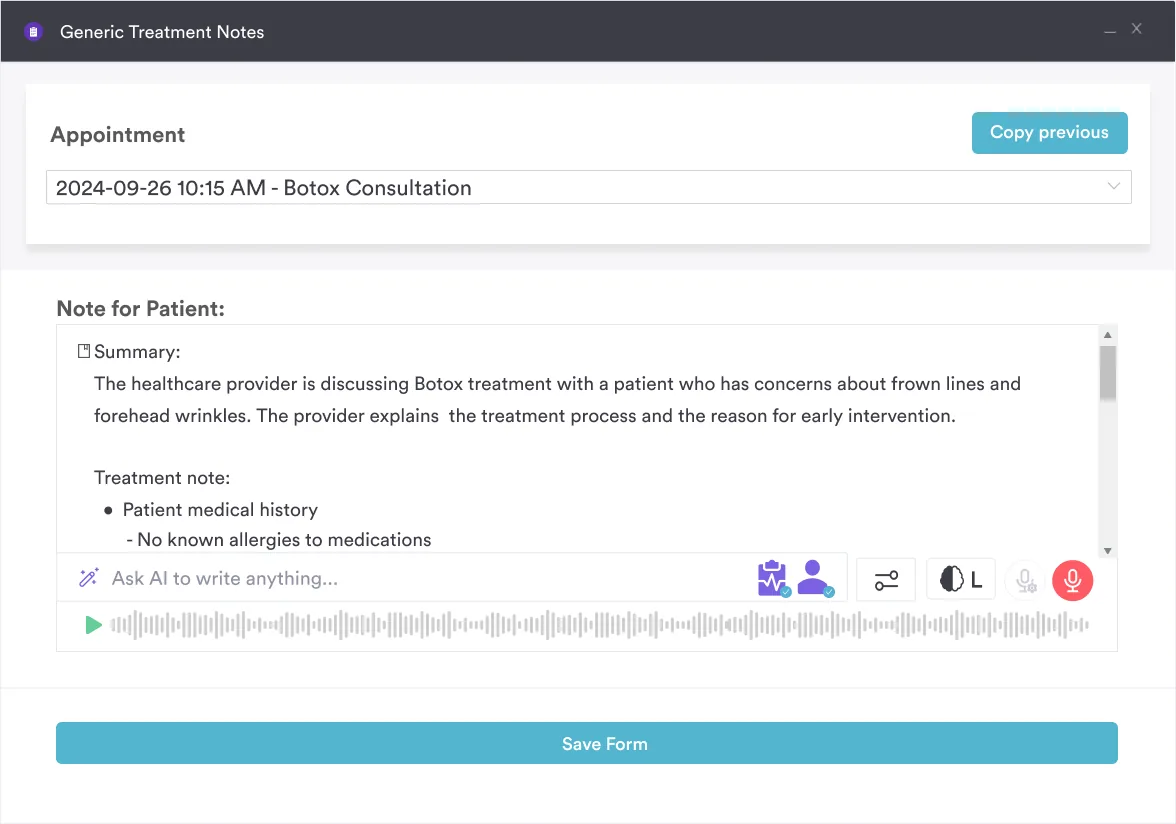
AI-assisted documentation: With practice management software like Pabau, you record Adson’s test findings in a structured client record, and Pabau Scribe, our AI scribe, turns your spoken assessment into a draft SOAP note. That means less time typing between patients and a consistent record for billing and referral.
No single test can diagnose thoracic outlet syndrome. Clinicians typically use multiple provocative maneuvers to increase confidence. Understanding how Adson’s test compares to related tests helps guide your assessment strategy.
The reverse Adson’s test, also called the Halstead maneuver, flips the head position. In the standard test the patient rotates the head toward the side being examined; in the reverse version the patient turns the head away from the tested side while the examiner extends the arm backward and monitors the radial pulse. Both narrow the thoracic outlet and look for the same positive sign: a diminished or absent radial pulse, with or without symptom reproduction.
Reach for the reverse test when the standard maneuver is negative but symptoms persist, or when a patient’s anatomy (such as a contralateral cervical rib) makes the standard head position unrevealing. Running Adson’s and reverse Adson’s in the same session and recording both results side by side gives a fuller picture of where the compression sits.
Combined testing protocols yield higher diagnostic confidence than any single maneuver. Working through the relevant tests in sequence and comparing the results is easier with clinical documentation software that keeps them side by side in one record.
Clinical documentation best practices for Adson’s test follow the same SOAP note structure used elsewhere in the chart, focusing on precision, consistency, and medico-legal clarity. Key fields to include:
Structured client records in modern EMR systems make this documentation faster and more consistent, keeping every test result, note, and referral in one patient timeline.
Adson’s test findings help differentiate between the two main TOS presentations. Understanding this distinction guides referral pathways and treatment decisions.
Documentation forms that distinguish these presentations help sports medicine clinicians and physiotherapists communicate clearly with referring physicians and specialists about the anatomical basis of symptoms.
Adson’s test remains a cornerstone screening tool for thoracic outlet syndrome in physiotherapy, chiropractic, and sports medicine practice. Its high sensitivity (72-92%) makes it effective for identifying individuals at risk, while its low specificity underscores the need for combined testing, imaging, and specialist referral to confirm diagnosis.
Using a standardized assessment form, especially one integrated into your EMR, ensures consistent and thorough documentation that supports clinical decision-making and meets professional compliance standards.
A structured approach to Adson’s test and related provocative maneuvers, supported by Pabau’s digital forms and clinical record tools, helps your practice screen for TOS confidently, differentiate vascular from neurogenic presentations, and refer patients appropriately to imaging or specialist care. Book a demo to see Pabau in action.
Need structured guidance on upper limb assessment protocols? Physical therapy EMR software helps physiotherapists organize and compare multiple provocative tests within a single patient record.
Want to improve your clinical documentation consistency? Digital forms for healthcare practices ensure every Adson’s test is documented the same way across your practice.
Looking to streamline TOS referral workflows? Automated workflow software can trigger specialist referral prompts when multiple TOS maneuvers are positive.
Adson’s test is a clinical assessment maneuver where the examiner monitors the radial pulse while the patient extends their neck, rotates the head toward the tested side, and depresses the shoulder. A positive result (pulse obliteration or diminution) suggests compression of the subclavian artery in the interscalene triangle, raising concern for thoracic outlet syndrome.
Pulse diminution or obliteration during Adson’s test suggests vascular TOS (subclavian artery compression). Symptom reproduction (arm pain, numbness, heaviness) strengthens the finding. However, a positive test alone cannot confirm TOS, because false positives are common — studies report them in roughly 9-20% of healthy volunteers, and more often in people with carpal tunnel syndrome. Combine results with other maneuvers and imaging for diagnostic confidence.
Adson’s test has sensitivity of 72-92% (good at detecting TOS when present) but specificity of only 9-53% (poor at ruling out TOS). This means high false-positive rates, making Adson’s an effective screening test but not a confirmatory test. Predictive value improves when combined with related maneuvers and imaging.
Seat the patient upright, locate the radial pulse, then ask them to extend their neck, rotate their head toward the tested side, and depress that shoulder. Monitor the pulse while the patient maintains this position for 30-60 seconds. Document whether the pulse remains strong, diminishes, or disappears, and note any symptoms the patient experiences.
Document baseline radial pulse, patient positioning (degree of head rotation, shoulder position, breathing technique), radial pulse response during the test, any symptom reproduction, and comparison with other TOS maneuvers performed. Include interpretation of findings (vascular vs. neurogenic TOS) and whether imaging or specialist referral is warranted.
No. Adson’s test is a screening tool, not a diagnostic test. Diagnosis requires combining Adson’s results with other provocative maneuvers (Roos, Wright’s, Costoclavicular), clinical history, imaging findings (ultrasound, MRA, angiography), and sometimes nerve studies (EMG/NCS). Use multiple tests to increase confidence before referring for specialist evaluation.
Yes. Adson’s test has low specificity, and studies report false positives in roughly 9-20% of healthy volunteers who show pulse diminution or obliteration without having TOS. Symptom reproduction during the maneuver is what makes a positive finding clinically meaningful, not the pulse change alone.
Adson’s test uses static positioning (neck extension and rotation with shoulder depression) to narrow the interscalene triangle. The Roos test (EAST) uses dynamic movement: the patient holds both arms abducted and externally rotated at 90 degrees and opens and closes the fists for three minutes. The Roos test is often more sensitive for activity-related compression, while Adson’s is faster to perform. Many clinicians use both together.
A positive Adson’s test alone does not justify imaging. Combine findings with Physiopedia’s TOS assessment framework: order ultrasound, MRA, or CT angiography for suspected vascular TOS, or MRI and EMG/NCS for suspected neurogenic TOS, only when symptom reproduction accompanies supporting findings from other maneuvers such as the Roos, Costoclavicular, or Wright’s tests.
The reverse Adson’s test turns the patient’s head away from the tested side while extending the neck and depressing the shoulder, the opposite rotation from the standard test. It can help identify TOS in patients with atypical anatomy, such as a cervical rib on the opposite side, when the standard maneuver does not reproduce symptoms.
Yes. The Halstead maneuver is another name for the reverse Adson’s test. The patient turns the head away from the tested side while the examiner extends the arm backward and palpates the radial pulse, the opposite head position from the standard Adson’s test. A diminished or absent pulse, especially with symptom reproduction, is a positive finding.