ICD-10 code S53.442D: UCL sprain of left elbow, subsequent encounter
ICD-10 code S53.442D is a valid, billable ICD-10-CM diagnosis code effective Oct...
Last Updated: August 10, 2026
CPT code 01272 describes anesthesia for femoral artery ligation procedures, classified under the upper leg arterial anesthesia range (01260-01274).
Base units for 01272 are 4 per the ASA Relative Value Guide. Total anesthesia payment uses the formula (Base Units + Time Units + Modifying Units) x Conversion Factor.
Modifiers AA, QZ, QK, and QX govern who provides and supervises the anesthesia. Payer rules on these modifiers vary, so verify each payer’s policy before billing.
Practice management software like Pabau helps anesthesia and surgical practices track CPT codes, attach correct modifiers, and reduce claim errors before submission.
CPT code 01272 is the anesthesia code for femoral artery ligation. It’s billed separately from the surgical procedure itself, using a dedicated anesthesia CPT code rather than the surgical code’s associated anesthesia value.
The code carries 4 base units under the ASA Relative Value Guide and sits within the 01260-01274 range for anesthesia on arteries of the upper leg, alongside codes for bypass grafts, embolectomies, and other femoral artery interventions. This reference covers the base unit calculation, applicable modifiers, Medicare rates, ICD-10 crosswalk, and documentation requirements needed to bill 01272 correctly.
Femoral artery procedures cover a clinically significant range: From femoral endarterectomy and femoral-popliteal bypass grafts to arterial access procedures and embolectomy. Understanding where CPT code 01272 fits within that range, and what documentation supports it, keeps claims clean on the first submission.
CPT code 01272 is the AMA’s designated code for anesthesia services provided during femoral artery ligation. The AMA maintains the CPT code set, and 01272 falls within the anesthesia section for arteries of the upper leg, covering femoral artery ligation specifically rather than other femoral artery interventions.
The official long descriptor reads: Anesthesia for procedures on arteries of upper leg, including bypass graft; femoral artery ligation. This descriptor is specific to femoral artery ligation. If the operative note describes a different femoral artery procedure, such as an embolectomy or a procedure not further specified, an adjacent code in the 01260-01274 range applies instead.
Anesthesiologists and CRNAs billing this code should confirm the procedure documentation explicitly identifies femoral artery ligation as the operative procedure. Vascular procedures on the upper leg can span multiple code options.
Selecting 01272 requires that the surgeon’s operative note documents ligation specifically, rather than a bypass graft, embolectomy, or an unspecified femoral artery intervention captured by an adjacent code in the 01260-01274 range.
The American Society of Anesthesiologists (ASA) assigns a base unit value to every anesthesia CPT code through its Relative Value Guide. For CPT 01272, the base unit value is 4.
Base units reflect the complexity of the procedure, patient positioning requirements, and the skill level the anesthesia service demands. They are fixed for the code regardless of how long the case runs.
Anesthesia reimbursement does not use a flat fee. It uses a formula that adds base units to time units, then multiplies the total by a conversion factor. The standard formula is:
(Base Units + Time Units + Modifying Units) x Conversion Factor = Total Allowed Amount
Time units are calculated at one unit per 15 minutes of anesthesia time. Anesthesia time starts when the anesthesiologist or CRNA begins preparing the patient for anesthesia and ends when they are no longer in personal attendance.
A 90-minute femoral artery procedure generates 6 time units (90 / 15 = 6). Modifying units apply when qualifying circumstances (such as emergency status or extreme patient age) add complexity.
The conversion factor itself varies by payer and geography. Medicare publishes an anesthesia conversion factor annually through the Physician Fee Schedule. Commercial payers negotiate their own rates separately.
Verify the current conversion factor with the CMS Physician Fee Schedule lookup tool for Medicare cases, and with each commercial payer’s fee schedule for contracted accounts.
For anesthesia base units and conversion factors specifically, consult the ASA Relative Value Guide or the CMS anesthesia-specific fee schedule directly. General RVU lookup tools such as FastRVU cover standard surgical CPT codes only, and do not publish anesthesia base units.
Anesthesia modifier selection signals who is providing the service and the supervision arrangement in place. Billing CPT 01272 without the correct modifier is one of the most common reasons anesthesia claims fail on first pass. Four modifiers apply most frequently.
When a QK/QX team arrangement is used, the anesthesiologist bills with QK and the CRNA bills with QX on the same procedure. Medicare pays 50% to each provider in that model.
State rules on CRNA supervision vary. Some states allow CRNAs to practice without physician oversight, which affects whether QZ or QX applies. Verify the applicable state opt-out status and payer-specific modifier rules before billing, as commercial payers may not follow Medicare’s model exactly.
For a broader reference on how CPT code billing applies across service lines, our coaching CPT code guide covers the modifier framework in comparable detail.
Document the supervision arrangement in the anesthesia record before closing the chart. Modifier errors on anesthesia claims are audit flags. Note the exact start and end times of anesthesia, the name of the supervising physician (if applicable), and the total time in minutes so your billing team can calculate time units accurately.
Anesthesia reimbursement is not a single number. The total allowed amount depends on the payer, the geographic area, the modifier used, and the case duration. What CMS publishes is the anesthesia conversion factor, which is the dollar value applied to each anesthesia unit in the billing formula. The conversion factor changes annually with the Medicare Physician Fee Schedule.
Medicare applies a national base anesthesia conversion factor, adjusted for geographic practice cost differences using the Geographic Practice Cost Index (GPCI). The formula the Centers for Medicare and Medicaid Services uses is:
Payment = (Base Units + Time Units) x (Conversion Factor x GPCI)
Because the conversion factor and GPCI values change each calendar year, no fixed dollar amount should be stated here without citing a current CMS source. Billing teams should pull the current-year anesthesia conversion factor directly from the CMS Physician Fee Schedule lookup tool and apply the relevant GPCI for the facility’s location.
Commercial payer rates typically exceed Medicare rates for anesthesia services, though this varies by contract. Always confirm contracted rates with each payer separately and never apply the Medicare conversion factor to commercial claims without verification.
Every anesthesia claim requires a supporting diagnosis code that justifies the medical necessity of the procedure. For femoral artery cases billed under CPT 01272, the ICD-10-CM diagnosis code should reflect the underlying condition requiring surgery. These are the most common diagnosis code categories paired with this procedure.
I74.3 covers non-septic arterial embolism and thrombosis of the lower extremities, the code most often paired with 01272 for a femoral embolectomy. A septic arterial embolism is coded differently, under I76, and should not be substituted for I74.3 on a routine femoral artery claim.
The ICD-10-CM code must match the surgeon’s documented primary diagnosis, not a secondary or incidental finding. For peripheral artery disease cases, laterality matters: Codes differ for right versus left extremity involvement. Unspecified laterality codes (ending in 9) are acceptable only when the operative note genuinely does not specify the side, though payers may query these.
Confirm the crosswalk between the surgical CPT code and the ICD-10 diagnosis code is medically justified. Payers use automated edits to flag mismatched procedure-diagnosis combinations. A femoral artery anesthesia claim paired with a diagnosis that does not involve the lower extremity vasculature is likely to deny on medical necessity grounds.
Review ICD-10 crosswalk resources and payer-specific Local Coverage Determinations (LCDs) before submission. The AAPC Codify lookup tool provides crosswalk lookups between CPT and ICD-10 codes.
Anesthesia claims have documentation requirements that differ from standard surgical or evaluation and management (E/M) claims. Missing or incomplete anesthesia records are among the most frequently cited compliance issues in anesthesia billing audits. The anesthesia record must support the entire claim.
HIPAA-compliant record retention applies to anesthesia records. For practices managing anesthesia documentation across multiple cases and providers, HIPAA compliance standards outline the safeguards required for storing and transmitting patient records. Structured digital documentation reduces the risk of missing fields that trigger claim review.
Practices should also review the HIPAA compliance checklist to ensure documentation workflows meet federal requirements. Pabau’s digital forms feature lets practices build structured anesthesia record templates that capture all required fields automatically, reducing missing fields in post-case documentation.
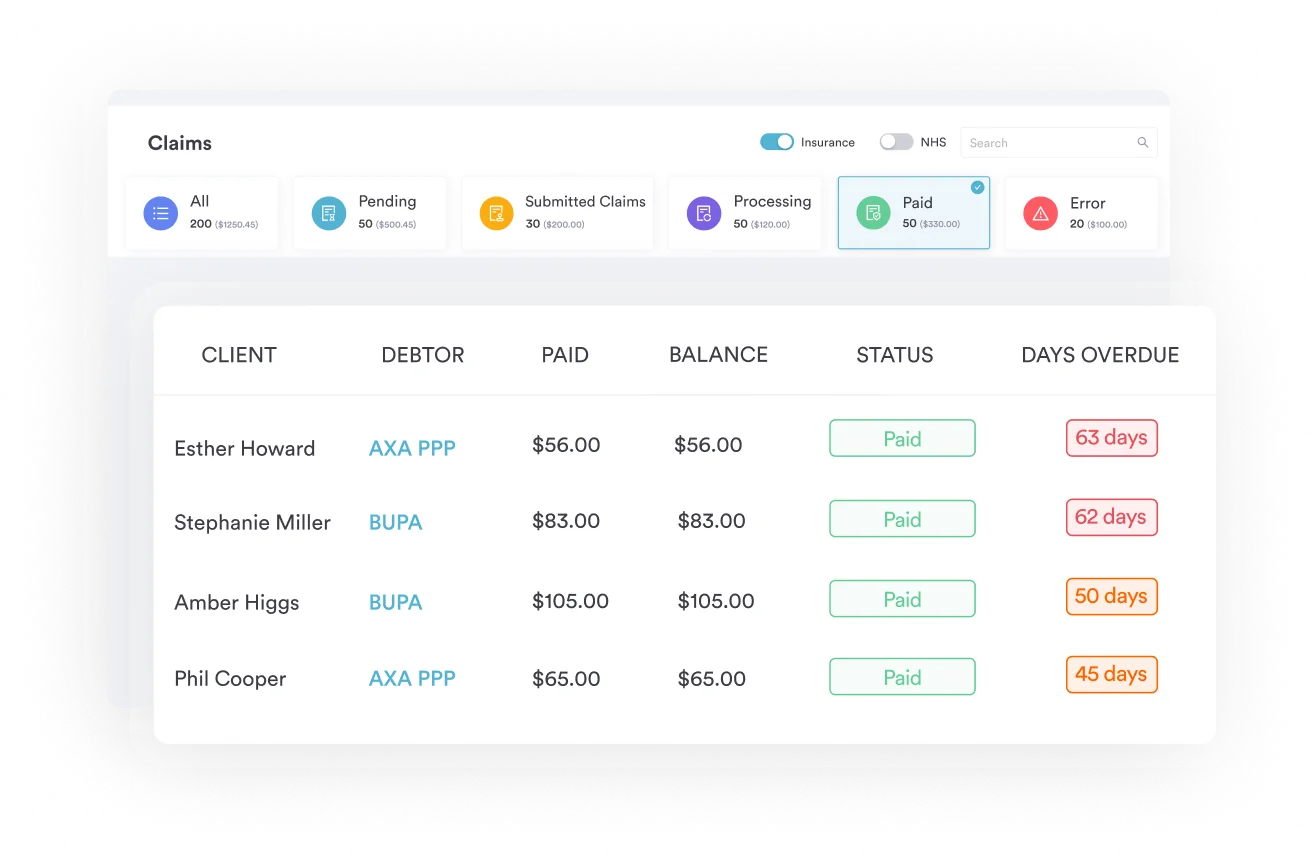
Pabau's claims management tools help surgical and anesthesia practices attach the right CPT codes, modifiers, and documentation to every claim. Fewer denials. Faster reimbursement.

The 01260-01274 range contains several codes for upper leg arterial anesthesia. Choosing the correct code requires matching the specific surgical procedure to the code descriptor. Below is a decision guide for the most commonly confused adjacent codes.
The key distinction between 01270, 01272, and 01274 is not whether the femoral artery is named, but which specific procedure was performed on it. All three codes sit within the upper leg arterial anesthesia range and can involve the femoral artery.
Use 01272 when the operative report documents femoral artery ligation, use 01274 when it documents femoral artery embolectomy, and reserve 01270 for an upper leg arterial procedure that is not further specified by a more precise code. Confusing these codes is an easy way to misstate both the procedure performed and the base units on a claim.
Popliteal artery procedures fall outside this range entirely. They are billed under a separate lower-leg anesthesia family, including 01444 for popliteal artery repair and 01500 for other lower-leg arterial procedures, not under 01270-01274.
For broader context on CPT code selection in procedures involving vascular access, the IVF CPT codes guide covers a comparable approach to choosing between adjacent codes for clinical procedures.
Practices working with plastic surgery or reconstructive vascular cases may also find Pabau’s plastic surgery EMR resources relevant to managing procedure documentation across complex surgical cases. Practices that combine surgical recovery with rehabilitation services may also find Pabau’s physical therapy EMR tools useful for coordinating post-operative care documentation.
Anesthesia billing depends on accurate time capture, correct modifier assignment, and complete documentation in the anesthesia record. When any of those elements are missing or inconsistent, the claim fails. Practices managing high-volume vascular or surgical caseloads need a system that connects clinical documentation to the billing workflow without manual data transfer between the two.
Pabau’s claims management software allows anesthesia and surgical practices to attach CPT codes and modifiers at the point of documentation, reducing the transcription errors that generate modifier mismatches. Digital forms capture structured anesthesia record data, including start and stop times, ASA status, and provider details, in a format that flows directly into the billing record.
For practices that have expanded to multiple surgical sites, the multi-location management feature keeps documentation and billing organized across all sites from a single platform.
For practices managing anesthesia-adjacent workflows, including pre-operative assessments and post-procedure care documentation, Pabau’s client record management tools maintain a complete audit-ready patient record. The practice management software framework that underlies these features connects scheduling, documentation, and billing in one system, so the anesthesia record, the operative note, and the claim are always aligned.
Billing CPT code 01272 correctly requires more than knowing the descriptor. The base unit value, the time unit formula, the right modifier for the supervision arrangement, and a matched ICD-10 diagnosis code all have to align before the claim reaches the payer. Errors at any of those points generate denials that take time and resources to resolve.
Pabau’s claims management tools help anesthesia and surgical teams build those elements into the documentation workflow, not bolt them on after the fact.
If you want to see how structured CPT code and modifier management fits into a complete practice workflow, explore Pabau’s automated workflows or speak with the team about how Pabau handles anesthesia billing documentation for your case volume.
Need a reference for related anesthesia CPT coding? IVF CPT codes billing guide covers how adjacent CPT codes are structured for procedural anesthesia and surgical services.
Need a reference for an adjacent anesthesia code? 01440 covers anesthesia for knee and popliteal artery procedures, immediately adjacent to the femoral artery range.
Looking for a structured overview of CPT billing workflows? Coaching CPT codes reference explains how CPT code selection, modifiers, and billing formulas apply across service categories.
CPT code 01272 is the anesthesia code for femoral artery ligation. It falls within the 01260-01274 range for anesthesia on arteries of the upper leg and carries 4 ASA base units. Use it when the operative documentation clearly identifies femoral artery ligation as the procedure performed. A different code in the range applies if the femoral artery procedure is a bypass graft, embolectomy, or not otherwise specified.
CPT 01272 has 4 base units per the ASA Relative Value Guide. These are added to time units (one unit per 15 minutes of anesthesia time) and any modifying units to calculate the total number of anesthesia units before applying the payer’s conversion factor.
The four primary modifiers are AA (anesthesiologist personally performed the service), QZ (CRNA without physician direction), QK (anesthesiologist directing 2-4 concurrent CRNA cases), and QX (CRNA under physician medical direction). The correct modifier depends on who provided the anesthesia and the supervision arrangement. Verify each payer’s specific requirements before billing.
Use the formula: (Base Units + Time Units + Modifying Units) x Conversion Factor. For CPT 01272, base units are 4. Time units are calculated at one per 15 minutes of anesthesia time. The conversion factor is set annually by CMS for Medicare and negotiated separately by each commercial payer. Check the current CMS Physician Fee Schedule and apply geographic adjusters for your facility location.
Qualifying circumstance codes 99100 (extreme age, under 1 or over 70) and 99140 (emergency conditions) may apply when clinically documented. Coverage for these codes varies by payer. Not all commercial plans reimburse them. Document the clinical basis clearly in the anesthesia record before appending either code to the claim.
Yes. A CRNA can bill CPT 01272 using modifier QZ when performing the service without physician direction, or modifier QX when under physician medical direction. State-level opt-out rules determine whether CRNAs in a given state can practice without physician supervision, which affects modifier selection. Confirm your state’s opt-out status and each payer’s policy before billing.