








HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
HCPCS code G2212 is the Medicare-specific add-on code for prolonged office or outpatient E/M services beyond the maximum time of CPT 99205, 99215, or 99483
G2212 triggers when total physician time exceeds the level-5 E/M threshold by at least 15 minutes, and can be billed in additional 15-minute increments
Medicare uses G2212 where commercial payers typically require CPT 99417 instead; verify per payer contract before billing
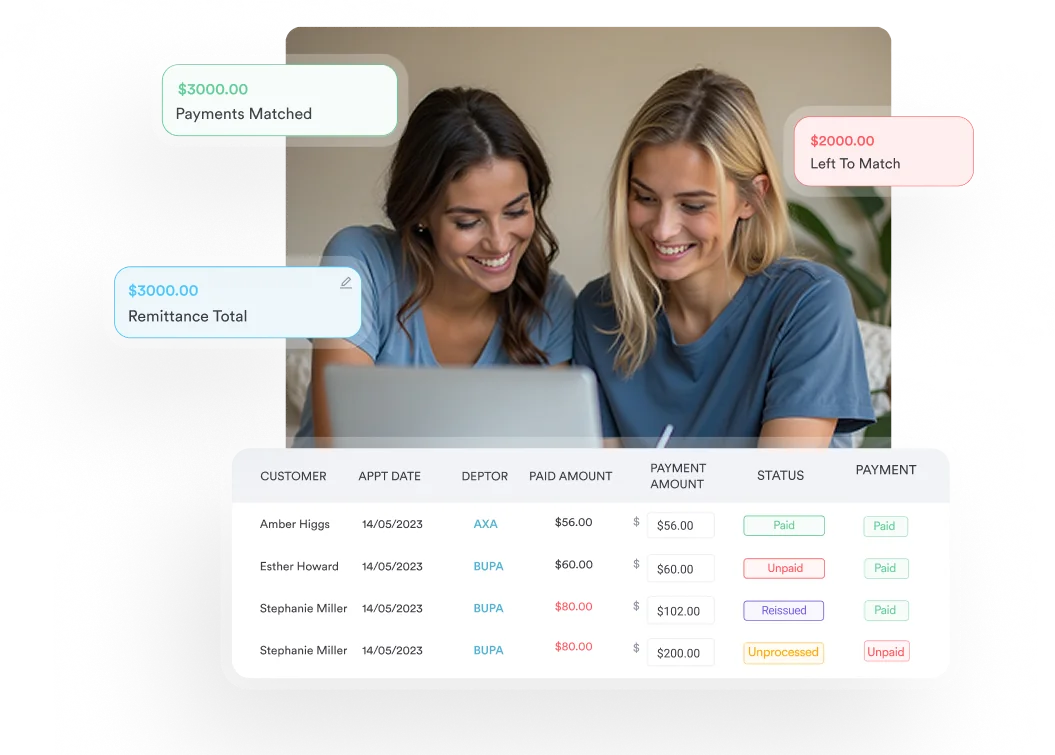
Practice management software like Pabau, with built-in claims management, validates claims before submission and tracks their status — catching coding errors on complex add-on codes like G2212 before they cause denials
According to the Centers for Medicare and Medicaid Services (CMS), HCPCS code G2212 covers prolonged office or other outpatient evaluation and management services beyond the maximum required time of the primary procedure, billed per each additional 15 minutes by the physician or qualified healthcare professional, with or without direct patient contact.
It lists separately in addition to CPT codes 99205, 99215, and 99483.
CMS introduced G2212 in the 2021 Medicare Physician Fee Schedule final rule. The code replaced the older prolonged service codes (99354, 99355, 99358, 99359) for outpatient settings, aligning with the 2021 E/M revisions that shifted level selection to total physician time rather than face-to-face time alone.
Practices that use claims management software to validate claims before submission are better positioned to catch documentation issues on these encounters before they reach the payer.
G2212 does not apply to every long appointment. It activates only after the physician has already hit the maximum required time for the highest level E/M visit and then surpassed that threshold by at least 15 minutes on the same date of service.
The time thresholds for the primary codes that anchor G2212 are:
Each additional complete 15-minute block beyond the trigger point supports one additional unit of G2212. A 99205 visit running 104 minutes, for instance, would support two units of G2212 (89-103 minutes = 1 unit; 104 minutes and above = 2 units).
Noridian Healthcare Solutions, a Medicare Administrative Contractor, confirms that the G2212 clock runs on total physician time on the date of service, not just face-to-face encounter time.
That includes pre-visit review, documentation, care coordination — such as arranging home safety DME like a bath tub wall rail (HCPCS code E0241) for an at-risk patient — and post-visit tasks performed that day. Physicians billing Medicare through a primary care EHR should confirm that their system captures all-day time, not just appointment slot duration.
Document start and end times for each activity segment on the date of service, including pre-visit chart review, shared decision-making, and post-visit documentation. Auditors reviewing G2212 claims want a total-time narrative, not a single timestamp. A brief time log in the note prevents denials before they happen.
One of the most common billing questions around G2212 is whether to use it or CPT code 99417. The answer depends entirely on who the payer is.
The American Medical Association (AMA) maintains CPT 99417, while CMS maintains HCPCS code G2212 through the annual Medicare Physician Fee Schedule rulemaking process. Both cover the same clinical scenario: prolonged time beyond the level-5 threshold. The split exists because CMS chose not to adopt the AMA’s code when it revised E/M coding in 2021.
Practices managing both Medicare and commercial payer contracts through a practice management platform should configure payer-specific billing rules to route G2212 to Medicare claims and 99417 to commercial claims automatically. Manual routing is a common source of denials in mixed-payer environments.
G2212 and G2211 are both add-on codes appended to office and outpatient E/M visits, but they capture different clinical scenarios. Confusing them leads to either underbilling or claim rejection.
G2211 is the complexity add-on code. It accounts for the ongoing relationship and inherent complexity of being the continuing, responsible clinician for a patient with serious, complex conditions. It does not require additional time beyond the primary E/M threshold.
HCPCS code G2212 is the time add-on code. It captures documented extra minutes beyond the maximum required time of a level-5 visit. It does not depend on relationship continuity or condition complexity alone.
The American Academy of Ophthalmology and the AAPC have both noted that G2211 and G2212 can theoretically be billed together on the same date of service when both clinical criteria are met, but practices should confirm their MAC’s current guidance before doing so.
Some local coverage determinations may restrict simultaneous billing. Physicians in specialties with complex chronic patient panels, such as endocrinology or psychiatry, are most likely to encounter situations where both codes apply. For psychiatry-specific billing context, see psychiatry EMR software considerations.
Pabau's claims management software validates claims before submission and tracks their status, helping practices catch coding errors on complex claims like G2212 before they go out the door.

HCPCS code G2212 is one of the codes auditors scrutinize most closely in E/M billing reviews. Claims without adequate documentation are the primary driver of post-payment audits and recoupment requests.
At minimum, the clinical note must support:
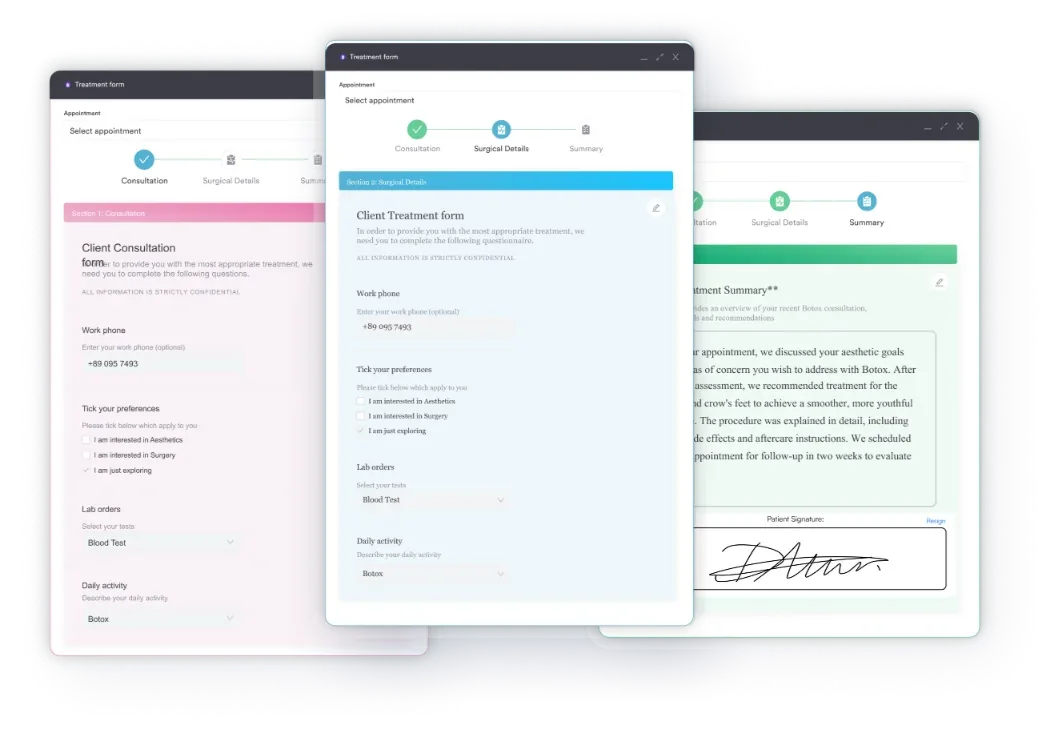
Practices using digital forms and structured note templates can build time-capture fields directly into visit workflows, closing common documentation shortfalls before billing. Pairing structured templates with medical billing software built for US billing workflows keeps clinical documentation and claims submission in sync.
The note does not need to be exhaustive, but it does need to answer an auditor’s two core questions: how long the visit took, and why?
The official HCPCS code G2212 descriptor includes explicit exclusions. Billing G2212 on the same date of service as any of the following codes will result in a claim edit or denial:
These restrictions exist because G2212 replaced the older prolonged service framework for outpatient settings. Submitting G2212 alongside any of these legacy codes creates a duplicate billing conflict under HIPAA billing regulations.
There are also setting restrictions. HCPCS code G2212 applies only to office and other outpatient E/M services. It does not apply to inpatient, observation, emergency department, or nursing facility visits. The place of service code on the claim must reflect an office or outpatient setting for G2212 to be reportable.
HCPCS code G2212 may be reported by physicians and qualified healthcare professionals (QHPs). Clinical staff time does not count toward the G2212 threshold. CPT codes 99415 and 99416 cover clinical staff prolonged time under direct supervision, but those codes cannot be billed on the same date as G2212.
Nurse practitioners and physician assistants billing under their own NPI as qualified healthcare professionals can report G2212 when they independently provide and document the prolonged service time.
Incident-to billing arrangements, where services are reported under the supervising physician’s NPI, have additional requirements and should be confirmed with the relevant MAC before billing. For practices employing NPs and PAs, a nurse practitioner private practice guide covers billing structure considerations in more detail.
Flag every encounter where total physician time reaches 60 minutes for a 99215 visit or 80 minutes for a 99205 visit. That gives your billing team a 9-14 minute buffer to confirm whether the documentation supports G2212 before the claim goes out. Catching borderline cases at coding time costs far less than post-payment audits.
According to the CMS Physician Fee Schedule lookup tool, reimbursement for HCPCS code G2212 is determined annually through the Medicare Physician Fee Schedule (MPFS) and varies by geographic location based on the applicable conversion factor and locality-specific RVU adjustments.
National average rates fluctuate year to year as CMS updates work RVU values, practice expense RVUs, and the conversion factor. Practices should verify the current rate for their MAC jurisdiction directly through the CMS fee schedule lookup rather than relying on static figures, which can be outdated within months of publication.
The AAPC Codify HCPCS lookup provides a useful cross-reference for verifying code status, code history, and associated coverage notes alongside fee schedule data.
California workers’ compensation is a notable special case. California’s Division of Workers’ Compensation has required HCPCS code G2212, instead of CPT 99417, for extended E/M time since 2021.
The time thresholds mirror the Medicare framework. Practices in California billing workers’ comp should confirm current fee schedule rates with the California Division of Workers’ Compensation, as MPFS rates do not automatically apply to workers’ comp.
The single most common reason G2212 claims are denied or underbilled is incomplete time documentation at the point of care. Physicians rarely track their time with billing in mind during a complex visit, and by the time the note is finalized, the precise time split across activities is gone.
This kind of documentation lag is a common bottleneck in healthcare revenue cycle management, and one that costs practices reimbursement over a year.
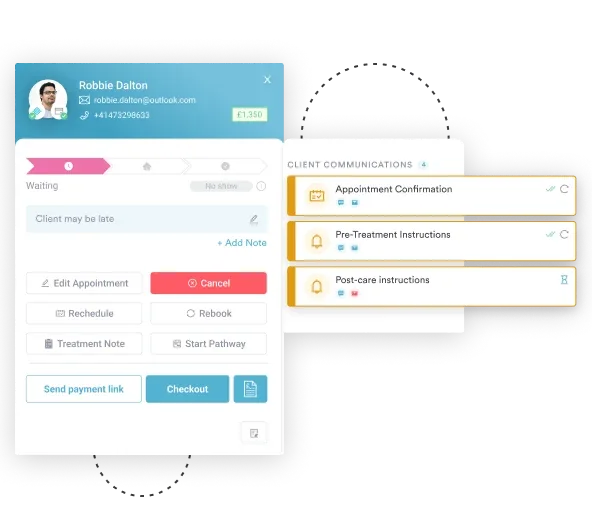
Purpose-built automated workflow tools can prompt physicians to confirm total visit time before a note is signed, capturing the data at the moment it is most accurate. Structured note templates can include required fields for time documentation, preventing the note from being completed without a time entry.
For practices exploring how to systematize their billing infrastructure, a medical practice business plan framework can help map which billing workflows need tool support.
Pabau’s claims management software validates claims against payer requirements before submission, flagging missing details like authorization codes so errors get caught before a claim goes out.
A live claims dashboard tracks each submission’s status — pending, submitted, processing, paid, or rejected — which helps billing teams catch coding mistakes on complex claims, including G2212, before they turn into denials.
Practices with complex billing needs, including multi-specialty groups handling psychiatry, endocrinology, and primary care, also benefit from HIPAA compliance checklists for primary care to ensure documentation workflows meet both billing and regulatory standards.
Prolonged visits represent time-intensive physician work. HCPCS code G2212 exists to ensure Medicare pays for that work, but only when the documentation holds up under scrutiny. The code activates at a precise time threshold, carries explicit exclusion rules, and requires time-specific documentation that most standard note templates do not capture by default.
Practices that build G2212 awareness into their billing workflows and use structured documentation tools recover revenue that would otherwise slip through.
To see how Pabau’s claims management software validates claims before submission and tracks their status through to payment, explore how private practices benefit from integrated billing tools, or review Pabau’s claims management software in detail.
Need a full overview of medical billing workflows? Practice management software features covers the core tools that support accurate claims submission and revenue cycle management.
Billing across multiple specialties? Coaching CPT codes illustrates how add-on code logic applies across different clinical service categories.
Want to improve compliance across your billing documentation? Medical forms at your healthcare practice explains how structured digital forms reduce missing documentation that leads to claim denials.
Working with UK private healthcare claims? CCSD code 0001B covers billing under the UK’s private coding system.
HCPCS code G2212 is the Medicare-specific add-on code for prolonged office or outpatient E/M services beyond the maximum required time of CPT codes 99205, 99215, or 99483. It is reported in addition to the primary E/M code for each additional 15-minute increment of physician time that exceeds the level-5 visit threshold on the date of service.
G2212 is used for Medicare Part B billing; CPT 99417 is used for most commercial payers. Both codes cover the same clinical scenario, prolonged outpatient E/M time beyond the level-5 threshold, but CMS created G2212 as a Medicare-specific alternative when it revised E/M coding in 2021. Submitting CPT 99417 to Medicare will result in a denial.
Yes. HCPCS code G2212 can be billed in multiple units on the same date of service, with each unit representing a complete additional 15-minute increment of physician time beyond the primary E/M threshold. Documentation must support the total time across all units claimed.
No universal modifier is required for HCPCS code G2212. However, individual Medicare Administrative Contractors (MACs) may have local coverage determinations that require a modifier in specific circumstances. Always verify with your MAC’s current guidance before submitting claims.
G2211 (the visit complexity add-on) and G2212 (the prolonged time add-on) can be reported on the same date of service when both sets of criteria are independently met. G2211 addresses the complexity of an ongoing care relationship; G2212 addresses documented extra time beyond the level-5 threshold. Confirm your MAC does not restrict simultaneous billing before submitting both.



