ICD-10 code S53.442D: UCL sprain of left elbow, subsequent encounter
ICD-10 code S53.442D is a valid, billable ICD-10-CM diagnosis code effective Oct...
Last Updated: August 10, 2026
HCPCS code J0670 covers injection of mepivacaine hydrochloride, billed per 10 ml administered – not per vial or per dose.
Medicare Part B reimburses J0670 under the buy-and-bill model using Average Sales Price (ASP) plus 6% methodology; rates update quarterly.
Missing or unsupported ICD-10 diagnosis codes are the most common reason J0670 claims are denied – always pair the code with a valid covered diagnosis.
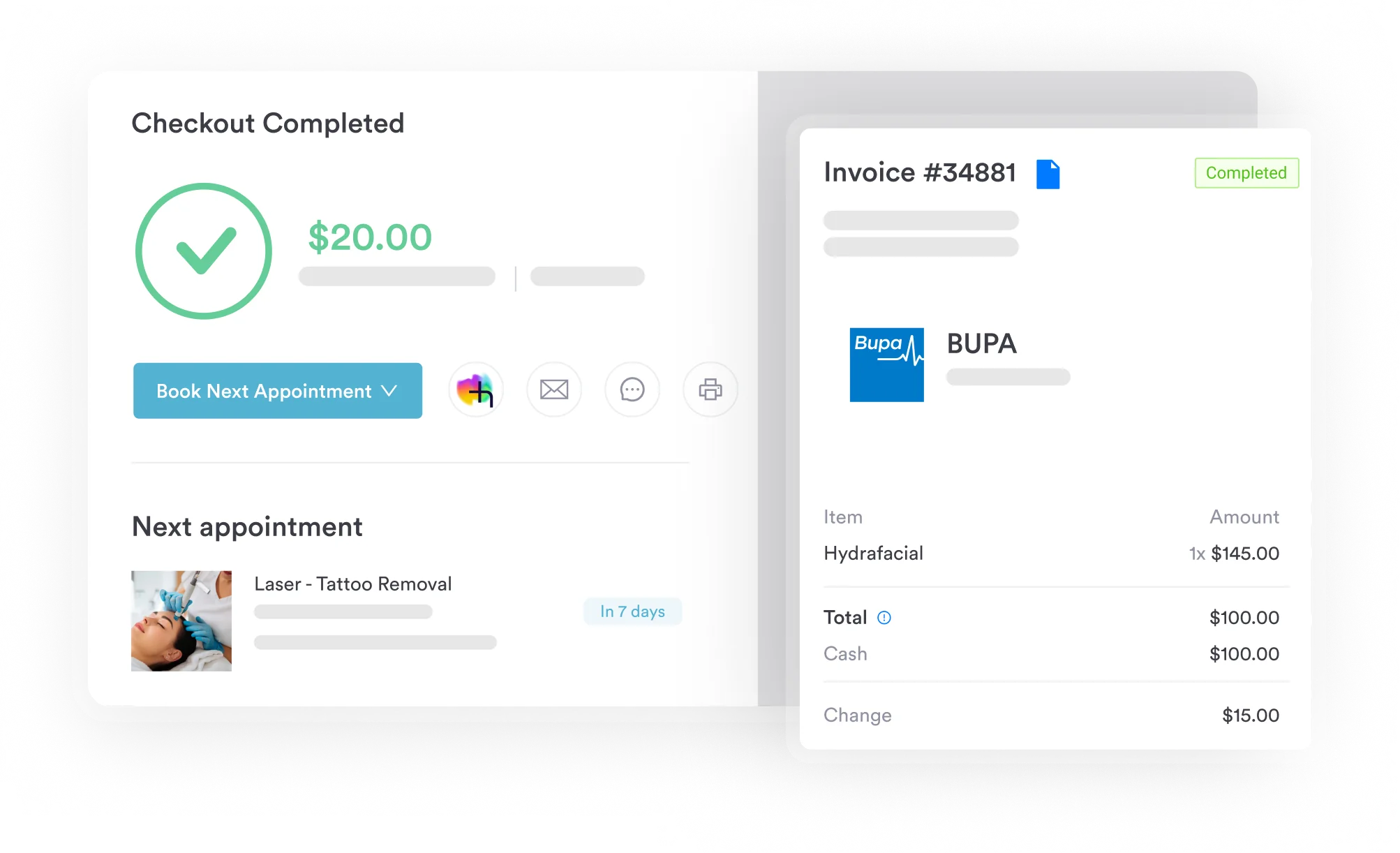
Pabau’s claims management software lets billers attach J-codes, units, modifiers, and ICD-10 codes directly to treatment records for clean claim submission.
Mepivacaine is one of the most routine injectable anesthetics in practice, and HCPCS code J0670 is just as often billed with a small mistake nobody notices until the remittance advice shows up. Get the unit count wrong, skip the waste modifier, or pair it with an unsupported diagnosis, and the claim gets denied.
Here is what determines whether that claim clears the first time.
HCPCS code J0670 covers the injection of mepivacaine hydrochloride, billed per 10 ml administered. Mepivacaine is a local anesthetic widely used for nerve blocks, epidural anesthesia, dental blocks, and infiltration procedures. The code is valid for fiscal year 2026 and is maintained by the Centers for Medicare and Medicaid Services (CMS) as part of the HCPCS Level II code set.
Mepivacaine hydrochloride is an amide-type local anesthetic that blocks nerve conduction by inhibiting sodium channel activity. Clinicians use it where a rapid onset and intermediate duration of action is needed. Common formulations are 1%, 1.5%, 2%, and 3% solutions.
The drug is marketed under the brand names Carbocaine and Polocaine. For billing purposes, the brand name does not change the code – all mepivacaine hydrochloride injections map to HCPCS code J0670 regardless of which manufacturer’s product is used.
Practices administering mepivacaine as part of IV therapy protocols can streamline documentation with IV therapy practice software that attaches drug details at the point of care.
Clinical contexts where J0670 applies include:
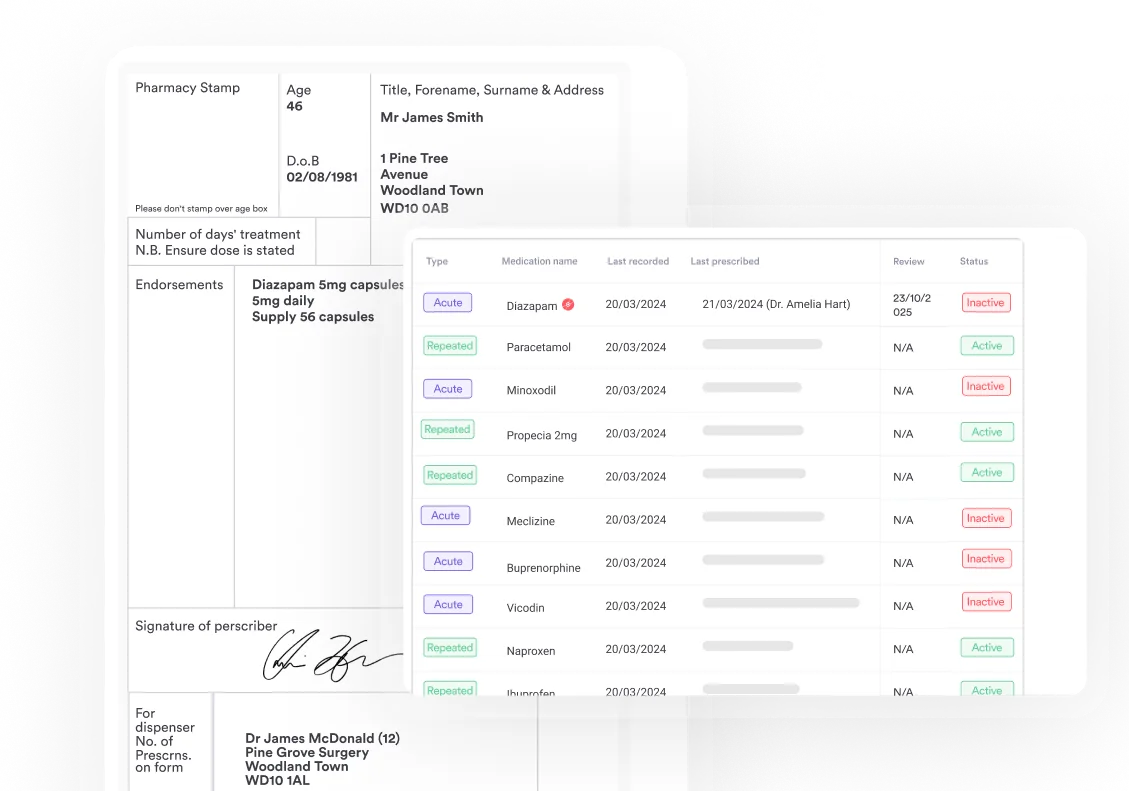
Practices that dispense or administer mepivacaine in-house under a buy-and-bill arrangement need robust prescription management tools to track drug lot numbers, expiration dates, and administered volumes – all of which feed into accurate unit billing.
The unit definition is central to accurate billing. J0670 is billed per 10 ml of mepivacaine hydrochloride actually administered to the patient – not per vial opened, not per concentration, and not per procedure.
Round the administered volume to the nearest 10 ml unit. Always document the exact volume drawn, administered, and wasted in the procedure note. CMS expects this documentation to support the unit count on the claim.
Using HIPAA-compliant billing workflows that link the drug administration record directly to the claim prevents the transcription errors that most commonly inflate or underreport unit counts.
Document the mepivacaine volume in millilitres in the procedure note at the time of administration, not at billing. Retrospective volume estimates are a common audit trigger – real-time recording protects the claim.
Medicare Part B covers J0670 as a separately payable drug under the physician-administered drug (buy-and-bill) model. The practice purchases mepivacaine, administers it to the patient, and bills Medicare for reimbursement after the fact.
Payment is calculated at ASP+6%: the Average Sales Price of the drug, as reported quarterly to CMS by manufacturers, plus a 6% add-on to cover acquisition and handling costs.
Because ASP is updated four times per year, the reimbursement rate for J0670 changes quarterly. Always verify the current rate against the CMS Physician Fee Schedule lookup tool before submitting claims for a new quarter.
Pabau’s claims management software supports electronic claim generation in the 837P format, letting billers attach J-codes, units, and modifiers directly to treatment records rather than re-entering data manually in a separate billing system.
Key Medicare coverage considerations for J0670:
The J0670 fee schedule rate is set by the CMS ASP quarterly pricing file. CMS publishes updated ASP files each quarter, typically effective January 1, April 1, July 1, and October 1. Specific dollar amounts change with each update and should not be treated as fixed.
For the most current J0670 allowable amount, use the AAPC HCPCS code lookup or the CMS fee schedule search. Both reflect the current Medicare allowable. Private payers typically negotiate their own rates, which may be above or below Medicare – always confirm with the individual payer contract.
Geographic payment locality adjustments (geographic practice cost indices, or GPCIs) do not typically apply to separately payable drug codes in the same way they do to physician work RVUs. The drug payment is primarily driven by the ASP file rather than locality modifiers.
Every J0670 claim requires a supporting ICD-10 diagnosis code that establishes medical necessity. Missing or non-covered diagnosis codes are the top denial driver for local anesthetic J-codes. The ICD-10 code should reflect the clinical reason the anesthetic was administered, not the drug itself.
Commonly paired ICD-10 diagnosis codes for J0670 include the following categories:
Check the applicable MAC’s LCD for J0670 or the procedure being performed. LCDs list covered diagnoses explicitly, and submitting a non-listed diagnosis code will result in denial. For panniculitis claims specifically, cross-check M79.3 against your MAC’s covered-diagnosis list before billing J0670 for the infiltration anesthesia used during treatment.
National Drug Code (NDC) reporting is required on Medicaid claims for physician-administered drugs. Each NDC is an 11-digit number identifying the specific drug manufacturer, product, and package size. When billing J0670 to Medicaid, you must report the NDC of the exact product administered, not a generic NDC for mepivacaine.
Mepivacaine hydrochloride is manufactured by several pharmaceutical companies. NDC codes change when manufacturers update packaging or discontinue products. Rather than relying on a static list, use the NLM Clinical Tables HCPCS API or the CMS NDC crosswalk file (updated quarterly) to confirm the current NDC-to-J0670 mapping for your specific product.
NDC reporting on Medicaid claims follows an 11-digit format (5-4-2): labeler code, product code, package code. Medicare does not require NDC reporting for J-codes, but Medicaid programs do – and some states impose additional state-level NDC requirements beyond the federal standard.
Pabau lets your billing team link J0670 units, modifiers, and ICD-10 codes to the patient's treatment record and generate clean 837P claims without switching between systems. No more manual copy-paste between your coding reference and your billing platform.

Modifiers adjust how a claim is processed. For J0670, two drug-waste modifiers and several procedural modifiers are most relevant. Using the wrong modifier – or omitting one that is required – is a common claim denial trigger.
The JW modifier has been required for discarded single-dose vial drugs since 2017. CMS introduced the JZ modifier on a different timeline: effective January 1, 2023 for optional use, mandatory from July 1, 2023, with non-compliant claims subject to rejection from October 1, 2023.
Under the current policy, practitioners must use JW for discarded drug from single-dose or single-use containers and JZ to attest to zero waste. Multi-dose vials follow different rules – waste from a multi-dose vial typically does not require a JW modifier. Confirm current guidance against your MAC’s local policy.
Practices managing these modifier decisions can benefit from reviewing med spa compliance requirements around documentation standards that apply to drug administration records.
J0670 denials cluster around a predictable set of errors. Most are avoidable with front-end workflow controls rather than back-end claim fixes.
Robust practice management software with built-in claim scrubbing catches most of these errors before the claim leaves the practice. Front-end edits – checking units, modifier presence, and ICD-10 linkage at the time of entry – are cheaper and faster than working denials after the fact.
For practices managing complex medical documentation workflows across multiple providers, structured claim templates tied to specific J-codes reduce variability and the risk of these common errors reaching the payer.
Run a pre-submission claim audit on all J0670 lines each month: check that every claim has (1) a units value derived from the documented administered volume, (2) a covered ICD-10 diagnosis, and (3) either JW or JZ modifier where a single-dose vial was used. This three-point check catches the majority of J0670 denials before they happen.
A clean J0670 claim depends on the same details being captured every time, not reconstructed after the fact. The requirements below pull together what CMS and most payers expect to see on the record before they will pay the claim.
Pabau’s digital forms capture this detail at the point of care, so the volume, modifier, and diagnosis code needed to support a J0670 claim already exist in the patient’s record before the claim is generated.
Mepivacaine is one of several local anesthetic drugs with their own HCPCS J-codes. Knowing the adjacent codes helps billers choose the correct code when the wrong drug is selected or when a procedure involves more than one anesthetic agent.
Never substitute J3490 for J0670 when billing mepivacaine. J3490 is an unclassified drug code reserved for drugs without a specific HCPCS code. Using it when J0670 exists signals incorrect coding and may trigger a medical review request.
CMS deleted J2001 for lidocaine effective October 1, 2024 and split it into three unit-specific codes, J2002, J2003, and J2004, so confirm which lidocaine code applies before billing it alongside J0670.
Practices billing mepivacaine alongside a base anesthesia code should also confirm the CPT descriptor matches the procedure performed – CPT 00529 shows how base units are assigned for anesthesia billed with a drug code like J0670.
Practices billing CPT 00770 or another anesthesia base code alongside J0670 should also check NCCI (National Correct Coding Initiative) edits to confirm the drug code and the procedural code are not bundled together for the specific service rendered.
Accurate billing for mepivacaine hydrochloride injections depends on three things: the right unit count (per 10 ml administered), a supported ICD-10 diagnosis, and the correct modifier for drug waste. Get any one of those wrong and the claim denies.
Pabau’s claims management software ties the administered drug volume, the diagnosis code, and any required modifiers directly to the patient’s treatment record, generating a clean 837P claim without manual data re-entry. If your billing team is spending time chasing J-code denials, book a demo to see how the end-to-end workflow reduces that rework.
Billing anesthesia alongside a drug code like J0670? CPT 00520 breaks down base units for closed-chest anesthesia procedures.
Need the CPT code for a vascular procedure under anesthesia? CPT 01272 covers billing for anesthesia during femoral artery procedures.
Coding anesthesia for a urologic procedure? CPT 00910 explains base units and modifiers for transurethral anesthesia.
HCPCS code J0670 is a Level II drug code for the injection of mepivacaine hydrochloride, billed per 10 ml administered. It covers all mepivacaine formulations regardless of brand name, including Carbocaine and Polocaine, and is used across nerve block, epidural, dental, and infiltration anesthesia procedures.
Bill one unit of J0670 for every 10 ml of mepivacaine hydrochloride administered to the patient. A 20 ml administration equals 2 units; a 30 ml administration equals 3 units. Always base unit count on the volume documented in the procedure note, not the vial size drawn.
Yes, Medicare Part B covers J0670 as a separately payable, physician-administered drug under the buy-and-bill model. Reimbursement is based on ASP+6% methodology, updated quarterly by CMS. A covered ICD-10 diagnosis code must support medical necessity on every claim.
Multiple NDC codes map to J0670 depending on the manufacturer, concentration, and package size of the mepivacaine hydrochloride product used. NDC codes change when manufacturers update products. Always use the CMS NDC crosswalk file or the NLM Clinical Tables API to confirm the current mapping for your specific product before submitting Medicaid claims.
Carbocaine and Polocaine are brand names for mepivacaine hydrochloride. All three refer to the same active ingredient. For billing purposes, the brand name does not change the HCPCS code: J0670 applies to all mepivacaine hydrochloride injections regardless of manufacturer or commercial name.
Modifier JW applies when drug is drawn from a single-dose vial and a remainder is discarded; modifier JZ applies when the entire drawn amount is administered with no waste. Modifier 59 applies when J0670 must be identified as a distinct service separate from a bundled anesthesia code. Modifier GA applies when a patient has signed an Advance Beneficiary Notice (ABN) and coverage is uncertain.
J0670 can be billed alongside anesthesia CPT codes only when mepivacaine is administered as a distinct, separately identifiable service not already bundled into the global anesthesia code. Check NCCI edits for the specific anesthesia CPT code billed on the same date of service before adding J0670 as a separate line item.